Download as docx, pdf, or txt
You might also like
- EMREE. UAE Emirates BluePrintDocument32 pagesEMREE. UAE Emirates BluePrintDhienda Laddy NasrulNo ratings yet
- Medical Certificate: To Whom It May ConcernDocument8 pagesMedical Certificate: To Whom It May Concernvissia guzmanNo ratings yet
- (DTP) Approved Joint DOH-NNC Devolution Transition Plan - March 24, 2022 (1) (1) FOR HRH 2Document19 pages(DTP) Approved Joint DOH-NNC Devolution Transition Plan - March 24, 2022 (1) (1) FOR HRH 2Arabella CatindoyNo ratings yet
- Kawasaki DiseaseDocument18 pagesKawasaki DiseaseCharm ArroyoNo ratings yet
- Neonatal Pneumonia Case StudyDocument2 pagesNeonatal Pneumonia Case StudyAngel Villamor0% (1)
- National Leprosy Control ProgramDocument3 pagesNational Leprosy Control ProgramKrizle Adaza100% (1)
- Anemia Unspecified FinalDocument47 pagesAnemia Unspecified FinalMaria Paula BungayNo ratings yet
- Chlamydia Research PaperDocument3 pagesChlamydia Research Paperapi-313987677No ratings yet
- Tuberculosis - TB - Pathophysiology - Schematic DiagramDocument3 pagesTuberculosis - TB - Pathophysiology - Schematic DiagramCyrus De Asis90% (10)
- Pneumonia Case Study FinalllDocument56 pagesPneumonia Case Study Finalllbethrice melegritoNo ratings yet
- Non-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The AmericasDocument2 pagesNon-Modifiable Factor Modifiable Factor: South-East Asia, Eastern, Mediterranean, Western Pacific, and The Americaschristian quiaoitNo ratings yet
- Pcap PathoDocument2 pagesPcap PathoLardel CarayNo ratings yet
- Acute PyelonephritisDocument24 pagesAcute PyelonephritisChristine Karen Ang Suarez100% (1)
- I. Population: Sex Ratio 96 Males: 100 Females InterpretationDocument25 pagesI. Population: Sex Ratio 96 Males: 100 Females InterpretationanreilegardeNo ratings yet
- Group 3 Abruptio Placentae Revised Case StudyDocument87 pagesGroup 3 Abruptio Placentae Revised Case StudyXena IngalNo ratings yet
- Journal Pcap CDocument3 pagesJournal Pcap CKit LaraNo ratings yet
- Acute PyelonephritisDocument105 pagesAcute Pyelonephritisyasira50% (2)
- IMCI Learning FeedbackDocument1 pageIMCI Learning Feedbackinah krizia lagueNo ratings yet
- Head To Toe Assessment of Infant CsepreDocument5 pagesHead To Toe Assessment of Infant CsepreteuuuuNo ratings yet
- NCPDocument2 pagesNCPDaryl Paglinawan100% (1)
- Case Study: College of NursingDocument3 pagesCase Study: College of NursingVincent PolicarNo ratings yet
- Case 1 (Pneumonia) ArioDocument26 pagesCase 1 (Pneumonia) ArioJoegie ArioNo ratings yet
- Teaching PlanDocument1 pageTeaching PlanUnis OwtwoNo ratings yet
- BSN2F-2C Pcap Case-Pres Final-OutputDocument76 pagesBSN2F-2C Pcap Case-Pres Final-OutputLeaNo ratings yet
- Journal Study Regarding PCAP WashingtonDocument1 pageJournal Study Regarding PCAP WashingtonLuis WashingtonNo ratings yet
- Benign Febrile ConvulsionDocument10 pagesBenign Febrile ConvulsionJuan Luis C. SingsonNo ratings yet
- Common Side Effects of Oxytocin Include:: CNS: Maternal: COMADocument3 pagesCommon Side Effects of Oxytocin Include:: CNS: Maternal: COMAann camposNo ratings yet
- PCAP FinalDocument28 pagesPCAP FinalAmiebelle Naval0% (2)
- Case Study Benign Tumors of The Uterus: MyomaDocument3 pagesCase Study Benign Tumors of The Uterus: MyomaToto RyanNo ratings yet
- Pathophysiology of Abortion Case Study (Vizconde, Ehreiz Raiden C. BSN2-A)Document4 pagesPathophysiology of Abortion Case Study (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- Name - Kleah Comillo - BSN1 (Chapter5)Document2 pagesName - Kleah Comillo - BSN1 (Chapter5)Holyver TabarnillaNo ratings yet
- CATAINA, Maria Elizabeth D. - Case-scenario-DRDocument3 pagesCATAINA, Maria Elizabeth D. - Case-scenario-DRMarielle CatainaNo ratings yet
- NCPDocument7 pagesNCPJulianne Jeamer FabroaNo ratings yet
- Case (Acute Gastroenteritis) Group 4Document36 pagesCase (Acute Gastroenteritis) Group 4EljhayrosNo ratings yet
- Case Study PcapDocument3 pagesCase Study PcapClaire PalaciosNo ratings yet
- Pediatric Community Acquired Pneumonia (Pecap) : Case StudyDocument32 pagesPediatric Community Acquired Pneumonia (Pecap) : Case StudyR Hornilla ArcegaNo ratings yet
- In Partial Fulfillment of The Requirements in Care of Mother and Child and Adolescent 217 Related Learning ExperienceDocument28 pagesIn Partial Fulfillment of The Requirements in Care of Mother and Child and Adolescent 217 Related Learning ExperienceAllyssa BunagNo ratings yet
- Cabingaojb BSN 2a Imci Case ScenarioDocument6 pagesCabingaojb BSN 2a Imci Case ScenarioJulia CabingaoNo ratings yet
- A Case Study of Acute GastroenteritisDocument42 pagesA Case Study of Acute GastroenteritisGelah DacanayNo ratings yet
- Balyan in The Context of 21st Century PhilippinesDocument1 pageBalyan in The Context of 21st Century PhilippinesA. J. SantosNo ratings yet
- RLE 109 Group 4 Case Analysis in MastitisDocument20 pagesRLE 109 Group 4 Case Analysis in MastitisEugene MananganNo ratings yet
- "Uterine Leiomyoma " A Case Study: Saint Mary's University School of Health and Natural SciencesDocument75 pages"Uterine Leiomyoma " A Case Study: Saint Mary's University School of Health and Natural SciencesKyla CarbonelNo ratings yet
- CPD Concept MapDocument1 pageCPD Concept MapShandle Dynne Baena100% (1)
- Midyr Case Study NewDocument18 pagesMidyr Case Study NewAndres Ham Samson BernabeNo ratings yet
- FNCP @@@@@Document33 pagesFNCP @@@@@Sheryl Ann Barit PedinesNo ratings yet
- NCP Neonatal SepsisDocument1 pageNCP Neonatal SepsisGen-GenMedranoGirayNo ratings yet
- COMPLETE CS - Acute PyelonephritisDocument53 pagesCOMPLETE CS - Acute Pyelonephritisyasira100% (1)
- Influenza PATHOPHYSIOLOGYDocument3 pagesInfluenza PATHOPHYSIOLOGYElle RosalesNo ratings yet
- Concept Map UTI PregnantDocument2 pagesConcept Map UTI PregnantChriz LechNo ratings yet
- Dengue Health Teaching PlanDocument6 pagesDengue Health Teaching PlanMae VisperasNo ratings yet
- 04 Community Diagnosis Talandang 1 NEW DataDocument43 pages04 Community Diagnosis Talandang 1 NEW DataLeslie Noreen AguilarNo ratings yet
- Journal Pcap CDocument3 pagesJournal Pcap CKit Lara50% (2)
- Atrial Septal Defect - 7 Year OldDocument1 pageAtrial Septal Defect - 7 Year OldMSNo ratings yet
- Acute PyelonephritisDocument22 pagesAcute PyelonephritisAmaizing Grace Mejia Carlos75% (4)
- Reflection On MCN LECDocument12 pagesReflection On MCN LECLecery Sophia WongNo ratings yet
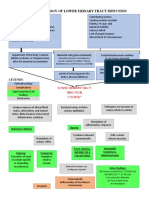
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- Drug StudyDocument6 pagesDrug StudyMiru มิริวNo ratings yet
- Urinary Tract Infectio Case StudyDocument17 pagesUrinary Tract Infectio Case Studyjunex123No ratings yet
- Group1 HTP Dengue-FinalDocument9 pagesGroup1 HTP Dengue-FinalCHRISTINE GRACE ELLONo ratings yet
- Dengue Prevention Health Teaching 09-16-10Document3 pagesDengue Prevention Health Teaching 09-16-10Bakushido100% (2)
- Marjorie A. Carganilla BSN 3-2 Pathophysiology of Urinaryy Tract Infection Precipitating FactorsDocument8 pagesMarjorie A. Carganilla BSN 3-2 Pathophysiology of Urinaryy Tract Infection Precipitating FactorsMarjorie CarganillaNo ratings yet
- Case Study (APN)Document10 pagesCase Study (APN)ErleNo ratings yet
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentErleNo ratings yet
- 13 Areas of AssessmentDocument4 pages13 Areas of AssessmentKryzza LeizellNo ratings yet
- Childhood Multisystem Inflammatory Syndrome With PDocument5 pagesChildhood Multisystem Inflammatory Syndrome With PGiska VelindaNo ratings yet
- FinalthesisoftuberculosisDocument86 pagesFinalthesisoftuberculosisOuaingar ngueadoumNo ratings yet
- Clinical Lab Report: Test Result Flags Ref. Range UnitsDocument1 pageClinical Lab Report: Test Result Flags Ref. Range UnitsMichaela HessonNo ratings yet
- KP COVID ReportDocument2 pagesKP COVID ReportBal Mukund JhaNo ratings yet
- Bardac 208M - APIC CSPA PosterDocument1 pageBardac 208M - APIC CSPA PosterDyaniNo ratings yet
- FscommoncoldDocument2 pagesFscommoncoldhakmoch hakmNo ratings yet
- Grip StrengthDocument11 pagesGrip StrengthMiguel Angel HermosilloNo ratings yet
- Systemic Lupus ErythematosusDocument8 pagesSystemic Lupus ErythematosusthemanofthepeacefulwarNo ratings yet
- Unbreakable Minds Documentary AssignmentDocument6 pagesUnbreakable Minds Documentary Assignmentbonnie moenNo ratings yet
- Pub - Epidemics and Pandemics Their Impacts On Human His PDFDocument526 pagesPub - Epidemics and Pandemics Their Impacts On Human His PDFana ionescu100% (1)
- Resource Chart Medical Eligibility Contraceptives EnglishDocument1 pageResource Chart Medical Eligibility Contraceptives EnglishGoh Zheng YuenNo ratings yet
- Consolidated TB Guidelines For Zambia Final VersionDocument169 pagesConsolidated TB Guidelines For Zambia Final VersionFred PupeNo ratings yet
- MycoDot PIDocument4 pagesMycoDot PITanveer100% (1)
- ColonosDocument27 pagesColonoshyunsuh255100% (1)
- EvolDocument11 pagesEvolpharmaNo ratings yet
- Ekso SpecsDocument2 pagesEkso SpecsJames Felton KeithNo ratings yet
- CHN 145 QuestionsDocument46 pagesCHN 145 QuestionsAlyssaGrandeMontimorNo ratings yet
- How Is Balanitis Treated Answers From DoctorsDocument1 pageHow Is Balanitis Treated Answers From Doctorsyaseen bahramandNo ratings yet
- Dermatitis Herpetiformis CDAC PP 508Document2 pagesDermatitis Herpetiformis CDAC PP 508D U N I A A N I M ENo ratings yet
- Diagnosis and Recent Therapy of Fixed Drug EruptionDocument14 pagesDiagnosis and Recent Therapy of Fixed Drug EruptionSheilaNo ratings yet
- A Dictionary of Epidemiology, 6th Edition Publisher: Oxford University Press Editor: Miguel PortaDocument3 pagesA Dictionary of Epidemiology, 6th Edition Publisher: Oxford University Press Editor: Miguel PortaMarkoNo ratings yet
- клостридиен миозит PDFDocument1 pageклостридиен миозит PDFDrivailaNo ratings yet
- Wiwik Pratiwi Jafar - PO714241211040 - DIV TK.1A FISIOTERAPIDocument1 pageWiwik Pratiwi Jafar - PO714241211040 - DIV TK.1A FISIOTERAPIAndi Resky AisyahNo ratings yet
- GorantlaDocument18 pagesGorantlaapi-464986748No ratings yet
- NeuroblastomaDocument10 pagesNeuroblastomadita100% (1)
- Eczema and DermatitisDocument47 pagesEczema and DermatitisDeborah ChemutaiNo ratings yet