Download as pdf or txt
You might also like
- Science5 - q2 - Mod3 - Modes of Reproduction in Animals - v4Document23 pagesScience5 - q2 - Mod3 - Modes of Reproduction in Animals - v4Nellen Grace Ortiz84% (25)
- TOG 2021 Volume 23 Issue 2Document72 pagesTOG 2021 Volume 23 Issue 2Lakshmi DheviNo ratings yet
- The Problem and Its Background: Republic of The Philippines Landy National High School Landy, Santa Cruz, MarinduqueDocument29 pagesThe Problem and Its Background: Republic of The Philippines Landy National High School Landy, Santa Cruz, MarinduqueIvy Rose Plata100% (1)
- Closing The Loop Patient SafetyDocument34 pagesClosing The Loop Patient SafetyVirginia Abalos0% (1)
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- Forceps Delivery For Gravidocardiac PatientsDocument80 pagesForceps Delivery For Gravidocardiac PatientsTots A. Macahilo-LayawonNo ratings yet
- Hypothyroidism Pregnancy BrochureDocument2 pagesHypothyroidism Pregnancy BrochureNungky KusumaNo ratings yet
- UTI On A Background of Obstructive NephropathyDocument26 pagesUTI On A Background of Obstructive NephropathyAminath MeesanNo ratings yet
- Physiologicalchangesinpregnancy 170323142156Document69 pagesPhysiologicalchangesinpregnancy 170323142156madhu.B100% (1)
- Abnormal Uterin ActionDocument65 pagesAbnormal Uterin Actionshweta raiNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- Ectopic Pregnancy PDFDocument38 pagesEctopic Pregnancy PDFByron Ruiz Lapuerta100% (1)
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Shubrat Singh: EctopicDocument25 pagesShubrat Singh: Ectopicshubham royalNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Caesarean Scar Ectopic Pregnancy: Case ReportDocument3 pagesCaesarean Scar Ectopic Pregnancy: Case ReportDewi SaftariNo ratings yet
- AbortionDocument67 pagesAbortionaneley cherinetNo ratings yet
- Guidelines For Management of Endometrial CarcinomaDocument41 pagesGuidelines For Management of Endometrial CarcinomaVeenaNo ratings yet
- 4-. Revision Notes of Lecture OneDocument104 pages4-. Revision Notes of Lecture OneHasan DahamshehNo ratings yet
- POP June 10,2021 1Document48 pagesPOP June 10,2021 1Kerod AbebeNo ratings yet
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborDocument10 pagesE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALINo ratings yet
- Normal and Abnormal PeurperiumDocument62 pagesNormal and Abnormal PeurperiumMOHAMED AZIZNo ratings yet
- Vaginal Bleeding in Pregnancy - 5-Minute Emergency ConsultDocument6 pagesVaginal Bleeding in Pregnancy - 5-Minute Emergency ConsultLaoMed plusNo ratings yet
- Jaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TDocument35 pagesJaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TSerge TresorNo ratings yet
- The Role Ultrasound in Early PregnancyDocument167 pagesThe Role Ultrasound in Early PregnancyCordova ArridhoNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Nancy E Fay MD Facog Division of Reproductive MedicineDocument32 pagesNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNo ratings yet
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- MRCOG Part 2 - March 2015 Recalls.: StatisticsDocument10 pagesMRCOG Part 2 - March 2015 Recalls.: StatisticsAmanda RahmawatiNo ratings yet
- Breech PresentationDocument29 pagesBreech PresentationSrikitta DanieliaNo ratings yet
- Genital FistulaeDocument15 pagesGenital Fistulaesangeetha francisNo ratings yet
- Deep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateDocument11 pagesDeep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateGabyta007No ratings yet
- Menstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiDocument16 pagesMenstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiBini Don DanielNo ratings yet
- Induction of Labour Techniq SADocument18 pagesInduction of Labour Techniq SAPujanaWiaktaNo ratings yet
- Forcep DeliveryDocument11 pagesForcep DeliveryAyushi100% (1)
- Traumatic PPHDocument30 pagesTraumatic PPHRizwana BanuNo ratings yet
- Phase 3 All EMQs in 1 Part OneDocument60 pagesPhase 3 All EMQs in 1 Part Onesanjayb1008491No ratings yet
- Abortion KuliahDocument38 pagesAbortion KuliahElsa Hasibuan100% (1)
- Abnormal Labor and Dystocia: Dept. of Ob&Gyn, The First Affiliated Hospital He KeDocument63 pagesAbnormal Labor and Dystocia: Dept. of Ob&Gyn, The First Affiliated Hospital He KeJoan LuisNo ratings yet
- Cholestatic Disease in PregnancyDocument25 pagesCholestatic Disease in Pregnancyarifbotwin100% (1)
- Operative Vaginal Delivery PDFDocument56 pagesOperative Vaginal Delivery PDFFarehan Md Isa100% (1)
- Trial of LabourDocument2 pagesTrial of Labourgeorgeloto12No ratings yet
- Fetal MonitoringDocument6 pagesFetal MonitoringRraouzmaaliNo ratings yet
- Practice Essentials: DefinitionsDocument5 pagesPractice Essentials: DefinitionsNovita sariNo ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Scaohoid Fracture 4Document34 pagesScaohoid Fracture 4Noor Al Zahraa Ali100% (1)
- Intrapartum Fetal Monitoring Guideline - Physiological-CTG PDFDocument33 pagesIntrapartum Fetal Monitoring Guideline - Physiological-CTG PDFKovacs TiborNo ratings yet
- Ectopic PregnancyDocument39 pagesEctopic PregnancyFecky Fihayatul IchsanNo ratings yet
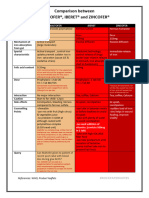
- Comparison Between Maltofer-Iberet-Zincofer TAMBAHANDocument4 pagesComparison Between Maltofer-Iberet-Zincofer TAMBAHANhomesweethomestaytciNo ratings yet
- Malformation of Female Reproductive SystemDocument170 pagesMalformation of Female Reproductive SystemKriti BanstolaNo ratings yet
- Abdominal HysterectomyDocument28 pagesAbdominal HysterectomyNatanael SusantoNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Anatomy of Female Genital TractDocument99 pagesAnatomy of Female Genital TractIuliana StefanucaNo ratings yet
- 19 - Trauma in PregancyDocument23 pages19 - Trauma in PregancyIman KadeNo ratings yet
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Document559 pagesObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113No ratings yet
- Dystocia 2010Document55 pagesDystocia 2010Meigy NitalessyNo ratings yet
- Normal Conduct of LaborDocument62 pagesNormal Conduct of LaborFaye Cabotaje LinganNo ratings yet
- Gynecological LaparosDocument32 pagesGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Evolving Concepts of The Vulnerable Atherosclerotic Plaque and TheDocument16 pagesEvolving Concepts of The Vulnerable Atherosclerotic Plaque and TheKhánh Nguyễn NgọcNo ratings yet
- Acetaminophen Increases Aldosterone Secretion While SuppressingDocument7 pagesAcetaminophen Increases Aldosterone Secretion While SuppressingKhánh Nguyễn NgọcNo ratings yet
- Extrarenal Effects of Aldosterone On Potassium HomeostasisDocument8 pagesExtrarenal Effects of Aldosterone On Potassium HomeostasisKhánh Nguyễn NgọcNo ratings yet
- Cir 0000000000001092Document19 pagesCir 0000000000001092Khánh Nguyễn NgọcNo ratings yet
- Maternal and Neonatal Immunization Field Guide: For Latin America and The CaribbeanDocument94 pagesMaternal and Neonatal Immunization Field Guide: For Latin America and The Caribbeanmrizky ihsanNo ratings yet
- Mefenamic Acid Drug Study FormDocument2 pagesMefenamic Acid Drug Study Form2C- VILLACARLOS, LEONA ROSE M.No ratings yet
- GE Elect 3 Module 13 14 MangiboaDocument8 pagesGE Elect 3 Module 13 14 MangiboaMary Loiesyl Camara Ubay-ubayNo ratings yet
- Nursing Seminar 1 SAS Session 14Document8 pagesNursing Seminar 1 SAS Session 14ZiaNo ratings yet
- Vesicovaginal Fistula in Uganda: Journal of Obstetrics and GynaecologyDocument7 pagesVesicovaginal Fistula in Uganda: Journal of Obstetrics and GynaecologyAli AlyousfeNo ratings yet
- Debating 101Document3 pagesDebating 101Azalia AretaNo ratings yet
- LPLT12405 : LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document2 pagesLPLT12405 : LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085TarunNo ratings yet
- Research Article: The Effects of Yoga Exercise On Pelvic Floor Rehabilitation of Postpartum WomenDocument16 pagesResearch Article: The Effects of Yoga Exercise On Pelvic Floor Rehabilitation of Postpartum WomenFoto AyuNo ratings yet
- Reference Brochure Thyroid 2011Document27 pagesReference Brochure Thyroid 2011ViktarNo ratings yet
- Literasi B. Inggris TO RG15Document6 pagesLiterasi B. Inggris TO RG15HelmyHaikalNo ratings yet
- General Biology 1: Disorders and Diseases: Cell Cycle Learning Activity 1: Mistakes in Cell DivisionDocument1 pageGeneral Biology 1: Disorders and Diseases: Cell Cycle Learning Activity 1: Mistakes in Cell DivisionArianne AtilasNo ratings yet
- Screenshot 2022-10-14 at 10.08.56 PMDocument38 pagesScreenshot 2022-10-14 at 10.08.56 PMParita ShahNo ratings yet
- SHM National Moot Court Competition 2022Document8 pagesSHM National Moot Court Competition 2022Ayushman DubeyNo ratings yet
- TimetableDocument13 pagesTimetableQonita Prasta AgustiaNo ratings yet
- Disease Condition:: Hyperemsis Gravidarum: DefinitionDocument4 pagesDisease Condition:: Hyperemsis Gravidarum: DefinitionPriyanka JohnNo ratings yet
- Muna Tahlak, MD, FACOG Latifa HospitalDocument44 pagesMuna Tahlak, MD, FACOG Latifa HospitalNur Rahmat Wibowo100% (1)
- Puberty in Girls: and What's HappeningDocument12 pagesPuberty in Girls: and What's HappeningCounseling BGANo ratings yet
- Lectures DGODocument10 pagesLectures DGOnumairaNo ratings yet
- Bergink, Veerle PDFDocument158 pagesBergink, Veerle PDFMonaIftikharNo ratings yet
- Reproductive Rights - A Comparative Study of Constitutional JurispDocument25 pagesReproductive Rights - A Comparative Study of Constitutional JurispBharat AntilNo ratings yet
- Cervical Cancer Causes, Risk Factors, and PreventionDocument15 pagesCervical Cancer Causes, Risk Factors, and PreventionSf AkhadiyatiNo ratings yet
- Vinod Soni v. Union of IndiaDocument5 pagesVinod Soni v. Union of IndiaSonia ShrinivasanNo ratings yet
- Effect of Phototherapy With Alumunium Foil Reflectors On Neonatal HyperbilirubinemiaDocument5 pagesEffect of Phototherapy With Alumunium Foil Reflectors On Neonatal HyperbilirubinemiaBunga Tri AmandaNo ratings yet
- Drug Study: Lorma Colleges Con Template Related Learning ExperienceDocument2 pagesDrug Study: Lorma Colleges Con Template Related Learning ExperienceJohn Angelo ValdezNo ratings yet
- Ijgo 13146Document7 pagesIjgo 13146evaNo ratings yet
- Article in Press: Caring For Women Through Early Pregnancy Loss: Exploring Nurses' Experiences of CareDocument7 pagesArticle in Press: Caring For Women Through Early Pregnancy Loss: Exploring Nurses' Experiences of Carekabo kaboNo ratings yet
- Herbs For Womb Health 2Document14 pagesHerbs For Womb Health 2Maggie WoodNo ratings yet