Download as pdf or txt
You might also like
- Ongoing Debate in Orbital FracturesDocument11 pagesOngoing Debate in Orbital Fractureslaljadeff12100% (1)
- Reconstruction TechniquesDocument5 pagesReconstruction TechniquesGokul GopiNo ratings yet
- The Nasolabial Flap: The Most Versatile Method in Facial ReconstructionDocument7 pagesThe Nasolabial Flap: The Most Versatile Method in Facial Reconstructionshreya dasNo ratings yet
- The Spreader Flap in Primary Rhinoplasty: BackgroundDocument8 pagesThe Spreader Flap in Primary Rhinoplasty: BackgroundAlex Rolando SuntaxiNo ratings yet
- Component Dorsal Hump Reducton PMID 15457053Document11 pagesComponent Dorsal Hump Reducton PMID 15457053julio torresNo ratings yet
- Baur2014 2Document7 pagesBaur2014 2mona khosraviNo ratings yet
- Nasal Base ReductionDocument6 pagesNasal Base Reductiondiego suescunNo ratings yet
- Regional Flaps Head and NeckDocument6 pagesRegional Flaps Head and NeckJim HopkinsNo ratings yet
- Nasal Base SurgeryDocument8 pagesNasal Base SurgeryLaureano FilhoNo ratings yet
- Bardach 1995Document4 pagesBardach 1995ABKarthikeyanNo ratings yet
- Total Soft Palate Reconstruction Using The Palatal Island and Lateral Pharyngeal WallDocument5 pagesTotal Soft Palate Reconstruction Using The Palatal Island and Lateral Pharyngeal WallDr Saikat SahaNo ratings yet
- Reverse Sural Artery Pedicle Flap.20Document2 pagesReverse Sural Artery Pedicle Flap.20Sisay GirmaNo ratings yet
- Submental Island FlapDocument20 pagesSubmental Island FlapdrshariquennazirNo ratings yet
- Sps 20079Document10 pagesSps 20079Zouzou YuNo ratings yet
- Fanous 2008Document36 pagesFanous 2008Mohammed ijasNo ratings yet
- Archivo 15 Marzo 2019Document15 pagesArchivo 15 Marzo 2019Enrique LinaresNo ratings yet
- Nasal Dorsal AugmentationDocument9 pagesNasal Dorsal AugmentationAnonymous O9x3NDNo ratings yet
- Glabellar Flaps For Reconstruction of Skin DefectsDocument6 pagesGlabellar Flaps For Reconstruction of Skin Defectslaljadeff12No ratings yet
- Sabapathy 2014Document15 pagesSabapathy 2014Trina ViskhawatNo ratings yet
- The Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsDocument8 pagesThe Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsSebastianNo ratings yet
- Soft Palat ReconstructionDocument5 pagesSoft Palat Reconstructionprogramari maxiloNo ratings yet
- Nasal SeptumDocument20 pagesNasal SeptumAlejandra Oliveros VargasNo ratings yet
- Alar Base Reduction and Alar-Columellar RelationshipDocument9 pagesAlar Base Reduction and Alar-Columellar RelationshipFabian Camelo OtorrinoNo ratings yet
- Caudal Septal Extension GraftDocument12 pagesCaudal Septal Extension Graftstéphan AlessandroNo ratings yet
- Bilobed Flaps: Cong Vo, DDS, MD, William Walsh Thomas, MD, Hans C. Brockhoff II, DDS, MD, Daniel Petrisor, DMD, MDDocument4 pagesBilobed Flaps: Cong Vo, DDS, MD, William Walsh Thomas, MD, Hans C. Brockhoff II, DDS, MD, Daniel Petrisor, DMD, MDlaljadeff12No ratings yet
- Sphenopalatine Artery Ligation, Technical NoteDocument3 pagesSphenopalatine Artery Ligation, Technical Notenatalia.gallinoNo ratings yet
- A Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryDocument9 pagesA Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryJWPlasticsurgeryNo ratings yet
- Michael Friedman, MD, Vytenis Grybauskas, MD, David Chang, MDDocument4 pagesMichael Friedman, MD, Vytenis Grybauskas, MD, David Chang, MDConstantin StanNo ratings yet
- Alar Spanning Suture - PerkinsDocument4 pagesAlar Spanning Suture - PerkinsBiraimaNo ratings yet
- P ('t':'3', 'I':'669533173') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document3 pagesP ('t':'3', 'I':'669533173') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)miadexxNo ratings yet
- Modified FAMMDocument4 pagesModified FAMMSilverline TeamNo ratings yet
- Spreader Flap Con GibaDocument7 pagesSpreader Flap Con GibaH Mauricio Zuñiga ZamoraNo ratings yet
- 2.rhinoplasty in The African American PatientDocument10 pages2.rhinoplasty in The African American PatientFabian Camelo OtorrinoNo ratings yet
- Current Approaches To Septal Saddle Nose Reconstruction Using AutograftsDocument7 pagesCurrent Approaches To Septal Saddle Nose Reconstruction Using AutograftsRosaMinnitiNo ratings yet
- Ferraz 2021Document8 pagesFerraz 2021wijana410No ratings yet
- Cirugía Orejas Prominente - Mustardé 1967Document5 pagesCirugía Orejas Prominente - Mustardé 196722omar22No ratings yet
- The Plastysma Myocutaneous F Lap: Dale A. Baur, DDS, MDDocument6 pagesThe Plastysma Myocutaneous F Lap: Dale A. Baur, DDS, MDlaljadeff12No ratings yet
- Total Laryngectomy: Technique: Harvey M. Tucker, MDDocument3 pagesTotal Laryngectomy: Technique: Harvey M. Tucker, MDKumaran Bagavathi RagavanNo ratings yet
- 40 Complex Facial Reconstruction Aldona Jedrysiak, M.DDocument6 pages40 Complex Facial Reconstruction Aldona Jedrysiak, M.DAndini RomzaNo ratings yet
- The Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North AmerDocument9 pagesThe Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North Amerlaljadeff12No ratings yet
- Jurnal Alar FlareDocument10 pagesJurnal Alar FlareMayaSuyataNo ratings yet
- Nasal Surgery For Sleep-Disordered BreathingDocument6 pagesNasal Surgery For Sleep-Disordered Breathinglaljadeff12No ratings yet
- Dhir 2016Document12 pagesDhir 2016Pasquale ProvaNo ratings yet
- The Cervicofacial Flap in Facial - 2003 - Oral and Maxillofacial Surgery ClinicDocument7 pagesThe Cervicofacial Flap in Facial - 2003 - Oral and Maxillofacial Surgery Cliniclaljadeff12No ratings yet
- Nasal Reconstruction 1Document11 pagesNasal Reconstruction 1geoffrowley3No ratings yet
- Ettinger 1980Document4 pagesEttinger 1980Krupali JainNo ratings yet
- Bilateral Advancement FlapDocument11 pagesBilateral Advancement FlapjeciscasNo ratings yet
- Closed RhinoplastyDocument10 pagesClosed RhinoplastyVivie SantidamrongkulNo ratings yet
- Kawase Artikel Contemp Neurosurg Maart 2008 E.J. DelwelDocument6 pagesKawase Artikel Contemp Neurosurg Maart 2008 E.J. DelwelMariagilNo ratings yet
- Kyestone Flaps PDFDocument9 pagesKyestone Flaps PDFDra. Bianca Ariza MoralesNo ratings yet
- PIIS1043181018300332Document4 pagesPIIS1043181018300332Ottofianus Alvedo Hewick KalangiNo ratings yet
- Mon 1.1 FowlerDocument4 pagesMon 1.1 FowlerMohannad WylieNo ratings yet
- All Approaches Midface TraumaDocument92 pagesAll Approaches Midface TraumaYogendra RawatNo ratings yet
- Versatility of The Coronal Approach in Maxillofacial Surgery PDFDocument6 pagesVersatility of The Coronal Approach in Maxillofacial Surgery PDFdrgurpal74No ratings yet
- Mclaurin 2020Document9 pagesMclaurin 2020magus davilaNo ratings yet
- Treatment NASALDocument7 pagesTreatment NASALRezaNo ratings yet
- Kridel 2018Document3 pagesKridel 2018nunisulastri1998No ratings yet
- Archfaci 5 2 197Document5 pagesArchfaci 5 2 197Mugdha FrancisNo ratings yet
- Pec MajorDocument6 pagesPec MajorUsama SaeedNo ratings yet
- Free FlapDocument19 pagesFree FlaperinastevianaNo ratings yet
- Treacher Collins Syndrome Comprehensi - 2004 - Oral and Maxillofacial Surgery CDocument21 pagesTreacher Collins Syndrome Comprehensi - 2004 - Oral and Maxillofacial Surgery Claljadeff12No ratings yet
- UntitledDocument221 pagesUntitledlaljadeff12No ratings yet
- Anesthesia ProtocolsDocument15 pagesAnesthesia Protocolslaljadeff12No ratings yet
- Oral and Maxillofacial Injuries Experienced - 2005 - Oral and Maxillofacial SurDocument9 pagesOral and Maxillofacial Injuries Experienced - 2005 - Oral and Maxillofacial Surlaljadeff12100% (1)
- Entropion: InstrumentsDocument158 pagesEntropion: Instrumentslaljadeff12No ratings yet
- Peripheral Odontogenic Tumors: Alice E. Curran, DMD, MSDocument10 pagesPeripheral Odontogenic Tumors: Alice E. Curran, DMD, MSlaljadeff12No ratings yet
- Odontogenic Malignancies: Lee J. Slater, DDS, MSDocument16 pagesOdontogenic Malignancies: Lee J. Slater, DDS, MSlaljadeff12No ratings yet
- Intraosseous Ameloblast 2004 Oral and Maxillofacial Surgery Clinics of NorthDocument14 pagesIntraosseous Ameloblast 2004 Oral and Maxillofacial Surgery Clinics of Northlaljadeff12No ratings yet
- Calcifying Odontogenic Cyst and Denti - 2004 - Oral and Maxillofacial Surgery CLDocument7 pagesCalcifying Odontogenic Cyst and Denti - 2004 - Oral and Maxillofacial Surgery CLlaljadeff12No ratings yet
- Secondary Correction of Midface FracturesDocument12 pagesSecondary Correction of Midface Fractureslaljadeff12No ratings yet
- Nonsyndromic Craniosynostosis Diagnosis - 2004 - Oral and Maxillofacial SurgerDocument17 pagesNonsyndromic Craniosynostosis Diagnosis - 2004 - Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Difficult Questions Facing The CR 2004 Oral and Maxillofacial Surgery ClinicDocument10 pagesDifficult Questions Facing The CR 2004 Oral and Maxillofacial Surgery Cliniclaljadeff12No ratings yet
- Positional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery CliniDocument8 pagesPositional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery Clinilaljadeff12No ratings yet
- Orthoptic Eval and Treatment in Orbital FracturesDocument10 pagesOrthoptic Eval and Treatment in Orbital Fractureslaljadeff12No ratings yet
- Primary Orbital Fracture RepairDocument27 pagesPrimary Orbital Fracture Repairlaljadeff12100% (1)
- Intraop Feedback and Quality ControlDocument12 pagesIntraop Feedback and Quality Controllaljadeff12No ratings yet
- Bioterrorism and Biologic Warfare: Sidney L. Bourgeois, JR, DDS, Michael J. Doherty, DDSDocument32 pagesBioterrorism and Biologic Warfare: Sidney L. Bourgeois, JR, DDS, Michael J. Doherty, DDSlaljadeff12No ratings yet
- Rejuvenation of The Anterior Neck 2014 Atlas of The Oral and MaxillofacialDocument12 pagesRejuvenation of The Anterior Neck 2014 Atlas of The Oral and Maxillofaciallaljadeff12No ratings yet
- Evidence Based Decision MakingDocument19 pagesEvidence Based Decision Makinglaljadeff12No ratings yet
- Upper Airway Hypoglossal Nerve Stimulation - 2019 - Atlas of The Oral and MaxiDocument6 pagesUpper Airway Hypoglossal Nerve Stimulation - 2019 - Atlas of The Oral and Maxilaljadeff12No ratings yet
- Anatomy of The OrbitsDocument18 pagesAnatomy of The Orbitslaljadeff12No ratings yet
- Short Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial SurgerDocument16 pagesShort Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Pediatric Tongue Base Surgery: Gi Soo Lee, MD, Edm, Umakanth Katwa, MDDocument5 pagesPediatric Tongue Base Surgery: Gi Soo Lee, MD, Edm, Umakanth Katwa, MDlaljadeff12No ratings yet
- Tonsillectomy and Pharyngoplasty: Tissue-Preserving TechniquesDocument6 pagesTonsillectomy and Pharyngoplasty: Tissue-Preserving Techniqueslaljadeff12No ratings yet
- Transoral Robotic Surgery For The - 2019 - Atlas of The Oral and Maxillofacial SDocument8 pagesTransoral Robotic Surgery For The - 2019 - Atlas of The Oral and Maxillofacial Slaljadeff12No ratings yet
- Glabellar Flaps For Reconstruction of Skin DefectsDocument6 pagesGlabellar Flaps For Reconstruction of Skin Defectslaljadeff12No ratings yet
- Nasal Surgery For Sleep-Disordered BreathingDocument6 pagesNasal Surgery For Sleep-Disordered Breathinglaljadeff12No ratings yet
- Rhomboid Flap - 2020 - Atlas of The Oral and Maxillofacial Surgery ClinicsDocument6 pagesRhomboid Flap - 2020 - Atlas of The Oral and Maxillofacial Surgery Clinicslaljadeff12No ratings yet
- Keystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDDocument14 pagesKeystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDlaljadeff12No ratings yet
- Cases - Oral Cysts 1Document42 pagesCases - Oral Cysts 1aya123mo7amedNo ratings yet
- Puspita - Monitoring Cotc & SOS SOMDocument36 pagesPuspita - Monitoring Cotc & SOS SOMIrwansyah DiahNo ratings yet
- A Critical Analysis of Bennett Movement 1Document18 pagesA Critical Analysis of Bennett Movement 1Rik ChatterjeeNo ratings yet
- Alvin B. Vibar, M.D.Document55 pagesAlvin B. Vibar, M.D.Ditas ChuNo ratings yet
- Hearing and BalanceDocument7 pagesHearing and BalanceGaby SanchezNo ratings yet
- Extraction of TeethDocument84 pagesExtraction of TeethAkram Thabet50% (2)
- Interception of Skeletal Class 3 Malocclusion With Frankle 3 Appliance in Late Mixed Dentition A Case ReportDocument6 pagesInterception of Skeletal Class 3 Malocclusion With Frankle 3 Appliance in Late Mixed Dentition A Case ReportLibardo García TolosaNo ratings yet
- HabitsDocument36 pagesHabitsMaitreyi LimayeNo ratings yet
- Botos Alexandra - Oral SemiologyDocument46 pagesBotos Alexandra - Oral SemiologyMaria OlteanNo ratings yet
- Ear Assessment 4Document49 pagesEar Assessment 4Feven AbrahamNo ratings yet
- 3 Case Report Geographic Tongue Haritsa BudimanDocument10 pages3 Case Report Geographic Tongue Haritsa Budimanharitsa budimanNo ratings yet
- Complicaciones Hilos PdoDocument3 pagesComplicaciones Hilos PdodominiqueNo ratings yet
- Gr10 Ch13.6 TBDocument6 pagesGr10 Ch13.6 TBnr46jpdxbpNo ratings yet
- On Seeing in The Dark - Remarks On The Evolution of The EyeDocument5 pagesOn Seeing in The Dark - Remarks On The Evolution of The EyeabbraxasNo ratings yet
- Anatomy Midterm 2Document92 pagesAnatomy Midterm 2Cassandra DavisNo ratings yet
- Periodontal Considerations Determining The Design and Location of Margins in Restorative DentistryDocument9 pagesPeriodontal Considerations Determining The Design and Location of Margins in Restorative DentistryAnonymous AyxIccS4aXNo ratings yet
- Szpilki Gis AngDocument2 pagesSzpilki Gis Angxpathetic.aestheticNo ratings yet
- USE OF TEMPORARY ANCHORAGE DEVICES IN INTRUSION OF SUPRAERUPTED MOLARS-case ReportsDocument9 pagesUSE OF TEMPORARY ANCHORAGE DEVICES IN INTRUSION OF SUPRAERUPTED MOLARS-case ReportsVesna AndreevskaNo ratings yet
- The TracheaDocument16 pagesThe TracheaMatende husseinNo ratings yet
- Orthodontist's Perceptions of Smile EstheticsA Questionnaire Based StudyDocument5 pagesOrthodontist's Perceptions of Smile EstheticsA Questionnaire Based StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Frenzel Techinique Eric FattahDocument7 pagesFrenzel Techinique Eric FattahJohan VandersmissenNo ratings yet
- Neodent Neoarch Immediate Fixed Full-Arch Solution Manual: Grand MorseDocument44 pagesNeodent Neoarch Immediate Fixed Full-Arch Solution Manual: Grand Morsewaf51No ratings yet
- CSF Rhinorrhea 2022Document396 pagesCSF Rhinorrhea 2022Daniel AraujoNo ratings yet
- Integumentary System NotesDocument7 pagesIntegumentary System NotesDale Gil JuliaNo ratings yet
- Differential FOrce Method of Orthodontic Treatment (1977) (Dragged) 3Document1 pageDifferential FOrce Method of Orthodontic Treatment (1977) (Dragged) 3MADANo ratings yet
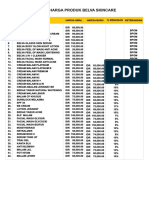
- Daftar Harga Belva Aesthetic ClinicDocument1 pageDaftar Harga Belva Aesthetic Clinicmas adiNo ratings yet
- Digital Workflow For The Rehabilitation of The Excessively Worn DentitionDocument26 pagesDigital Workflow For The Rehabilitation of The Excessively Worn Dentitionfloressam2000No ratings yet
- Jyotsna Rao - QRS 4th Year - Community Dentistry - Www.thedentalhub.org.InDocument64 pagesJyotsna Rao - QRS 4th Year - Community Dentistry - Www.thedentalhub.org.InHeyo HolaNo ratings yet
- PanoramikDocument38 pagesPanoramikStephanie Victoria100% (1)
- Micro Implanted Anchorage Safety Cortical Bone Thickness in IZCDocument5 pagesMicro Implanted Anchorage Safety Cortical Bone Thickness in IZCLisbethNo ratings yet