
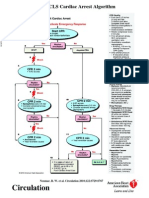
Pediatric Advanced Life Support: I. PALS System Approach Algorithm
Pediatric Advanced Life Support: I. PALS System Approach Algorithm
You might also like
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDocument1 pageAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNo ratings yet
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDocument3 pagesCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- Hollymatic Super: Operators Manual Parts ListDocument45 pagesHollymatic Super: Operators Manual Parts ListCarlosERodriguezA100% (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- ACLS Pharmacology Pretest Question Answers PDF (SET-2)Document9 pagesACLS Pharmacology Pretest Question Answers PDF (SET-2)김민길100% (1)
- Practice StripsDocument9 pagesPractice StripsErica Yamamoto50% (4)
- Algorithm-ACLS Electrical Cardioversion 200612Document1 pageAlgorithm-ACLS Electrical Cardioversion 200612Kavya ShreeNo ratings yet
- Irvine Welsh Ecstasy Three Tales of Chemical RomanceDocument43 pagesIrvine Welsh Ecstasy Three Tales of Chemical RomanceClara RuizNo ratings yet
- AHA-PALS 2010: Pediatric Chain of SurvivalDocument10 pagesAHA-PALS 2010: Pediatric Chain of SurvivalIsabel CastilloNo ratings yet
- ACLS Study Guide NewDocument35 pagesACLS Study Guide NewNIRANJANA SHALINI100% (1)
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocument3 pagesDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- Acls DrugsDocument10 pagesAcls DrugsChintami Octavia100% (1)
- ACLS MedicationsDocument31 pagesACLS MedicationscmirceaNo ratings yet
- Collective Bargaining, Strikes and The Quest For Industrial Peace in NigeriaDocument23 pagesCollective Bargaining, Strikes and The Quest For Industrial Peace in Nigeriafarad6a0% (1)
- ACLS Official GuideDocument11 pagesACLS Official GuideICU RSPGNo ratings yet
- ToxidromesDocument1 pageToxidromesMayer Rosenberg100% (7)
- Emergency Lecture PDFDocument57 pagesEmergency Lecture PDFDuane Liloc100% (1)
- EKG Quick Reference ChartDocument4 pagesEKG Quick Reference ChartMildaNo ratings yet
- ACLS Study Guide: Ecg Strip InterpretationDocument12 pagesACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (2)
- ACLS Training - Most Important Points To RememberDocument5 pagesACLS Training - Most Important Points To RememberEman ElzeftawyNo ratings yet
- CPR ACLS Study GuideDocument18 pagesCPR ACLS Study GuideJohn Phamacy100% (1)
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Rhythm Recognition - ACLS Medical Training 1Document9 pagesRhythm Recognition - ACLS Medical Training 1Catalina BorquezNo ratings yet
- Cardiovascular SYSTEM - Heart Dysrythmia IllustrationsDocument3 pagesCardiovascular SYSTEM - Heart Dysrythmia IllustrationsKim GonzalesNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- ACLS PharmacologyDocument5 pagesACLS PharmacologyKuruva MallikarjunaNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- Adenosine: Rapid IV PushDocument4 pagesAdenosine: Rapid IV PushsabboNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 pagesACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelNo ratings yet
- 10 Common EKG Heart Rhythms PDFDocument1 page10 Common EKG Heart Rhythms PDFtchanochNo ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- PALS Study GuideDocument12 pagesPALS Study GuidePrerna SehgalNo ratings yet
- 15 Item ACLS Drill With RationaleDocument12 pages15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- ECG Master Class-2Document138 pagesECG Master Class-2Shohag ID Center100% (1)
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- 17 Cardiac DrugsDocument6 pages17 Cardiac DrugshiwaralelataNo ratings yet
- Aha Acls Prep Packet 2021 NewDocument69 pagesAha Acls Prep Packet 2021 Newdim100% (2)
- Sample Acls For DummiesDocument3 pagesSample Acls For DummiesTodd Cole100% (1)
- Dosage CalculationsDocument39 pagesDosage Calculationssalak9462900% (1)
- Introd To ECG Code Blue Champs March 2019Document52 pagesIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- EKG - Basic Interpretation and ACLS PreparationDocument39 pagesEKG - Basic Interpretation and ACLS PreparationSergio Cano100% (2)
- ACLS Study Guide JULY 2021 UPDATEDocument3 pagesACLS Study Guide JULY 2021 UPDATENina Morada100% (3)
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- Drugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaDocument20 pagesDrugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaAfrida Sahestina100% (1)
- Ccu Survival GuideDocument10 pagesCcu Survival Guideomegasauron0gmailcom100% (1)
- ACLS Class Packet 2015Document9 pagesACLS Class Packet 2015Chi Wiin100% (3)
- Pals Que Estion and Answer FullDocument31 pagesPals Que Estion and Answer FullNeo Latoya MadunaNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- 7 Suggestions Paramedic Airway ANAM22 WMDocument5 pages7 Suggestions Paramedic Airway ANAM22 WMcedivadeniaNo ratings yet
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocument50 pagesAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNo ratings yet
- Drug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryDocument5 pagesDrug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryMarcel YoungNo ratings yet
- Paramedic Pediatric Scenario 2017Document3 pagesParamedic Pediatric Scenario 2017Chad StreetNo ratings yet
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Ok Ok Notes PediaDocument10 pagesOk Ok Notes PediaIsabel CastilloNo ratings yet
- Dermatology - Skin NeoplasmsDocument12 pagesDermatology - Skin NeoplasmsIsabel CastilloNo ratings yet
- Pedia Pre School NewsDocument3 pagesPedia Pre School NewsIsabel CastilloNo ratings yet
- Dermatology - Exanthematous Viral DiseasesDocument6 pagesDermatology - Exanthematous Viral DiseasesIsabel CastilloNo ratings yet
- DERMATOLOGY - Cuteneous Candidiasis, PityrosporumDocument4 pagesDERMATOLOGY - Cuteneous Candidiasis, PityrosporumIsabel CastilloNo ratings yet
- SURGICAL PATHOLOGY SOFT TISSUES TableDocument4 pagesSURGICAL PATHOLOGY SOFT TISSUES TableIsabel CastilloNo ratings yet
- EMBRYOGENESIS and Fetal DevtDocument50 pagesEMBRYOGENESIS and Fetal DevtIsabel CastilloNo ratings yet
- Surgical Pathology - CNSDocument2 pagesSurgical Pathology - CNSIsabel CastilloNo ratings yet
- Pediatric Therapeutics: Eximius 2021Document13 pagesPediatric Therapeutics: Eximius 2021Isabel CastilloNo ratings yet
- Diseases of The Newborn: ObjectivesDocument17 pagesDiseases of The Newborn: ObjectivesIsabel CastilloNo ratings yet
- Growth and DevelopmentDocument60 pagesGrowth and DevelopmentIsabel CastilloNo ratings yet
- Implantataion Placental Development and AbnormalitiesDocument62 pagesImplantataion Placental Development and AbnormalitiesIsabel CastilloNo ratings yet
- Acute and Chronic PancreatitisDocument8 pagesAcute and Chronic PancreatitisIsabel CastilloNo ratings yet
- Irritable Bowel SyndromeDocument3 pagesIrritable Bowel SyndromeIsabel CastilloNo ratings yet
- Pneumonia: TranscribersDocument6 pagesPneumonia: TranscribersIsabel CastilloNo ratings yet
- Pack-Years of Cigarette Smoking Is The Most HighlyDocument5 pagesPack-Years of Cigarette Smoking Is The Most HighlyIsabel CastilloNo ratings yet
- Inflammatory Bowel Disease: Microorganisms That Drive DiseaseDocument4 pagesInflammatory Bowel Disease: Microorganisms That Drive DiseaseIsabel CastilloNo ratings yet
- Adolescent Medicine: Early AdolescenceDocument2 pagesAdolescent Medicine: Early AdolescenceIsabel CastilloNo ratings yet
- Interatitial Lung DiseaseDocument2 pagesInteratitial Lung DiseaseIsabel CastilloNo ratings yet
- Causes of HypothyroidismDocument6 pagesCauses of HypothyroidismIsabel Castillo100% (1)
- Acute Appendicitis and Peritonitis: RLQ, To The Pelvis, Right FlankDocument4 pagesAcute Appendicitis and Peritonitis: RLQ, To The Pelvis, Right FlankIsabel CastilloNo ratings yet
- Mesenteric Vascular Insufficiency: ClassificationDocument2 pagesMesenteric Vascular Insufficiency: ClassificationIsabel CastilloNo ratings yet
- Hyperthyroidism: EpidemiologyDocument8 pagesHyperthyroidism: EpidemiologyIsabel CastilloNo ratings yet
- AsthmaDocument4 pagesAsthmaIsabel CastilloNo ratings yet
- Approach To The Patient With Disease of The Respiratory SystemDocument3 pagesApproach To The Patient With Disease of The Respiratory SystemIsabel CastilloNo ratings yet
- Diseases of Esophagus.Document3 pagesDiseases of Esophagus.Isabel Castillo100% (2)
- Anorectal Disease and Common Anorectal DisordersDocument2 pagesAnorectal Disease and Common Anorectal DisordersIsabel CastilloNo ratings yet
- Approach To Patients With Gastrointestinal Disease: Eximius 2021Document5 pagesApproach To Patients With Gastrointestinal Disease: Eximius 2021Isabel CastilloNo ratings yet
- Yield, Viscosity, and Gel Strength of Wami Tilapia (Oreochromis Urolepis Hornorum) Skin Gelatin: Optimization of The Extraction ProcessDocument9 pagesYield, Viscosity, and Gel Strength of Wami Tilapia (Oreochromis Urolepis Hornorum) Skin Gelatin: Optimization of The Extraction ProcessAMAANINo ratings yet
- Bod and CodDocument66 pagesBod and CodKamlesh Kamlesh EtwaroNo ratings yet
- Flow Controller TotalizerDocument3 pagesFlow Controller TotalizerDhiraj MistryNo ratings yet
- Tecnoseal Catalogo Anodos 16Document212 pagesTecnoseal Catalogo Anodos 16JorgeNo ratings yet
- Contract of ServiceDocument2 pagesContract of ServiceAnonymous 03JIPKRkNo ratings yet
- Epa242 PDFDocument4 pagesEpa242 PDFpapadafiNo ratings yet
- SA2 2014 English Course - ADocument8 pagesSA2 2014 English Course - AsunnyNo ratings yet
- 2012-07-24 Item 12 California Homeless Bill of RightsDocument8 pages2012-07-24 Item 12 California Homeless Bill of RightsToby NixonNo ratings yet
- Background Platelet-Rich Plasma (PRP) Therapy Is An Easy, Safe, Autologous, and Cheap BiologicDocument10 pagesBackground Platelet-Rich Plasma (PRP) Therapy Is An Easy, Safe, Autologous, and Cheap BiologicsandhiNo ratings yet
- O Level OrientationDocument4 pagesO Level OrientationKim NisarNo ratings yet
- Unstable Angina PectorisDocument35 pagesUnstable Angina PectorisAkbar IskandarNo ratings yet
- 3M Scotchkote - Custom Coating GuideDocument16 pages3M Scotchkote - Custom Coating GuideUgoRibeiroNo ratings yet
- Earth Compaction EquipmentDocument15 pagesEarth Compaction EquipmentÄmî Îíţ ŚHäh100% (1)
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- Rekapitulasi Absensi Pegawai Puskesmas Koto Baru BULAN: April 2019Document49 pagesRekapitulasi Absensi Pegawai Puskesmas Koto Baru BULAN: April 2019Tuti AgustiniNo ratings yet
- S1-TITAN Overview BrochureDocument8 pagesS1-TITAN Overview BrochureFedeNo ratings yet
- Lock WallaceDocument2 pagesLock WallaceVeronika CalanceaNo ratings yet
- Access - Catalog - DP&Casing Tools-15-18Document4 pagesAccess - Catalog - DP&Casing Tools-15-18RICHARDNo ratings yet
- Research Paper On Greenhouse Effect PDFDocument8 pagesResearch Paper On Greenhouse Effect PDFgz8reqdc100% (1)
- TDS ASP-epoxyCoveDocument2 pagesTDS ASP-epoxyCovetatenda mhuruNo ratings yet
- Lysosome PresentationDocument5 pagesLysosome Presentationapi-241502402No ratings yet
- Direct Deposit Authorization: 0122-DDAUTH-B66846Document2 pagesDirect Deposit Authorization: 0122-DDAUTH-B66846Jitendra SharmaNo ratings yet
- The Winners and Losers of GlobalizationDocument7 pagesThe Winners and Losers of GlobalizationRalucutsaNo ratings yet
- ECG LictureDocument25 pagesECG LictureALi NursingNo ratings yet
- Benzene Toluene & Xylene PurificationDocument2 pagesBenzene Toluene & Xylene PurificationvivekdkrpuNo ratings yet
- AdgfhDocument44 pagesAdgfhnurulNo ratings yet





















































































































Download as docx, pdf, or txt
You might also like
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDocument1 pageAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNo ratings yet
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDocument3 pagesCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- Hollymatic Super: Operators Manual Parts ListDocument45 pagesHollymatic Super: Operators Manual Parts ListCarlosERodriguezA100% (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- ACLS Pharmacology Pretest Question Answers PDF (SET-2)Document9 pagesACLS Pharmacology Pretest Question Answers PDF (SET-2)김민길100% (1)
- Practice StripsDocument9 pagesPractice StripsErica Yamamoto50% (4)
- Algorithm-ACLS Electrical Cardioversion 200612Document1 pageAlgorithm-ACLS Electrical Cardioversion 200612Kavya ShreeNo ratings yet
- Irvine Welsh Ecstasy Three Tales of Chemical RomanceDocument43 pagesIrvine Welsh Ecstasy Three Tales of Chemical RomanceClara RuizNo ratings yet
- AHA-PALS 2010: Pediatric Chain of SurvivalDocument10 pagesAHA-PALS 2010: Pediatric Chain of SurvivalIsabel CastilloNo ratings yet
- ACLS Study Guide NewDocument35 pagesACLS Study Guide NewNIRANJANA SHALINI100% (1)
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocument3 pagesDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- Acls DrugsDocument10 pagesAcls DrugsChintami Octavia100% (1)
- ACLS MedicationsDocument31 pagesACLS MedicationscmirceaNo ratings yet
- Collective Bargaining, Strikes and The Quest For Industrial Peace in NigeriaDocument23 pagesCollective Bargaining, Strikes and The Quest For Industrial Peace in Nigeriafarad6a0% (1)
- ACLS Official GuideDocument11 pagesACLS Official GuideICU RSPGNo ratings yet
- ToxidromesDocument1 pageToxidromesMayer Rosenberg100% (7)
- Emergency Lecture PDFDocument57 pagesEmergency Lecture PDFDuane Liloc100% (1)
- EKG Quick Reference ChartDocument4 pagesEKG Quick Reference ChartMildaNo ratings yet
- ACLS Study Guide: Ecg Strip InterpretationDocument12 pagesACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (2)
- ACLS Training - Most Important Points To RememberDocument5 pagesACLS Training - Most Important Points To RememberEman ElzeftawyNo ratings yet
- CPR ACLS Study GuideDocument18 pagesCPR ACLS Study GuideJohn Phamacy100% (1)
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- Rhythm Recognition - ACLS Medical Training 1Document9 pagesRhythm Recognition - ACLS Medical Training 1Catalina BorquezNo ratings yet
- Cardiovascular SYSTEM - Heart Dysrythmia IllustrationsDocument3 pagesCardiovascular SYSTEM - Heart Dysrythmia IllustrationsKim GonzalesNo ratings yet
- ICE DrugsDocument2 pagesICE DrugsRichelle FrondaNo ratings yet
- ACLS PharmacologyDocument5 pagesACLS PharmacologyKuruva MallikarjunaNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- Adenosine: Rapid IV PushDocument4 pagesAdenosine: Rapid IV PushsabboNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 pagesACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelNo ratings yet
- 10 Common EKG Heart Rhythms PDFDocument1 page10 Common EKG Heart Rhythms PDFtchanochNo ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- PALS Study GuideDocument12 pagesPALS Study GuidePrerna SehgalNo ratings yet
- 15 Item ACLS Drill With RationaleDocument12 pages15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- ECG Master Class-2Document138 pagesECG Master Class-2Shohag ID Center100% (1)
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- 17 Cardiac DrugsDocument6 pages17 Cardiac DrugshiwaralelataNo ratings yet
- Aha Acls Prep Packet 2021 NewDocument69 pagesAha Acls Prep Packet 2021 Newdim100% (2)
- Sample Acls For DummiesDocument3 pagesSample Acls For DummiesTodd Cole100% (1)
- Dosage CalculationsDocument39 pagesDosage Calculationssalak9462900% (1)
- Introd To ECG Code Blue Champs March 2019Document52 pagesIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- EKG - Basic Interpretation and ACLS PreparationDocument39 pagesEKG - Basic Interpretation and ACLS PreparationSergio Cano100% (2)
- ACLS Study Guide JULY 2021 UPDATEDocument3 pagesACLS Study Guide JULY 2021 UPDATENina Morada100% (3)
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- Drugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaDocument20 pagesDrugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaAfrida Sahestina100% (1)
- Ccu Survival GuideDocument10 pagesCcu Survival Guideomegasauron0gmailcom100% (1)
- ACLS Class Packet 2015Document9 pagesACLS Class Packet 2015Chi Wiin100% (3)
- Pals Que Estion and Answer FullDocument31 pagesPals Que Estion and Answer FullNeo Latoya MadunaNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- 7 Suggestions Paramedic Airway ANAM22 WMDocument5 pages7 Suggestions Paramedic Airway ANAM22 WMcedivadeniaNo ratings yet
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocument50 pagesAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNo ratings yet
- Drug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryDocument5 pagesDrug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryMarcel YoungNo ratings yet
- Paramedic Pediatric Scenario 2017Document3 pagesParamedic Pediatric Scenario 2017Chad StreetNo ratings yet
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Ok Ok Notes PediaDocument10 pagesOk Ok Notes PediaIsabel CastilloNo ratings yet
- Dermatology - Skin NeoplasmsDocument12 pagesDermatology - Skin NeoplasmsIsabel CastilloNo ratings yet
- Pedia Pre School NewsDocument3 pagesPedia Pre School NewsIsabel CastilloNo ratings yet
- Dermatology - Exanthematous Viral DiseasesDocument6 pagesDermatology - Exanthematous Viral DiseasesIsabel CastilloNo ratings yet
- DERMATOLOGY - Cuteneous Candidiasis, PityrosporumDocument4 pagesDERMATOLOGY - Cuteneous Candidiasis, PityrosporumIsabel CastilloNo ratings yet
- SURGICAL PATHOLOGY SOFT TISSUES TableDocument4 pagesSURGICAL PATHOLOGY SOFT TISSUES TableIsabel CastilloNo ratings yet
- EMBRYOGENESIS and Fetal DevtDocument50 pagesEMBRYOGENESIS and Fetal DevtIsabel CastilloNo ratings yet
- Surgical Pathology - CNSDocument2 pagesSurgical Pathology - CNSIsabel CastilloNo ratings yet
- Pediatric Therapeutics: Eximius 2021Document13 pagesPediatric Therapeutics: Eximius 2021Isabel CastilloNo ratings yet
- Diseases of The Newborn: ObjectivesDocument17 pagesDiseases of The Newborn: ObjectivesIsabel CastilloNo ratings yet
- Growth and DevelopmentDocument60 pagesGrowth and DevelopmentIsabel CastilloNo ratings yet
- Implantataion Placental Development and AbnormalitiesDocument62 pagesImplantataion Placental Development and AbnormalitiesIsabel CastilloNo ratings yet
- Acute and Chronic PancreatitisDocument8 pagesAcute and Chronic PancreatitisIsabel CastilloNo ratings yet
- Irritable Bowel SyndromeDocument3 pagesIrritable Bowel SyndromeIsabel CastilloNo ratings yet
- Pneumonia: TranscribersDocument6 pagesPneumonia: TranscribersIsabel CastilloNo ratings yet
- Pack-Years of Cigarette Smoking Is The Most HighlyDocument5 pagesPack-Years of Cigarette Smoking Is The Most HighlyIsabel CastilloNo ratings yet
- Inflammatory Bowel Disease: Microorganisms That Drive DiseaseDocument4 pagesInflammatory Bowel Disease: Microorganisms That Drive DiseaseIsabel CastilloNo ratings yet
- Adolescent Medicine: Early AdolescenceDocument2 pagesAdolescent Medicine: Early AdolescenceIsabel CastilloNo ratings yet
- Interatitial Lung DiseaseDocument2 pagesInteratitial Lung DiseaseIsabel CastilloNo ratings yet
- Causes of HypothyroidismDocument6 pagesCauses of HypothyroidismIsabel Castillo100% (1)
- Acute Appendicitis and Peritonitis: RLQ, To The Pelvis, Right FlankDocument4 pagesAcute Appendicitis and Peritonitis: RLQ, To The Pelvis, Right FlankIsabel CastilloNo ratings yet
- Mesenteric Vascular Insufficiency: ClassificationDocument2 pagesMesenteric Vascular Insufficiency: ClassificationIsabel CastilloNo ratings yet
- Hyperthyroidism: EpidemiologyDocument8 pagesHyperthyroidism: EpidemiologyIsabel CastilloNo ratings yet
- AsthmaDocument4 pagesAsthmaIsabel CastilloNo ratings yet
- Approach To The Patient With Disease of The Respiratory SystemDocument3 pagesApproach To The Patient With Disease of The Respiratory SystemIsabel CastilloNo ratings yet
- Diseases of Esophagus.Document3 pagesDiseases of Esophagus.Isabel Castillo100% (2)
- Anorectal Disease and Common Anorectal DisordersDocument2 pagesAnorectal Disease and Common Anorectal DisordersIsabel CastilloNo ratings yet
- Approach To Patients With Gastrointestinal Disease: Eximius 2021Document5 pagesApproach To Patients With Gastrointestinal Disease: Eximius 2021Isabel CastilloNo ratings yet
- Yield, Viscosity, and Gel Strength of Wami Tilapia (Oreochromis Urolepis Hornorum) Skin Gelatin: Optimization of The Extraction ProcessDocument9 pagesYield, Viscosity, and Gel Strength of Wami Tilapia (Oreochromis Urolepis Hornorum) Skin Gelatin: Optimization of The Extraction ProcessAMAANINo ratings yet
- Bod and CodDocument66 pagesBod and CodKamlesh Kamlesh EtwaroNo ratings yet
- Flow Controller TotalizerDocument3 pagesFlow Controller TotalizerDhiraj MistryNo ratings yet
- Tecnoseal Catalogo Anodos 16Document212 pagesTecnoseal Catalogo Anodos 16JorgeNo ratings yet
- Contract of ServiceDocument2 pagesContract of ServiceAnonymous 03JIPKRkNo ratings yet
- Epa242 PDFDocument4 pagesEpa242 PDFpapadafiNo ratings yet
- SA2 2014 English Course - ADocument8 pagesSA2 2014 English Course - AsunnyNo ratings yet
- 2012-07-24 Item 12 California Homeless Bill of RightsDocument8 pages2012-07-24 Item 12 California Homeless Bill of RightsToby NixonNo ratings yet
- Background Platelet-Rich Plasma (PRP) Therapy Is An Easy, Safe, Autologous, and Cheap BiologicDocument10 pagesBackground Platelet-Rich Plasma (PRP) Therapy Is An Easy, Safe, Autologous, and Cheap BiologicsandhiNo ratings yet
- O Level OrientationDocument4 pagesO Level OrientationKim NisarNo ratings yet
- Unstable Angina PectorisDocument35 pagesUnstable Angina PectorisAkbar IskandarNo ratings yet
- 3M Scotchkote - Custom Coating GuideDocument16 pages3M Scotchkote - Custom Coating GuideUgoRibeiroNo ratings yet
- Earth Compaction EquipmentDocument15 pagesEarth Compaction EquipmentÄmî Îíţ ŚHäh100% (1)
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- Rekapitulasi Absensi Pegawai Puskesmas Koto Baru BULAN: April 2019Document49 pagesRekapitulasi Absensi Pegawai Puskesmas Koto Baru BULAN: April 2019Tuti AgustiniNo ratings yet
- S1-TITAN Overview BrochureDocument8 pagesS1-TITAN Overview BrochureFedeNo ratings yet
- Lock WallaceDocument2 pagesLock WallaceVeronika CalanceaNo ratings yet
- Access - Catalog - DP&Casing Tools-15-18Document4 pagesAccess - Catalog - DP&Casing Tools-15-18RICHARDNo ratings yet
- Research Paper On Greenhouse Effect PDFDocument8 pagesResearch Paper On Greenhouse Effect PDFgz8reqdc100% (1)
- TDS ASP-epoxyCoveDocument2 pagesTDS ASP-epoxyCovetatenda mhuruNo ratings yet
- Lysosome PresentationDocument5 pagesLysosome Presentationapi-241502402No ratings yet
- Direct Deposit Authorization: 0122-DDAUTH-B66846Document2 pagesDirect Deposit Authorization: 0122-DDAUTH-B66846Jitendra SharmaNo ratings yet
- The Winners and Losers of GlobalizationDocument7 pagesThe Winners and Losers of GlobalizationRalucutsaNo ratings yet
- ECG LictureDocument25 pagesECG LictureALi NursingNo ratings yet
- Benzene Toluene & Xylene PurificationDocument2 pagesBenzene Toluene & Xylene PurificationvivekdkrpuNo ratings yet
- AdgfhDocument44 pagesAdgfhnurulNo ratings yet