
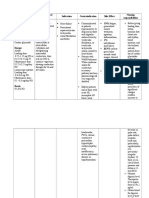
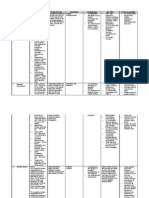
Drug Study (Amiodarone)
Drug Study (Amiodarone)
You might also like
- The Infamous Loserlimab RTF LetterDocument21 pagesThe Infamous Loserlimab RTF Letterbuyersstrikewp100% (3)
- Lesson Plan - A Caffeine Fueled WorldDocument5 pagesLesson Plan - A Caffeine Fueled WorldYaraCarobrez100% (1)
- Dobutamine Drug StudyDocument1 pageDobutamine Drug Studyjoella100% (1)
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Dobutamine Drug StudyDocument1 pageDobutamine Drug Studyzyr2189100% (2)
- EpinephrineDocument1 pageEpinephrineiamELHIZA67% (3)
- Nitroglycerin Drug StudyDocument2 pagesNitroglycerin Drug StudyNasrah N. Musa100% (6)
- Drug Study - NitroglycerinDocument2 pagesDrug Study - NitroglycerinKian Herrera100% (1)
- Calcium Gluconate Drug StudyDocument1 pageCalcium Gluconate Drug StudyChaepmunk Cy75% (4)
- VerapamilDocument1 pageVerapamilStephanie PeNo ratings yet
- Therapeutics HandbookDocument49 pagesTherapeutics Handbookaasdf100% (1)
- Amiodarone Drug StudyDocument3 pagesAmiodarone Drug StudyDexter Niel Ortilano CPAC-SNNo ratings yet
- DigoxinDocument4 pagesDigoxinJaessa FelicianoNo ratings yet
- DRUG STUDY - FurosemideDocument2 pagesDRUG STUDY - FurosemideKian HerreraNo ratings yet
- Dopamine HydrochlorideDocument2 pagesDopamine HydrochlorideNasrah N. MusaNo ratings yet
- Pharmacologic: Cardiovascular: FlushingDocument2 pagesPharmacologic: Cardiovascular: Flushingitsmeaya100% (5)
- EsmololDocument2 pagesEsmololtherock316_995149No ratings yet
- Atropine Sulfate Drug StudyDocument2 pagesAtropine Sulfate Drug StudyNasrah N. Musa67% (6)
- Midazolam Drug Study SaclotDocument1 pageMidazolam Drug Study SaclotMaybelle Cababat Saclot100% (1)
- AmiodaroneDocument2 pagesAmiodaronePauling Frez100% (5)
- Amiodarone (Cordarone)Document1 pageAmiodarone (Cordarone)jaybamanNo ratings yet
- Drug Study Calcium GluconateDocument1 pageDrug Study Calcium GluconateLarah Mae AndogNo ratings yet
- Sodium Bicarbonate Drug StudyDocument2 pagesSodium Bicarbonate Drug StudyMelinda Cariño BallonNo ratings yet
- Calcium GluconateDocument2 pagesCalcium GluconateMae Ann Bueno Castillon100% (1)
- Calcium Gluconate Drug StudyDocument1 pageCalcium Gluconate Drug StudyMichael Baylon DueñasNo ratings yet
- Drug Study (Aspirin, in Enalapril Maleate, Tramadol, AmlodipineDocument10 pagesDrug Study (Aspirin, in Enalapril Maleate, Tramadol, AmlodipineFlauros Ryu Jabien100% (1)
- Amiodarone (PACERONE)Document1 pageAmiodarone (PACERONE)Amanda CoadNo ratings yet
- Generic Name: Brand Name:: ClassificationsDocument2 pagesGeneric Name: Brand Name:: ClassificationsbillyktoubattsNo ratings yet
- Drug StudyDocument1 pageDrug Studyzjoshuac100% (1)
- Drug StudyDocument6 pagesDrug StudyGeraldine Gallaron - CasipongNo ratings yet
- Heparin InjectionDocument2 pagesHeparin InjectiongagandipkSNo ratings yet
- EnalaprilDocument4 pagesEnalaprilGwyn RosalesNo ratings yet
- DRUG STUDY SpironolactoneDocument4 pagesDRUG STUDY SpironolactoneJerremy LuqueNo ratings yet
- DobutamineDocument2 pagesDobutamineJaessa FelicianoNo ratings yet
- Drug StudyDocument3 pagesDrug Studyunkown userNo ratings yet
- EsmololDocument3 pagesEsmololTri Purma SariNo ratings yet
- Drug Study - Calcium GluconateDocument1 pageDrug Study - Calcium GluconatemikErlhNo ratings yet
- Drugstudy PotassiumchlorideDocument3 pagesDrugstudy Potassiumchloridetrina412No ratings yet
- Atenolol Drug StudyDocument2 pagesAtenolol Drug StudyFranz.thenurse6888100% (2)
- Drug Study - DigoxinDocument2 pagesDrug Study - DigoxinKian Herrera50% (2)
- Calcium Gluconate Drug SummDocument1 pageCalcium Gluconate Drug SummWarren100% (2)
- Drug StudyDocument6 pagesDrug StudyBrix John PortellanoNo ratings yet
- Acyclovir Drug Study WWW RNpedia ComDocument3 pagesAcyclovir Drug Study WWW RNpedia ComJanaica JuanNo ratings yet
- Drug Study D5W2Document3 pagesDrug Study D5W2Girlie Jane Sevillano RN100% (2)
- Drug Study DexamethasoneDocument4 pagesDrug Study Dexamethasoneamal abdulrahmanNo ratings yet
- Drug Study - MidazolamDocument8 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- Sevelamer - Drug StudyDocument1 pageSevelamer - Drug StudyAcads use100% (2)
- Case Presentation Station 3B Drug Study Sodium BicarbonateDocument5 pagesCase Presentation Station 3B Drug Study Sodium BicarbonatehahahahaaaaaaaNo ratings yet
- Dopamine HCLDocument1 pageDopamine HCLIvanne Hisoler100% (3)
- Drug Study - MidazolamDocument2 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- SHEENA Clomid Drug StudyDocument3 pagesSHEENA Clomid Drug StudyNur SetsuNo ratings yet
- HydrochlorothiazideDocument2 pagesHydrochlorothiazidekuro hanabusa100% (1)
- Drug StudyDocument3 pagesDrug StudyROCHELLE DALIWAN100% (1)
- Drug Study - AlfuzosinDocument1 pageDrug Study - AlfuzosinKian HerreraNo ratings yet
- DRUG STUDY - Calcium GluconateDocument2 pagesDRUG STUDY - Calcium GluconateSiergs Smith Gervacio100% (2)
- ACETAZOLAMIDEDocument2 pagesACETAZOLAMIDEjhitch1683% (6)
- Drug StudyDocument5 pagesDrug StudyLizeth Querubin92% (25)
- Dopamine Drug StudyDocument6 pagesDopamine Drug StudyGeorge RussellNo ratings yet
- Drug Study ClonidineDocument2 pagesDrug Study ClonidineCezanne CruzNo ratings yet
- P.W Drug Cards Week 10.... REDOOODocument19 pagesP.W Drug Cards Week 10.... REDOOOPRECIOUS wardNo ratings yet
- Class III AntiarrhythmicsDocument5 pagesClass III AntiarrhythmicsShereen Alobinay100% (1)
- Sotalol HydrochlorideDocument2 pagesSotalol HydrochlorideLIEZEL GRACE VELAYONo ratings yet
- Drug StudDocument31 pagesDrug StudTwisted FlameNo ratings yet
- Cephalocaudal AssessmentDocument9 pagesCephalocaudal AssessmentJustine ConuiNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Cues: Short Term: Independent: Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Cues: Short Term: Independent: Short TermJustine ConuiNo ratings yet
- Acute Lymphocytic LeukemiaDocument2 pagesAcute Lymphocytic LeukemiaJustine ConuiNo ratings yet
- Toddler NCPDocument2 pagesToddler NCPJustine Conui100% (1)
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Bryophyllum Pinnatum: (Katakataka)Document7 pagesBryophyllum Pinnatum: (Katakataka)JeemCarloFagelaPulaNo ratings yet
- Blood BankDocument10 pagesBlood BankMarie LlanesNo ratings yet
- Day 1 General Objective:: CognitiveDocument2 pagesDay 1 General Objective:: CognitiveReihann N. EdresNo ratings yet
- Chapter 36 Death Study GuideDocument25 pagesChapter 36 Death Study GuideDaniel McVayNo ratings yet
- Nashta: Gaurav Bapat Jagadis Purohit Ramyogananth Shambu Nandanan Surbhi Malhotra Swati Sahu Vikalp KataraDocument41 pagesNashta: Gaurav Bapat Jagadis Purohit Ramyogananth Shambu Nandanan Surbhi Malhotra Swati Sahu Vikalp KataraNaman ChaudharyNo ratings yet
- NewEarth - University COVID-19 Intelligence BriefDocument47 pagesNewEarth - University COVID-19 Intelligence BriefTony Lambert100% (1)
- "Pharmaceutical Care": (Asuhan Kefarmasian)Document37 pages"Pharmaceutical Care": (Asuhan Kefarmasian)Ririn sefrianiNo ratings yet
- Cognitive Impairment Evaluation and ManagementDocument19 pagesCognitive Impairment Evaluation and ManagementSAMUEL MARIN FUQUENENo ratings yet
- Altered Renal Perfusion CRFDocument5 pagesAltered Renal Perfusion CRFGen Ramos- SolisNo ratings yet
- ENG Paper 2 TrialDocument17 pagesENG Paper 2 TrialstudentmbsNo ratings yet
- Isolation GuidelinesDocument203 pagesIsolation GuidelinesAlifia TrisnaningrumNo ratings yet
- Dialog AssignmentDocument4 pagesDialog AssignmentKitket Photografi & Cinematografi100% (1)
- History of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedDocument3 pagesHistory of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedVicente BaltazarNo ratings yet
- Best Practice Workbook - Bipolar Disorder-Yong Xiang YiDocument45 pagesBest Practice Workbook - Bipolar Disorder-Yong Xiang YiJuraidahMohdNooh100% (1)
- CHM Case Study ChymotrypsinDocument8 pagesCHM Case Study Chymotrypsinfanney- chanNo ratings yet
- Hormone Replacement Therapy The Right Choice For Your PatientDocument9 pagesHormone Replacement Therapy The Right Choice For Your Patientdanny17phNo ratings yet
- Term Paper On Air PollutionDocument5 pagesTerm Paper On Air PollutionaixgaoqifNo ratings yet
- Solid Dosage Forms in Unani System of Medicine AnDocument7 pagesSolid Dosage Forms in Unani System of Medicine AnSiddharth JainNo ratings yet
- Men's Treatment GriffinDocument68 pagesMen's Treatment GriffintadcpNo ratings yet
- Kyle Liddle - Argumentative EssayDocument7 pagesKyle Liddle - Argumentative Essayapi-530385868No ratings yet
- Nursing History FormatDocument5 pagesNursing History FormatMira AurumtinNo ratings yet
- Biology Model Exam 2016Document18 pagesBiology Model Exam 2016samuelfiqiree345No ratings yet
- 41 & 42 - Nucleic Acid MetabolismDocument56 pages41 & 42 - Nucleic Acid MetabolismMădă Claws100% (1)
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- Charles Mann ProbableDocument2 pagesCharles Mann ProbableKIRO 7 Eyewitness NewsNo ratings yet
- Valproic Acid Drug Study PDFDocument4 pagesValproic Acid Drug Study PDFLiza Marie IgnacioNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- The Infamous Loserlimab RTF LetterDocument21 pagesThe Infamous Loserlimab RTF Letterbuyersstrikewp100% (3)
- Lesson Plan - A Caffeine Fueled WorldDocument5 pagesLesson Plan - A Caffeine Fueled WorldYaraCarobrez100% (1)
- Dobutamine Drug StudyDocument1 pageDobutamine Drug Studyjoella100% (1)
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Dobutamine Drug StudyDocument1 pageDobutamine Drug Studyzyr2189100% (2)
- EpinephrineDocument1 pageEpinephrineiamELHIZA67% (3)
- Nitroglycerin Drug StudyDocument2 pagesNitroglycerin Drug StudyNasrah N. Musa100% (6)
- Drug Study - NitroglycerinDocument2 pagesDrug Study - NitroglycerinKian Herrera100% (1)
- Calcium Gluconate Drug StudyDocument1 pageCalcium Gluconate Drug StudyChaepmunk Cy75% (4)
- VerapamilDocument1 pageVerapamilStephanie PeNo ratings yet
- Therapeutics HandbookDocument49 pagesTherapeutics Handbookaasdf100% (1)
- Amiodarone Drug StudyDocument3 pagesAmiodarone Drug StudyDexter Niel Ortilano CPAC-SNNo ratings yet
- DigoxinDocument4 pagesDigoxinJaessa FelicianoNo ratings yet
- DRUG STUDY - FurosemideDocument2 pagesDRUG STUDY - FurosemideKian HerreraNo ratings yet
- Dopamine HydrochlorideDocument2 pagesDopamine HydrochlorideNasrah N. MusaNo ratings yet
- Pharmacologic: Cardiovascular: FlushingDocument2 pagesPharmacologic: Cardiovascular: Flushingitsmeaya100% (5)
- EsmololDocument2 pagesEsmololtherock316_995149No ratings yet
- Atropine Sulfate Drug StudyDocument2 pagesAtropine Sulfate Drug StudyNasrah N. Musa67% (6)
- Midazolam Drug Study SaclotDocument1 pageMidazolam Drug Study SaclotMaybelle Cababat Saclot100% (1)
- AmiodaroneDocument2 pagesAmiodaronePauling Frez100% (5)
- Amiodarone (Cordarone)Document1 pageAmiodarone (Cordarone)jaybamanNo ratings yet
- Drug Study Calcium GluconateDocument1 pageDrug Study Calcium GluconateLarah Mae AndogNo ratings yet
- Sodium Bicarbonate Drug StudyDocument2 pagesSodium Bicarbonate Drug StudyMelinda Cariño BallonNo ratings yet
- Calcium GluconateDocument2 pagesCalcium GluconateMae Ann Bueno Castillon100% (1)
- Calcium Gluconate Drug StudyDocument1 pageCalcium Gluconate Drug StudyMichael Baylon DueñasNo ratings yet
- Drug Study (Aspirin, in Enalapril Maleate, Tramadol, AmlodipineDocument10 pagesDrug Study (Aspirin, in Enalapril Maleate, Tramadol, AmlodipineFlauros Ryu Jabien100% (1)
- Amiodarone (PACERONE)Document1 pageAmiodarone (PACERONE)Amanda CoadNo ratings yet
- Generic Name: Brand Name:: ClassificationsDocument2 pagesGeneric Name: Brand Name:: ClassificationsbillyktoubattsNo ratings yet
- Drug StudyDocument1 pageDrug Studyzjoshuac100% (1)
- Drug StudyDocument6 pagesDrug StudyGeraldine Gallaron - CasipongNo ratings yet
- Heparin InjectionDocument2 pagesHeparin InjectiongagandipkSNo ratings yet
- EnalaprilDocument4 pagesEnalaprilGwyn RosalesNo ratings yet
- DRUG STUDY SpironolactoneDocument4 pagesDRUG STUDY SpironolactoneJerremy LuqueNo ratings yet
- DobutamineDocument2 pagesDobutamineJaessa FelicianoNo ratings yet
- Drug StudyDocument3 pagesDrug Studyunkown userNo ratings yet
- EsmololDocument3 pagesEsmololTri Purma SariNo ratings yet
- Drug Study - Calcium GluconateDocument1 pageDrug Study - Calcium GluconatemikErlhNo ratings yet
- Drugstudy PotassiumchlorideDocument3 pagesDrugstudy Potassiumchloridetrina412No ratings yet
- Atenolol Drug StudyDocument2 pagesAtenolol Drug StudyFranz.thenurse6888100% (2)
- Drug Study - DigoxinDocument2 pagesDrug Study - DigoxinKian Herrera50% (2)
- Calcium Gluconate Drug SummDocument1 pageCalcium Gluconate Drug SummWarren100% (2)
- Drug StudyDocument6 pagesDrug StudyBrix John PortellanoNo ratings yet
- Acyclovir Drug Study WWW RNpedia ComDocument3 pagesAcyclovir Drug Study WWW RNpedia ComJanaica JuanNo ratings yet
- Drug Study D5W2Document3 pagesDrug Study D5W2Girlie Jane Sevillano RN100% (2)
- Drug Study DexamethasoneDocument4 pagesDrug Study Dexamethasoneamal abdulrahmanNo ratings yet
- Drug Study - MidazolamDocument8 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- Sevelamer - Drug StudyDocument1 pageSevelamer - Drug StudyAcads use100% (2)
- Case Presentation Station 3B Drug Study Sodium BicarbonateDocument5 pagesCase Presentation Station 3B Drug Study Sodium BicarbonatehahahahaaaaaaaNo ratings yet
- Dopamine HCLDocument1 pageDopamine HCLIvanne Hisoler100% (3)
- Drug Study - MidazolamDocument2 pagesDrug Study - MidazolamKian HerreraNo ratings yet
- SHEENA Clomid Drug StudyDocument3 pagesSHEENA Clomid Drug StudyNur SetsuNo ratings yet
- HydrochlorothiazideDocument2 pagesHydrochlorothiazidekuro hanabusa100% (1)
- Drug StudyDocument3 pagesDrug StudyROCHELLE DALIWAN100% (1)
- Drug Study - AlfuzosinDocument1 pageDrug Study - AlfuzosinKian HerreraNo ratings yet
- DRUG STUDY - Calcium GluconateDocument2 pagesDRUG STUDY - Calcium GluconateSiergs Smith Gervacio100% (2)
- ACETAZOLAMIDEDocument2 pagesACETAZOLAMIDEjhitch1683% (6)
- Drug StudyDocument5 pagesDrug StudyLizeth Querubin92% (25)
- Dopamine Drug StudyDocument6 pagesDopamine Drug StudyGeorge RussellNo ratings yet
- Drug Study ClonidineDocument2 pagesDrug Study ClonidineCezanne CruzNo ratings yet
- P.W Drug Cards Week 10.... REDOOODocument19 pagesP.W Drug Cards Week 10.... REDOOOPRECIOUS wardNo ratings yet
- Class III AntiarrhythmicsDocument5 pagesClass III AntiarrhythmicsShereen Alobinay100% (1)
- Sotalol HydrochlorideDocument2 pagesSotalol HydrochlorideLIEZEL GRACE VELAYONo ratings yet
- Drug StudDocument31 pagesDrug StudTwisted FlameNo ratings yet
- Cephalocaudal AssessmentDocument9 pagesCephalocaudal AssessmentJustine ConuiNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Cues: Short Term: Independent: Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Cues: Short Term: Independent: Short TermJustine ConuiNo ratings yet
- Acute Lymphocytic LeukemiaDocument2 pagesAcute Lymphocytic LeukemiaJustine ConuiNo ratings yet
- Toddler NCPDocument2 pagesToddler NCPJustine Conui100% (1)
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Bryophyllum Pinnatum: (Katakataka)Document7 pagesBryophyllum Pinnatum: (Katakataka)JeemCarloFagelaPulaNo ratings yet
- Blood BankDocument10 pagesBlood BankMarie LlanesNo ratings yet
- Day 1 General Objective:: CognitiveDocument2 pagesDay 1 General Objective:: CognitiveReihann N. EdresNo ratings yet
- Chapter 36 Death Study GuideDocument25 pagesChapter 36 Death Study GuideDaniel McVayNo ratings yet
- Nashta: Gaurav Bapat Jagadis Purohit Ramyogananth Shambu Nandanan Surbhi Malhotra Swati Sahu Vikalp KataraDocument41 pagesNashta: Gaurav Bapat Jagadis Purohit Ramyogananth Shambu Nandanan Surbhi Malhotra Swati Sahu Vikalp KataraNaman ChaudharyNo ratings yet
- NewEarth - University COVID-19 Intelligence BriefDocument47 pagesNewEarth - University COVID-19 Intelligence BriefTony Lambert100% (1)
- "Pharmaceutical Care": (Asuhan Kefarmasian)Document37 pages"Pharmaceutical Care": (Asuhan Kefarmasian)Ririn sefrianiNo ratings yet
- Cognitive Impairment Evaluation and ManagementDocument19 pagesCognitive Impairment Evaluation and ManagementSAMUEL MARIN FUQUENENo ratings yet
- Altered Renal Perfusion CRFDocument5 pagesAltered Renal Perfusion CRFGen Ramos- SolisNo ratings yet
- ENG Paper 2 TrialDocument17 pagesENG Paper 2 TrialstudentmbsNo ratings yet
- Isolation GuidelinesDocument203 pagesIsolation GuidelinesAlifia TrisnaningrumNo ratings yet
- Dialog AssignmentDocument4 pagesDialog AssignmentKitket Photografi & Cinematografi100% (1)
- History of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedDocument3 pagesHistory of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedVicente BaltazarNo ratings yet
- Best Practice Workbook - Bipolar Disorder-Yong Xiang YiDocument45 pagesBest Practice Workbook - Bipolar Disorder-Yong Xiang YiJuraidahMohdNooh100% (1)
- CHM Case Study ChymotrypsinDocument8 pagesCHM Case Study Chymotrypsinfanney- chanNo ratings yet
- Hormone Replacement Therapy The Right Choice For Your PatientDocument9 pagesHormone Replacement Therapy The Right Choice For Your Patientdanny17phNo ratings yet
- Term Paper On Air PollutionDocument5 pagesTerm Paper On Air PollutionaixgaoqifNo ratings yet
- Solid Dosage Forms in Unani System of Medicine AnDocument7 pagesSolid Dosage Forms in Unani System of Medicine AnSiddharth JainNo ratings yet
- Men's Treatment GriffinDocument68 pagesMen's Treatment GriffintadcpNo ratings yet
- Kyle Liddle - Argumentative EssayDocument7 pagesKyle Liddle - Argumentative Essayapi-530385868No ratings yet
- Nursing History FormatDocument5 pagesNursing History FormatMira AurumtinNo ratings yet
- Biology Model Exam 2016Document18 pagesBiology Model Exam 2016samuelfiqiree345No ratings yet
- 41 & 42 - Nucleic Acid MetabolismDocument56 pages41 & 42 - Nucleic Acid MetabolismMădă Claws100% (1)
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- Charles Mann ProbableDocument2 pagesCharles Mann ProbableKIRO 7 Eyewitness NewsNo ratings yet
- Valproic Acid Drug Study PDFDocument4 pagesValproic Acid Drug Study PDFLiza Marie IgnacioNo ratings yet