Download as pdf or txt
You might also like
- LABManualDocument3 pagesLABManualChriszaine PerezNo ratings yet
- Editorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystDocument4 pagesEditorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystLogical MonsterNo ratings yet
- Use of Locking-Loop Pigtail Nephrostomy Catheters in Dogs and Cats 20 Cases (2004 2009)Document10 pagesUse of Locking-Loop Pigtail Nephrostomy Catheters in Dogs and Cats 20 Cases (2004 2009)Bernardo BertoldiNo ratings yet
- Stenting in Pediatric TransplantationDocument27 pagesStenting in Pediatric TransplantationChris FrenchNo ratings yet
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Augmentation Bladder KomplikasiDocument9 pagesAugmentation Bladder KomplikasiOlivia BawaedaNo ratings yet
- Post-Cholecystectomy Acute Injury: What Can Go Wrong?Document7 pagesPost-Cholecystectomy Acute Injury: What Can Go Wrong?Ramyasree BadeNo ratings yet
- Trans-Fistulary Endoscopic Drainage For Post-Bariatric Abdominal Collections Communicating With The Upper Gastrointestinal TractDocument8 pagesTrans-Fistulary Endoscopic Drainage For Post-Bariatric Abdominal Collections Communicating With The Upper Gastrointestinal TractAlexandra JichituNo ratings yet
- Ureteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallDocument13 pagesUreteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallOoNo ratings yet
- Jurnal VaskularDocument6 pagesJurnal VaskulardrelvNo ratings yet
- Finally Ileal Ureter Corrected (1) (1) IbjuDocument11 pagesFinally Ileal Ureter Corrected (1) (1) IbjuSheshang KamathNo ratings yet
- 1 s2.0 S0022480423002895 MainDocument7 pages1 s2.0 S0022480423002895 Mainlucabarbato23No ratings yet
- Complications of Enterocystoplastycase SeriesDocument5 pagesComplications of Enterocystoplastycase SeriesIJAR JOURNALNo ratings yet
- Tube IleostomyDocument5 pagesTube IleostomyabhishekbmcNo ratings yet
- Plication of DJ Stents WceDocument1 pagePlication of DJ Stents Wcejinsi georgeNo ratings yet
- Hepaticojejunostomy vs. Hepaticoduodenostomy After Excision of Choledochal Cyst in Paediatric Population - A Retrospective StudyDocument3 pagesHepaticojejunostomy vs. Hepaticoduodenostomy After Excision of Choledochal Cyst in Paediatric Population - A Retrospective StudyGagan DeepNo ratings yet
- Dalton 2016Document4 pagesDalton 2016fjparadaNo ratings yet
- Complications of Biliary T-Tubes After Choledochotomy: Original ArticleDocument4 pagesComplications of Biliary T-Tubes After Choledochotomy: Original ArticleBikash SahNo ratings yet
- 9 Management of Common Bile-Duct Stones and Associated Gallbladder Stones: Surgical AspectsDocument14 pages9 Management of Common Bile-Duct Stones and Associated Gallbladder Stones: Surgical AspectsekoNo ratings yet
- Laparoscopic Repair of Vesicovaginal FistulaDocument4 pagesLaparoscopic Repair of Vesicovaginal FistulaGloria AteNo ratings yet
- Article 39794Document4 pagesArticle 39794d.amouzou1965No ratings yet
- Obstructive NephropathyDocument4 pagesObstructive NephropathyKevean Kimi LimNo ratings yet
- Intermittent Vs Indwelling CatheterizationDocument2 pagesIntermittent Vs Indwelling CatheterizationWildan DzakiyNo ratings yet
- Continuous Ambulatory Peritoneal Dialysis Catheter Placement Is Omentectomy Necessary 2016Document3 pagesContinuous Ambulatory Peritoneal Dialysis Catheter Placement Is Omentectomy Necessary 2016waldemar russellNo ratings yet
- Uro Catheter JournalDocument8 pagesUro Catheter JournalKokong Duda kereNo ratings yet
- Kurum Boor 2016Document4 pagesKurum Boor 2016Chema ToledoNo ratings yet
- A Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalDocument4 pagesA Study On Complications of Ventriculoperitoneal Shunt Surgery in Bir Hospital, Kathmandu, NepalHaziq AnuarNo ratings yet
- A Modified Supine Position Facilitates Bladder Function in Patient Undergoing Percutaneous Coronary InterventionDocument8 pagesA Modified Supine Position Facilitates Bladder Function in Patient Undergoing Percutaneous Coronary InterventionVelicia MargarethaNo ratings yet
- Is It Necessary To Ligate Distal Common Bile Duct Stumps After Excising Choledochal Cysts?Document4 pagesIs It Necessary To Ligate Distal Common Bile Duct Stumps After Excising Choledochal Cysts?Rajarshi KumarNo ratings yet
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpDocument9 pagesManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniNo ratings yet
- Congenital Hydronephrosis Disease or ConditionDocument8 pagesCongenital Hydronephrosis Disease or ConditionIrfan Syauqi AriantoNo ratings yet
- 1 s2.0 S2667008923000253 MainDocument4 pages1 s2.0 S2667008923000253 Mainal malikNo ratings yet
- Evidencia 1Document6 pagesEvidencia 1Ricardo Uzcategui ArreguiNo ratings yet
- Treatment of Obstructive Uropathy in One of Three Young Brothers Suffering From Gorlin-Cohen Syndrome: A Case ReportDocument4 pagesTreatment of Obstructive Uropathy in One of Three Young Brothers Suffering From Gorlin-Cohen Syndrome: A Case ReportMuhammad Kholid FirdausNo ratings yet
- 1 s2.0 S2214751921001584 MainDocument7 pages1 s2.0 S2214751921001584 MainfitriNo ratings yet
- PTBDDocument8 pagesPTBDDaniSantikaNo ratings yet
- Ureteric ComplicationsDocument7 pagesUreteric ComplicationstnsourceNo ratings yet
- Intermittent Catheterization and LoFricDocument32 pagesIntermittent Catheterization and LoFricmokilpoNo ratings yet
- PylonefritisDocument8 pagesPylonefritissintaNo ratings yet
- Pattern of Acute Intestinal Obstruction Is There A PDFDocument3 pagesPattern of Acute Intestinal Obstruction Is There A PDFMaría José Díaz RojasNo ratings yet
- JPM 14 00617Document9 pagesJPM 14 00617Taulant MukaNo ratings yet
- Role of Open Surgical Drainage or Aspiration in Management of Amoebic Liver AbscessDocument9 pagesRole of Open Surgical Drainage or Aspiration in Management of Amoebic Liver AbscessIJAR JOURNALNo ratings yet
- Reconstruction of Late-Onset Transplant Ureteral Stricture DiseaseDocument7 pagesReconstruction of Late-Onset Transplant Ureteral Stricture DiseasetnsourceNo ratings yet
- 1 s2.0 S1477513122005782 MainDocument8 pages1 s2.0 S1477513122005782 MainReza EffendiNo ratings yet
- Urinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesDocument10 pagesUrinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesRara Aulia IINo ratings yet
- Urologic Complications in Renal Transplants: Hannah R. Choate, Laura A. Mihalko, Bevan T. ChoateDocument7 pagesUrologic Complications in Renal Transplants: Hannah R. Choate, Laura A. Mihalko, Bevan T. ChoateNidhin MathewNo ratings yet
- Yan 2015Document4 pagesYan 2015ELIECERNo ratings yet
- 11228-Article Text-39349-1-10-20141009 PDFDocument5 pages11228-Article Text-39349-1-10-20141009 PDFsahandNo ratings yet
- Endourology and Stone Diseases: Original ArticlesDocument5 pagesEndourology and Stone Diseases: Original ArticlesTatik HandayaniNo ratings yet
- Vandenberg 2015Document8 pagesVandenberg 2015Zven BlackNo ratings yet
- Complete Penile DisassemblyDocument2 pagesComplete Penile DisassemblyGunduz AgaNo ratings yet
- Postoperative Fistula PancreaticDocument7 pagesPostoperative Fistula PancreaticstonmanNo ratings yet
- Early Complications Followoing Laparoscopic Cholecystectomy in Basrah General HospitalDocument15 pagesEarly Complications Followoing Laparoscopic Cholecystectomy in Basrah General HospitalBurhan SabirNo ratings yet
- Augmentation Cystoplasty in The Patient With Neurogenic BladderDocument12 pagesAugmentation Cystoplasty in The Patient With Neurogenic BladderReza EffendiNo ratings yet
- Reconstruction of Late-Onset Transplant Ureteral Stricture DiseaseDocument6 pagesReconstruction of Late-Onset Transplant Ureteral Stricture DiseaseAnanda KumarNo ratings yet
- s00535-015-1096-6Document15 pagess00535-015-1096-6Rogelio LlanesNo ratings yet
- 1 s2.0 S2772973723000188 MainDocument6 pages1 s2.0 S2772973723000188 MainMDrakeNo ratings yet
- International Journal of Nursing Studies: SciencedirectDocument4 pagesInternational Journal of Nursing Studies: Sciencedirectyoga madaniNo ratings yet
- Open Access Journal of Urology & Nephrology: Interventional Radiology Techniques in The Genitourinary TractDocument5 pagesOpen Access Journal of Urology & Nephrology: Interventional Radiology Techniques in The Genitourinary Tractalfredo elizondoNo ratings yet
- WarshawDocument11 pagesWarshawJuan RamirezNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Rhinitis Allergy and ElderlyDocument26 pagesRhinitis Allergy and ElderlyPutri Rizky AmaliaNo ratings yet
- Controversial TopicDocument11 pagesControversial TopicPutri Rizky AmaliaNo ratings yet
- Peterson 2012Document5 pagesPeterson 2012Putri Rizky AmaliaNo ratings yet
- Role of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayDocument6 pagesRole of Rhinitis in Laryngitis: Another Dimension of The Unified AirwayPutri Rizky AmaliaNo ratings yet
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- Literature Reading Short StatureDocument34 pagesLiterature Reading Short StaturePutri Rizky AmaliaNo ratings yet
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- Doctor Patient RelationshipDocument21 pagesDoctor Patient RelationshipPutri Rizky AmaliaNo ratings yet
- Epos Summary PDFDocument30 pagesEpos Summary PDFPutri Rizky AmaliaNo ratings yet
- The Half-Life of Infusion Fluids An Educational ReviewDocument8 pagesThe Half-Life of Infusion Fluids An Educational ReviewPutri Rizky AmaliaNo ratings yet
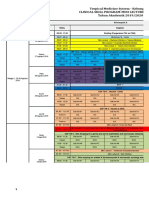
- Jadwal Perkulihanan THN 4 2019-2020 TM-FMDocument20 pagesJadwal Perkulihanan THN 4 2019-2020 TM-FMPutri Rizky AmaliaNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky Amalia100% (1)
- Kidney Anatomy and PhysiologyDocument5 pagesKidney Anatomy and PhysiologyDianne MacaraigNo ratings yet
- CHAPTER III UrolithiasisDocument10 pagesCHAPTER III Urolithiasisvictor zhefaNo ratings yet
- Republic of The Philippines Department of Education Region I Division of La Union San Juan District Second Quarter Name: - ScoreDocument3 pagesRepublic of The Philippines Department of Education Region I Division of La Union San Juan District Second Quarter Name: - ScoreMary Jane Acierto-cuello100% (3)
- Uts Las 7Document3 pagesUts Las 7Diane JavierNo ratings yet
- Renal Physiology: D. C. Mikulecky Faculty Mentoring Program Virginia Commonwealth UnivDocument35 pagesRenal Physiology: D. C. Mikulecky Faculty Mentoring Program Virginia Commonwealth UnivRiccardo Mason TroiaNo ratings yet
- Clitoral ErectionDocument4 pagesClitoral ErectionnathanNo ratings yet
- Anatomy of The Prostate GlandDocument18 pagesAnatomy of The Prostate GlandRao Ghayoor DxNo ratings yet
- CATHETERIZATIONDocument3 pagesCATHETERIZATIONanimesh pandaNo ratings yet
- Uti PBL 2Document1 pageUti PBL 2Aliah ZuhairahNo ratings yet
- Applied Animal ReproductionDocument91 pagesApplied Animal ReproductionArslan Aziz100% (1)
- Acute Kidney Injury in Children: Being AWAREDocument4 pagesAcute Kidney Injury in Children: Being AWAREIrkania PasangkaNo ratings yet
- Science and Health 5Document15 pagesScience and Health 5Ryrl ShinNo ratings yet
- UTI Disorder PDFDocument23 pagesUTI Disorder PDFMonarahayuNo ratings yet
- Strategic Intervention Materials PresentationDocument55 pagesStrategic Intervention Materials PresentationMary Athena Ibardaloza Adesna100% (15)
- Cranberry LaunchDocument11 pagesCranberry LaunchShouvik Das100% (1)
- Vesicoureteral Reflux 508Document8 pagesVesicoureteral Reflux 508Ikhdin SaadhiNo ratings yet
- Continuing Education Activity: HypospadiasDocument6 pagesContinuing Education Activity: HypospadiasMaulani Nurlatifah100% (1)
- Anatomy and Physiology of The Male and Female Reproductive System Female Reproductive Anatomy and PhysiologyDocument6 pagesAnatomy and Physiology of The Male and Female Reproductive System Female Reproductive Anatomy and PhysiologyJustJ ThingsNo ratings yet
- Male GenitaliaDocument3 pagesMale GenitaliaNathaniel PulidoNo ratings yet
- Anatomy and Physiology - EctopicDocument4 pagesAnatomy and Physiology - EctopicReyzelinNo ratings yet
- Semen Analysis - Aubf (BSMLS Olfu)Document8 pagesSemen Analysis - Aubf (BSMLS Olfu)Mitch IbayNo ratings yet
- Lec 18Document4 pagesLec 18Lyanna Louise SantosNo ratings yet
- The Reproductive System: Alyssa Ashley R. DiegoDocument46 pagesThe Reproductive System: Alyssa Ashley R. DiegoteacherashleyNo ratings yet
- Histology Male ReproductiveDocument31 pagesHistology Male Reproductivekhiks34No ratings yet
- Anatomy and PhysiologyDocument3 pagesAnatomy and PhysiologyChristopher bruncanoNo ratings yet
- Urinary System NotesDocument9 pagesUrinary System NotesBijay Kumar MahatoNo ratings yet
- Kulpak UPN - AnatomiDocument21 pagesKulpak UPN - AnatomigresiasallyNo ratings yet
- Physiology OF Renal SYSTEMDocument24 pagesPhysiology OF Renal SYSTEMsam bossaNo ratings yet
- Iraqi BOARDDocument14 pagesIraqi BOARDNasser AlbaddaiNo ratings yet