Download as pdf or txt
You might also like
- Geography - Study Guide - ANSWERS - Garret Nagle and Briony Cooke - Second Edition - Oxford 2017Document44 pagesGeography - Study Guide - ANSWERS - Garret Nagle and Briony Cooke - Second Edition - Oxford 2017Felix ShaoNo ratings yet
- Wpa PaperDocument12 pagesWpa Paperkhairul ezwan100% (1)
- What Next After 10th, Inter, DegreeDocument10 pagesWhat Next After 10th, Inter, DegreeBlue JaguarNo ratings yet
- A Randomized Controlled Trial of High-Intensity Interval Training and Inspiratory Muscle Training For Chronic Heart Failure Patients With Inspiratory Muscle WeaknessDocument15 pagesA Randomized Controlled Trial of High-Intensity Interval Training and Inspiratory Muscle Training For Chronic Heart Failure Patients With Inspiratory Muscle WeaknessAprilleo ViedroNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptThompson E IghaloNo ratings yet
- Physiotherapy Intervention As A Complementary Treatment For People Living With HIV/AIDSDocument19 pagesPhysiotherapy Intervention As A Complementary Treatment For People Living With HIV/AIDSNurul FitriaaNo ratings yet
- Psychological Response COVID Renal TXDocument5 pagesPsychological Response COVID Renal TXdrshhagarNo ratings yet
- Artigo Publicado PROTOCOLO Da TeseDocument8 pagesArtigo Publicado PROTOCOLO Da TeseRonivaldo L. DiasNo ratings yet
- Brazilian Journal of Physical TherapyDocument12 pagesBrazilian Journal of Physical TherapyKen ABNo ratings yet
- Exercise and Other Non-Pharmaceutical Interventions 2018Document10 pagesExercise and Other Non-Pharmaceutical Interventions 2018storm.ghirlandoNo ratings yet
- Multi-Professional Intervention in Adults With Arterial Hypertension: A Randomized Clinical TrialDocument7 pagesMulti-Professional Intervention in Adults With Arterial Hypertension: A Randomized Clinical TrialDesiati MaharaniNo ratings yet
- Journal of Clinical TrialsDocument10 pagesJournal of Clinical TrialsRodrigo DelgadoNo ratings yet
- Parhampour 2019 The Effects of Sixweek Resistance ADocument10 pagesParhampour 2019 The Effects of Sixweek Resistance AAmr Mohamed GalalNo ratings yet
- Isometric Handgrip-1Document9 pagesIsometric Handgrip-1Adi PramonoNo ratings yet
- 8 - Scheewe2012Document9 pages8 - Scheewe2012Sergio Machado NeurocientistaNo ratings yet
- 24 Ashraf Et AlDocument7 pages24 Ashraf Et AleditorijmrhsNo ratings yet
- Sharman 2014Document12 pagesSharman 2014Jorge Valiente FernandezNo ratings yet
- 10 7705@biomedica 4451Document13 pages10 7705@biomedica 4451Dhiyan GalehNo ratings yet
- Rehabilitasi CopdDocument8 pagesRehabilitasi CopdHenny RahmawatiNo ratings yet
- Self-Efficacy Among Indonesian Chronic Liver Disease PatientsDocument6 pagesSelf-Efficacy Among Indonesian Chronic Liver Disease PatientsIip Barudak CikoleNo ratings yet
- 1 s2.0 S2405587515300263 MainDocument8 pages1 s2.0 S2405587515300263 MainmaracioNo ratings yet
- The Relationship Between Sleep Disturbances and Quality of LifeDocument20 pagesThe Relationship Between Sleep Disturbances and Quality of LifeHusnan BimaNo ratings yet
- HHS Public Access: Intradialytic Activities and Health-Related Quality of Life Among Hemodialysis PatientsDocument16 pagesHHS Public Access: Intradialytic Activities and Health-Related Quality of Life Among Hemodialysis PatientslamyaaNo ratings yet
- High Intensity Interval Training Versus Moderate Intensity Continuous Training Within Cardiac Rehabilitation A Systematic Review and Meta AnalysisDocument18 pagesHigh Intensity Interval Training Versus Moderate Intensity Continuous Training Within Cardiac Rehabilitation A Systematic Review and Meta AnalysisAnatomska CentralaNo ratings yet
- IntervalexercisetrialAnnals2006 PDFDocument12 pagesIntervalexercisetrialAnnals2006 PDFrunmenNo ratings yet
- Reljic Et Al., 2021Document14 pagesReljic Et Al., 2021AILEENNo ratings yet
- Educational Program Patients With HypertensionDocument9 pagesEducational Program Patients With HypertensionRoy martadi NurmansyahNo ratings yet
- Validity of PSI and CURB-65 in PneumoniaDocument9 pagesValidity of PSI and CURB-65 in PneumoniaArdhito BudhijuwonoNo ratings yet
- Weight LossDocument13 pagesWeight Losskhan jeetNo ratings yet
- DFHDF DFJKJK DFDocument8 pagesDFHDF DFJKJK DFAndrés Araneda VásquezNo ratings yet
- 1 s2.0 S2531043718301107 MainDocument8 pages1 s2.0 S2531043718301107 MainCraniolyne RefianNo ratings yet
- Comparison of High-Intensity IDocument17 pagesComparison of High-Intensity IIulian-Stefan HOLUBIACNo ratings yet
- Ryan C Maves Uses of Procalcitonin As A Biomarker inDocument13 pagesRyan C Maves Uses of Procalcitonin As A Biomarker inrocky balboaaNo ratings yet
- Prevalence and Impact of Hepatitis On The Quality of Life of PatientsDocument5 pagesPrevalence and Impact of Hepatitis On The Quality of Life of PatientsjackleenNo ratings yet
- Journal Pone 0244850Document15 pagesJournal Pone 0244850yavy83No ratings yet
- In Critically Ill Adult Patients Community-Acquired Bloodstream InfectionDocument12 pagesIn Critically Ill Adult Patients Community-Acquired Bloodstream InfectionNeliel NoraNo ratings yet
- Guillen Barre y FisioterapiaDocument13 pagesGuillen Barre y FisioterapiaanaNo ratings yet
- Effects of HIIT On Aerobic Capacity in Cardiac Patients, A Sistematic Review With Metanalysis - 2017Document17 pagesEffects of HIIT On Aerobic Capacity in Cardiac Patients, A Sistematic Review With Metanalysis - 2017alarconscamilaNo ratings yet
- Rouben Off 2001Document7 pagesRouben Off 2001壮No ratings yet
- FocusDocument9 pagesFocusAdéline NolinNo ratings yet
- Research Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyDocument7 pagesResearch Article Telerehabilitation Using Fitness Application in Patients With Severe Cystic Fibrosis Awaiting Lung Transplant: A Pilot StudyBayu PrabuNo ratings yet
- 19417381221139343Document8 pages19417381221139343Thiago SartiNo ratings yet
- Low Level Viremia Is Associated With Serious Non-AIDS Events in People Living With HIVDocument20 pagesLow Level Viremia Is Associated With Serious Non-AIDS Events in People Living With HIVAbrahamKatimeNo ratings yet
- Coenzyme Q10 in Acute InfluenzaDocument7 pagesCoenzyme Q10 in Acute InfluenzaDaniNo ratings yet
- Fernandez Et Al 2023 Intrahospital Supervised Exercise Training Improves Survival Rate Among Hypertensive Patients WithDocument7 pagesFernandez Et Al 2023 Intrahospital Supervised Exercise Training Improves Survival Rate Among Hypertensive Patients WithAlexis Arce AlvarezNo ratings yet
- Pi Is 1098301516000267Document8 pagesPi Is 1098301516000267Avinash SivaNo ratings yet
- PHY2 8 E14455Document14 pagesPHY2 8 E14455Alexis Arce AlvarezNo ratings yet
- Pulmonary Impairment After Tuberculosis : Original ResearchDocument8 pagesPulmonary Impairment After Tuberculosis : Original ResearchPalaniappan MeyyappanNo ratings yet
- POTS EValuacion Del EjercicioDocument29 pagesPOTS EValuacion Del EjercicioAlfredoNo ratings yet
- Physical Activity, Cardiovascular Health, Quality of Life and Blood Pressure Control in Hypertensive Subjects: Randomized Clinical TrialDocument11 pagesPhysical Activity, Cardiovascular Health, Quality of Life and Blood Pressure Control in Hypertensive Subjects: Randomized Clinical TrialAlitNo ratings yet
- Effects of Combined Aerobic Strength Training Versus Fitness Education Program in CopdDocument9 pagesEffects of Combined Aerobic Strength Training Versus Fitness Education Program in Copdsana manzoorNo ratings yet
- Bouaziz Et Al., (2019) Effects of HIIT and Continuous Endurance TrainingDocument10 pagesBouaziz Et Al., (2019) Effects of HIIT and Continuous Endurance TrainingAna Flávia SordiNo ratings yet
- Effect of Evidence Based Lifestyle Guidelines On Self Efficacy of Patients With HypertensionDocument20 pagesEffect of Evidence Based Lifestyle Guidelines On Self Efficacy of Patients With HypertensionMuhammad DeddyNo ratings yet
- Physiology & Behavior: SciencedirectDocument8 pagesPhysiology & Behavior: SciencedirectScottNo ratings yet
- Non Exercise Estimated Cardiorespiratory Fitness and All Cause Mortality in Cancer PatientsDocument7 pagesNon Exercise Estimated Cardiorespiratory Fitness and All Cause Mortality in Cancer PatientsAthenaeum Scientific PublishersNo ratings yet
- Jurnal 5Document6 pagesJurnal 5Arswendo ValentinoNo ratings yet
- 2015 Article 241Document7 pages2015 Article 241hadiNo ratings yet
- Functional Outcome After Cardiac Rehabilitation AnDocument7 pagesFunctional Outcome After Cardiac Rehabilitation AnramonNo ratings yet
- Factors Influencing Heart Rate Variability: Stefan Sammito, Irina BöckelmannDocument5 pagesFactors Influencing Heart Rate Variability: Stefan Sammito, Irina BöckelmannHana Anggraeni PurnomoNo ratings yet
- Bernocchi-2018-Home-based Telerehabilitation IDocument7 pagesBernocchi-2018-Home-based Telerehabilitation IJonathanNo ratings yet
- ContentServer AspDocument8 pagesContentServer AspClauNo ratings yet
- High-Intensity Interval Training in Patients With Intermittent ClaudicationDocument13 pagesHigh-Intensity Interval Training in Patients With Intermittent ClaudicationAntónio José OliveiraNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Bjsports 2016 September 50-17-1030 Inline Supplementary Material 1Document5 pagesBjsports 2016 September 50-17-1030 Inline Supplementary Material 1Léo TavaresNo ratings yet
- 8688 Bas Tses Winter 2020 Online pg14 15889Document2 pages8688 Bas Tses Winter 2020 Online pg14 15889Léo TavaresNo ratings yet
- What Role Do Chronic Workloads Play in The Acute To Chronic Workload Ratio? Time To Dismiss ACWR and Its Underlying TheoryDocument12 pagesWhat Role Do Chronic Workloads Play in The Acute To Chronic Workload Ratio? Time To Dismiss ACWR and Its Underlying TheoryLéo TavaresNo ratings yet
- Nsca-Cpt Examination Detailed Content Outline: Cognitive LevelDocument5 pagesNsca-Cpt Examination Detailed Content Outline: Cognitive LevelLéo TavaresNo ratings yet
- The Specificity of Training Prescription and Physiological Assessment: A ReviewDocument17 pagesThe Specificity of Training Prescription and Physiological Assessment: A ReviewLéo TavaresNo ratings yet
- Periodization and Block Periodization in Sports .39Document21 pagesPeriodization and Block Periodization in Sports .39Léo TavaresNo ratings yet
- Hulin 2016Document6 pagesHulin 2016Léo TavaresNo ratings yet
- The Acute:chronic Workload Ratio Predicts Injury: High Chronic Workload May Decrease Injury Risk in Elite Rugby League PlayersDocument8 pagesThe Acute:chronic Workload Ratio Predicts Injury: High Chronic Workload May Decrease Injury Risk in Elite Rugby League PlayersLéo TavaresNo ratings yet
- Hulme 2018Document11 pagesHulme 2018Léo TavaresNo ratings yet
- Spikes in Acute Workload Are Associated With Increased Injury Risk in Elite Cricket Fast BowlersDocument5 pagesSpikes in Acute Workload Are Associated With Increased Injury Risk in Elite Cricket Fast BowlersLéo TavaresNo ratings yet
- 8688 Bas Tses Winter 2020 Online pg14 15889Document2 pages8688 Bas Tses Winter 2020 Online pg14 15889Léo TavaresNo ratings yet
- Volatility Forecasting - A Comparison of GARCH (1,1) and EWMA ModelsDocument14 pagesVolatility Forecasting - A Comparison of GARCH (1,1) and EWMA ModelsLéo TavaresNo ratings yet
- Proposal of A Global Training Load Measure PredictDocument8 pagesProposal of A Global Training Load Measure PredictLéo TavaresNo ratings yet
- LaTeX List - Enumerate and Itemize PDFDocument5 pagesLaTeX List - Enumerate and Itemize PDFchristal MIAKOUKILANo ratings yet
- 2009-11-05Document20 pages2009-11-05The University Daily KansanNo ratings yet
- Lab ManualDocument14 pagesLab Manualhak creationNo ratings yet
- Physics AS Level Formulas and DefinitionsDocument5 pagesPhysics AS Level Formulas and DefinitionsCharlene DaneekaNo ratings yet
- 2021 Nqesh Mock Test Set BDocument36 pages2021 Nqesh Mock Test Set Brandolf traigo100% (3)
- Alternative Disposal of Polystyrene Fish BoxesDocument2 pagesAlternative Disposal of Polystyrene Fish Boxesهزاع الفارسNo ratings yet
- CVPDocument20 pagesCVPThomas K. AddaiNo ratings yet
- IMMI Grant NotificationDocument4 pagesIMMI Grant NotificationAngeline GarciaNo ratings yet
- Itt420: Network and System Administration Lab Exercise 1Document5 pagesItt420: Network and System Administration Lab Exercise 1Nurul Shuhaini AidaNo ratings yet
- Safety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based InspectionsDocument3 pagesSafety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based Inspectionsi.kamalNo ratings yet
- Yeastar P-Series PBX System Datasheet enDocument7 pagesYeastar P-Series PBX System Datasheet enYemen BrokerNo ratings yet
- Kine 2p90 l19Document9 pagesKine 2p90 l19baileyschaefer28No ratings yet
- Ac Recovery Machine User Manual PDFDocument39 pagesAc Recovery Machine User Manual PDFmybdt1691No ratings yet
- Query ManualDocument37 pagesQuery ManualstraNo ratings yet
- Acmepacket4500 InstallationDocument112 pagesAcmepacket4500 InstallationfujiNo ratings yet
- Hanad General Trading Financial Statements 2023Document8 pagesHanad General Trading Financial Statements 2023Nyakwar Leoh NyabayaNo ratings yet
- BT08 PDFDocument4 pagesBT08 PDFAfdhalNo ratings yet
- Grade 8 Integrated Science Week 2 Lesson 2Document5 pagesGrade 8 Integrated Science Week 2 Lesson 2Balram HaroldNo ratings yet
- GregormendelandhispeasreadingandquestionsDocument2 pagesGregormendelandhispeasreadingandquestionsapi-248015505No ratings yet
- Chapter 3Document10 pagesChapter 3Adrian LohNo ratings yet
- Main Hydraulic System M315CDocument8 pagesMain Hydraulic System M315CMEULEYENo ratings yet
- Immersion PaperDocument21 pagesImmersion PaperCarl Justin BallertaNo ratings yet
- Lakefest Artist Vendor Application 09Document4 pagesLakefest Artist Vendor Application 09Jeffrey Alexander BrathwaiteNo ratings yet
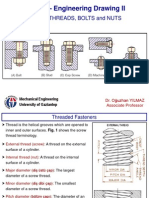
- SCREW THREADS, BOLTS and NUTS PDFDocument10 pagesSCREW THREADS, BOLTS and NUTS PDFhrhgk50% (2)
- Keysight U1251B and U1252B Handheld Digital Multimeter: User's and Service GuideDocument177 pagesKeysight U1251B and U1252B Handheld Digital Multimeter: User's and Service GuideAndi MulyanaNo ratings yet
- SuperDoctor5 UserGuideDocument139 pagesSuperDoctor5 UserGuidemlody45No ratings yet
- Gestational Hypertension - UTD PDFDocument21 pagesGestational Hypertension - UTD PDFShahar Perea ArizaNo ratings yet