
Q410.2cole 2006
Q410.2cole 2006
You might also like
- Farnsworth D 15 English PDFDocument4 pagesFarnsworth D 15 English PDFdian eka saputraNo ratings yet
- A Completed Example of Long Term Planning Cambridge Primary Science Guide p.16 17Document2 pagesA Completed Example of Long Term Planning Cambridge Primary Science Guide p.16 17Omar A. Mohammad100% (1)
- Grading Scales in OptometryDocument4 pagesGrading Scales in Optometrynaravichandran3662No ratings yet
- (AIIMS MDS Question PaperDocument20 pages(AIIMS MDS Question Papersavyasachin100% (1)
- Druthers March 2021Document12 pagesDruthers March 2021ThomasZiehmer100% (1)
- ColourDocument5 pagesColourRoyal Rajput Kamini SinghNo ratings yet
- Evaluation of New Rapid Plasma Reagin Card Screening Test For SyphilisDocument5 pagesEvaluation of New Rapid Plasma Reagin Card Screening Test For SyphilisDewa Ayu WidiadnyasariNo ratings yet
- Colour Vision TestsDocument9 pagesColour Vision Testsbforte09No ratings yet
- Color Blindness PresentationDocument22 pagesColor Blindness PresentationNgan HuynhNo ratings yet
- Diagnostic Signs of Accommodative InsufficiencyDocument7 pagesDiagnostic Signs of Accommodative InsufficiencyNorina Abdul GaforNo ratings yet
- Reynolds 1992Document3 pagesReynolds 1992snhmaitlaNo ratings yet
- Colour Vision - NajwaDocument52 pagesColour Vision - NajwaNajwa MansuriNo ratings yet
- Jurnal UtamaDocument4 pagesJurnal UtamaAmaluddinNo ratings yet
- Optometry: Clinical Colour Vision TestsDocument18 pagesOptometry: Clinical Colour Vision TestsPayel BeraNo ratings yet
- RP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormDocument6 pagesRP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormPinak PatelNo ratings yet
- Effects of Contrast Sensitivity On Colour Vision TestingDocument33 pagesEffects of Contrast Sensitivity On Colour Vision TestingDorothy Eugene Nindya WiharyantoNo ratings yet
- Butler 2019Document6 pagesButler 2019oldDEUSNo ratings yet
- Carruthers2008 Crows LinesDocument6 pagesCarruthers2008 Crows LinesArmin Arceo DuranNo ratings yet
- Aviation Ophthalmology Aviation Ophthalmology: DR Anthony Evans Chief, Aviation Medicine Section ICAO, MontrealDocument33 pagesAviation Ophthalmology Aviation Ophthalmology: DR Anthony Evans Chief, Aviation Medicine Section ICAO, MontrealNasan EnkhbaatarNo ratings yet
- Evolution of Colour Vision Testing PDFDocument10 pagesEvolution of Colour Vision Testing PDFDhivya SekarNo ratings yet
- Term 2 Block Test AnswersDocument12 pagesTerm 2 Block Test AnswersSheila ChaiNo ratings yet
- Cormack-Lehane Classification Revisited - BritishDocument3 pagesCormack-Lehane Classification Revisited - BritishAbdul HamidNo ratings yet
- LLLLDocument4 pagesLLLLWailmer PailNo ratings yet
- Clinical Color Vision Testing and Correlation With Visual FunctionDocument8 pagesClinical Color Vision Testing and Correlation With Visual FunctionPierre A. RodulfoNo ratings yet
- A Review On Color Vision Deficiency-408Document4 pagesA Review On Color Vision Deficiency-408Macarena AlvarezNo ratings yet
- VDRL SifilisDocument3 pagesVDRL SifilisNadia OktarinaNo ratings yet
- Singh 1999Document6 pagesSingh 1999Camille Louise LlaveNo ratings yet
- Validation Study of The Sniffin' Sticks'' Olfactory Test in A British Population: A Preliminary CommunicationDocument5 pagesValidation Study of The Sniffin' Sticks'' Olfactory Test in A British Population: A Preliminary CommunicationCoryza Gabrie tanNo ratings yet
- II. Entubacao - 2. (05) Cormack-Lehane Classification RevisitedDocument8 pagesII. Entubacao - 2. (05) Cormack-Lehane Classification RevisitedicaroNo ratings yet
- Para Red and Toluidine Red Pigments: Standard Test Methods ForDocument2 pagesPara Red and Toluidine Red Pigments: Standard Test Methods ForShaker QaidiNo ratings yet
- EXPERIMENT 5 - Chroamtorgraphy GRP9 RevDocument2 pagesEXPERIMENT 5 - Chroamtorgraphy GRP9 RevMic100% (2)
- VanishDocument6 pagesVanishArturo GuilliemNo ratings yet
- 3rd Report Color Blind TestingDocument10 pages3rd Report Color Blind Testingbertha tandiNo ratings yet
- Clinical Picture: Barry L Cole, Ross W HarrisDocument1 pageClinical Picture: Barry L Cole, Ross W HarrisjovanaNo ratings yet
- Analysis of Chiral Pharmaceuticals Using HPLC With CD DetectionDocument6 pagesAnalysis of Chiral Pharmaceuticals Using HPLC With CD DetectionAnonymous Shv3RwsWnrNo ratings yet
- Radhakrishnanand2008 PDFDocument5 pagesRadhakrishnanand2008 PDFnayelyNo ratings yet
- Ishihara 24 Plate Instructions IDocument3 pagesIshihara 24 Plate Instructions ItabetiaekNo ratings yet
- Blood and BloodstainsDocument27 pagesBlood and BloodstainsPrincess Mae EstabilloNo ratings yet
- Color Vision TestDocument4 pagesColor Vision Testa194801No ratings yet
- Normal Values For The Pelli-RobsonDocument6 pagesNormal Values For The Pelli-RobsonPutri kartiniNo ratings yet
- Cormack - Lehane Classification Revisited: Respiration and The AirwayDocument8 pagesCormack - Lehane Classification Revisited: Respiration and The AirwayhendranopNo ratings yet
- Mahinay Forensic Chemistry and ToxicologyDocument192 pagesMahinay Forensic Chemistry and Toxicologykurtjoshuason21No ratings yet
- ChromaaaaaalateDocument7 pagesChromaaaaaalateVanessaOlgaJ.DagondonNo ratings yet
- The Use of 1% Toluidine Blue Eye Drops in The Diagnosis of Ocular Surface Squamous Neoplasia Romero2013Document4 pagesThe Use of 1% Toluidine Blue Eye Drops in The Diagnosis of Ocular Surface Squamous Neoplasia Romero2013PamelaNo ratings yet
- Diagnostic Usefulness of Dermoscopy in Differentiating Lichen Aureus From Nummular EczemaDocument5 pagesDiagnostic Usefulness of Dermoscopy in Differentiating Lichen Aureus From Nummular EczemaFebrian AlfaroNo ratings yet
- Forensic Chemistry 2023Document19 pagesForensic Chemistry 2023Ada DukesNo ratings yet
- Forensic ChemistryDocument19 pagesForensic ChemistryAda DukesNo ratings yet
- RD rMADocument2 pagesRD rMAOsama TaghlebiNo ratings yet
- Droll 2012 Journal of EndodonticsDocument6 pagesDroll 2012 Journal of EndodonticsjassNo ratings yet
- Lemon1995 PDFDocument6 pagesLemon1995 PDFpalliNo ratings yet
- Ishihara - 38Document20 pagesIshihara - 38alinblohNo ratings yet
- Development of Computerized Color Vision Testing As A Replacement For Martin LanternDocument5 pagesDevelopment of Computerized Color Vision Testing As A Replacement For Martin LanternameliaNo ratings yet
- TLC Chromatography ExpDocument8 pagesTLC Chromatography ExpQistina NayliNo ratings yet
- 1516251256fsc p9 m25 E-TextDocument15 pages1516251256fsc p9 m25 E-TextpartikNo ratings yet
- FR 15 Farnsworth and LanthonyD15 Instructions Rev 1.7 0506Document7 pagesFR 15 Farnsworth and LanthonyD15 Instructions Rev 1.7 0506Muchammad Karunia Fadillah100% (1)
- Incorporating New, Bright Fluorochromes Into Multicolor Panel DesignDocument49 pagesIncorporating New, Bright Fluorochromes Into Multicolor Panel DesignKarla Novoa PérezNo ratings yet
- Stain Removal From A Silicone Maxillofacial ElastomerDocument5 pagesStain Removal From A Silicone Maxillofacial ElastomerAmar BhochhibhoyaNo ratings yet
- Loss of Heterozygosity at Chromosomes 8P, 9P, and 14Q Is Associated With Stage and Grade of Non-Papillary Renal Cell CarcinomasDocument5 pagesLoss of Heterozygosity at Chromosomes 8P, 9P, and 14Q Is Associated With Stage and Grade of Non-Papillary Renal Cell CarcinomasSarly FebrianaNo ratings yet
- DRAQ5 InfoDocument2 pagesDRAQ5 InfoHenry AmirNo ratings yet
- IJMLR121603Document7 pagesIJMLR121603sandeep raiNo ratings yet
- Problem 08 Just A Heel PrickDocument18 pagesProblem 08 Just A Heel PrickHid Dymple AhmadNo ratings yet
- Light and Colour Theories, and their relation to light and colour standardizationFrom EverandLight and Colour Theories, and their relation to light and colour standardizationNo ratings yet
- Alan PocinkiDocument33 pagesAlan PocinkiGèniaNo ratings yet
- SACE-2: SECTION 309-According To Section 309 of The Indian Penal Code (IPC) "Whoever AttemptsDocument6 pagesSACE-2: SECTION 309-According To Section 309 of The Indian Penal Code (IPC) "Whoever AttemptsSankalp PariharNo ratings yet
- W Wom Manual 112712Document18 pagesW Wom Manual 112712wahyuhendrosNo ratings yet
- Egress & Fire Protection L&I v1Document29 pagesEgress & Fire Protection L&I v1Areiffz IsmailNo ratings yet
- Current Good Manufacturing Practice - Fda CGMPDocument3 pagesCurrent Good Manufacturing Practice - Fda CGMPckbhaiNo ratings yet
- Evidence Based PracticeDocument4 pagesEvidence Based PracticeChandu RajNo ratings yet
- Full Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All ChapterDocument69 pagesFull Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All Chapterjustinesmedt868100% (5)
- DX Infective Endocarditis PDFDocument7 pagesDX Infective Endocarditis PDFSherree HayesNo ratings yet
- Efficacy of Computer Based Developmental Pediatric Screening (CBDPS)Document5 pagesEfficacy of Computer Based Developmental Pediatric Screening (CBDPS)RuchitaNo ratings yet
- Capella Arts Technical & Vocational Institute IncDocument6 pagesCapella Arts Technical & Vocational Institute IncHestia HDNo ratings yet
- Office of The Secretary: OpcjwDocument2 pagesOffice of The Secretary: OpcjwRichard FallegaNo ratings yet
- Finance (Pay Cell) Department G.O.Ms - No.306, Dated 13 October 2017Document15 pagesFinance (Pay Cell) Department G.O.Ms - No.306, Dated 13 October 2017manikandan andiappanNo ratings yet
- Office of The District Medical and Health Officer: Kurnool Notification No.03/NHM/2021, Dated: 07.08.2021Document9 pagesOffice of The District Medical and Health Officer: Kurnool Notification No.03/NHM/2021, Dated: 07.08.2021srikanth PosaNo ratings yet
- Material Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseDocument14 pagesMaterial Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseAri BinukoNo ratings yet
- Ca4 - The Use of Enzyme Supplements in Shrimp DietsDocument20 pagesCa4 - The Use of Enzyme Supplements in Shrimp DietsSrivatsava RajagopalanNo ratings yet
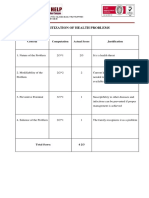
- Prioritization of Health Problems: ParenthoodDocument3 pagesPrioritization of Health Problems: ParenthoodMariana Mikaela AlagarNo ratings yet
- Miliaria-An Update: August 2017Document9 pagesMiliaria-An Update: August 2017Shafira TamaraNo ratings yet
- Sec 1 2023 NEW Unit 7Document7 pagesSec 1 2023 NEW Unit 7Wagdy MohammedNo ratings yet
- TeksolDocument5 pagesTeksolniki fitraNo ratings yet
- Current Therapeutic Research: SciencedirectDocument7 pagesCurrent Therapeutic Research: SciencedirectannisNo ratings yet
- The Rehabilitation Council of India Act, 1992Document12 pagesThe Rehabilitation Council of India Act, 1992Disability Rights AllianceNo ratings yet
- Biosafety SOPDocument4 pagesBiosafety SOPIsam SalehNo ratings yet
- Shell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsDocument2 pagesShell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsandriNo ratings yet
- Try Out 3 2019: Mata Pelajaran: Bahasa Inggris Jenjang: Sma/Ma Ipa Waktu: 120 MenitDocument50 pagesTry Out 3 2019: Mata Pelajaran: Bahasa Inggris Jenjang: Sma/Ma Ipa Waktu: 120 MenitEnglish ClassNo ratings yet
- Office of The Family and Children'S OmbudsDocument79 pagesOffice of The Family and Children'S OmbudsKING 5 NewsNo ratings yet
- Data Sheet Sample For SlaeemDocument3 pagesData Sheet Sample For SlaeemmuhannadNo ratings yet
- Role of Digital Therapeutics and The Changing Future of HealthcareDocument7 pagesRole of Digital Therapeutics and The Changing Future of HealthcareDavy DaveNo ratings yet
























































































Download as pdf or txt
You might also like
- Farnsworth D 15 English PDFDocument4 pagesFarnsworth D 15 English PDFdian eka saputraNo ratings yet
- A Completed Example of Long Term Planning Cambridge Primary Science Guide p.16 17Document2 pagesA Completed Example of Long Term Planning Cambridge Primary Science Guide p.16 17Omar A. Mohammad100% (1)
- Grading Scales in OptometryDocument4 pagesGrading Scales in Optometrynaravichandran3662No ratings yet
- (AIIMS MDS Question PaperDocument20 pages(AIIMS MDS Question Papersavyasachin100% (1)
- Druthers March 2021Document12 pagesDruthers March 2021ThomasZiehmer100% (1)
- ColourDocument5 pagesColourRoyal Rajput Kamini SinghNo ratings yet
- Evaluation of New Rapid Plasma Reagin Card Screening Test For SyphilisDocument5 pagesEvaluation of New Rapid Plasma Reagin Card Screening Test For SyphilisDewa Ayu WidiadnyasariNo ratings yet
- Colour Vision TestsDocument9 pagesColour Vision Testsbforte09No ratings yet
- Color Blindness PresentationDocument22 pagesColor Blindness PresentationNgan HuynhNo ratings yet
- Diagnostic Signs of Accommodative InsufficiencyDocument7 pagesDiagnostic Signs of Accommodative InsufficiencyNorina Abdul GaforNo ratings yet
- Reynolds 1992Document3 pagesReynolds 1992snhmaitlaNo ratings yet
- Colour Vision - NajwaDocument52 pagesColour Vision - NajwaNajwa MansuriNo ratings yet
- Jurnal UtamaDocument4 pagesJurnal UtamaAmaluddinNo ratings yet
- Optometry: Clinical Colour Vision TestsDocument18 pagesOptometry: Clinical Colour Vision TestsPayel BeraNo ratings yet
- RP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormDocument6 pagesRP-HPLC Method Development and Validation For The Estimation of Diclofenac Sodium, Tramadol Hydrochloride and Chlorzoxazone From Their Combined Tablet Dosage FormPinak PatelNo ratings yet
- Effects of Contrast Sensitivity On Colour Vision TestingDocument33 pagesEffects of Contrast Sensitivity On Colour Vision TestingDorothy Eugene Nindya WiharyantoNo ratings yet
- Butler 2019Document6 pagesButler 2019oldDEUSNo ratings yet
- Carruthers2008 Crows LinesDocument6 pagesCarruthers2008 Crows LinesArmin Arceo DuranNo ratings yet
- Aviation Ophthalmology Aviation Ophthalmology: DR Anthony Evans Chief, Aviation Medicine Section ICAO, MontrealDocument33 pagesAviation Ophthalmology Aviation Ophthalmology: DR Anthony Evans Chief, Aviation Medicine Section ICAO, MontrealNasan EnkhbaatarNo ratings yet
- Evolution of Colour Vision Testing PDFDocument10 pagesEvolution of Colour Vision Testing PDFDhivya SekarNo ratings yet
- Term 2 Block Test AnswersDocument12 pagesTerm 2 Block Test AnswersSheila ChaiNo ratings yet
- Cormack-Lehane Classification Revisited - BritishDocument3 pagesCormack-Lehane Classification Revisited - BritishAbdul HamidNo ratings yet
- LLLLDocument4 pagesLLLLWailmer PailNo ratings yet
- Clinical Color Vision Testing and Correlation With Visual FunctionDocument8 pagesClinical Color Vision Testing and Correlation With Visual FunctionPierre A. RodulfoNo ratings yet
- A Review On Color Vision Deficiency-408Document4 pagesA Review On Color Vision Deficiency-408Macarena AlvarezNo ratings yet
- VDRL SifilisDocument3 pagesVDRL SifilisNadia OktarinaNo ratings yet
- Singh 1999Document6 pagesSingh 1999Camille Louise LlaveNo ratings yet
- Validation Study of The Sniffin' Sticks'' Olfactory Test in A British Population: A Preliminary CommunicationDocument5 pagesValidation Study of The Sniffin' Sticks'' Olfactory Test in A British Population: A Preliminary CommunicationCoryza Gabrie tanNo ratings yet
- II. Entubacao - 2. (05) Cormack-Lehane Classification RevisitedDocument8 pagesII. Entubacao - 2. (05) Cormack-Lehane Classification RevisitedicaroNo ratings yet
- Para Red and Toluidine Red Pigments: Standard Test Methods ForDocument2 pagesPara Red and Toluidine Red Pigments: Standard Test Methods ForShaker QaidiNo ratings yet
- EXPERIMENT 5 - Chroamtorgraphy GRP9 RevDocument2 pagesEXPERIMENT 5 - Chroamtorgraphy GRP9 RevMic100% (2)
- VanishDocument6 pagesVanishArturo GuilliemNo ratings yet
- 3rd Report Color Blind TestingDocument10 pages3rd Report Color Blind Testingbertha tandiNo ratings yet
- Clinical Picture: Barry L Cole, Ross W HarrisDocument1 pageClinical Picture: Barry L Cole, Ross W HarrisjovanaNo ratings yet
- Analysis of Chiral Pharmaceuticals Using HPLC With CD DetectionDocument6 pagesAnalysis of Chiral Pharmaceuticals Using HPLC With CD DetectionAnonymous Shv3RwsWnrNo ratings yet
- Radhakrishnanand2008 PDFDocument5 pagesRadhakrishnanand2008 PDFnayelyNo ratings yet
- Ishihara 24 Plate Instructions IDocument3 pagesIshihara 24 Plate Instructions ItabetiaekNo ratings yet
- Blood and BloodstainsDocument27 pagesBlood and BloodstainsPrincess Mae EstabilloNo ratings yet
- Color Vision TestDocument4 pagesColor Vision Testa194801No ratings yet
- Normal Values For The Pelli-RobsonDocument6 pagesNormal Values For The Pelli-RobsonPutri kartiniNo ratings yet
- Cormack - Lehane Classification Revisited: Respiration and The AirwayDocument8 pagesCormack - Lehane Classification Revisited: Respiration and The AirwayhendranopNo ratings yet
- Mahinay Forensic Chemistry and ToxicologyDocument192 pagesMahinay Forensic Chemistry and Toxicologykurtjoshuason21No ratings yet
- ChromaaaaaalateDocument7 pagesChromaaaaaalateVanessaOlgaJ.DagondonNo ratings yet
- The Use of 1% Toluidine Blue Eye Drops in The Diagnosis of Ocular Surface Squamous Neoplasia Romero2013Document4 pagesThe Use of 1% Toluidine Blue Eye Drops in The Diagnosis of Ocular Surface Squamous Neoplasia Romero2013PamelaNo ratings yet
- Diagnostic Usefulness of Dermoscopy in Differentiating Lichen Aureus From Nummular EczemaDocument5 pagesDiagnostic Usefulness of Dermoscopy in Differentiating Lichen Aureus From Nummular EczemaFebrian AlfaroNo ratings yet
- Forensic Chemistry 2023Document19 pagesForensic Chemistry 2023Ada DukesNo ratings yet
- Forensic ChemistryDocument19 pagesForensic ChemistryAda DukesNo ratings yet
- RD rMADocument2 pagesRD rMAOsama TaghlebiNo ratings yet
- Droll 2012 Journal of EndodonticsDocument6 pagesDroll 2012 Journal of EndodonticsjassNo ratings yet
- Lemon1995 PDFDocument6 pagesLemon1995 PDFpalliNo ratings yet
- Ishihara - 38Document20 pagesIshihara - 38alinblohNo ratings yet
- Development of Computerized Color Vision Testing As A Replacement For Martin LanternDocument5 pagesDevelopment of Computerized Color Vision Testing As A Replacement For Martin LanternameliaNo ratings yet
- TLC Chromatography ExpDocument8 pagesTLC Chromatography ExpQistina NayliNo ratings yet
- 1516251256fsc p9 m25 E-TextDocument15 pages1516251256fsc p9 m25 E-TextpartikNo ratings yet
- FR 15 Farnsworth and LanthonyD15 Instructions Rev 1.7 0506Document7 pagesFR 15 Farnsworth and LanthonyD15 Instructions Rev 1.7 0506Muchammad Karunia Fadillah100% (1)
- Incorporating New, Bright Fluorochromes Into Multicolor Panel DesignDocument49 pagesIncorporating New, Bright Fluorochromes Into Multicolor Panel DesignKarla Novoa PérezNo ratings yet
- Stain Removal From A Silicone Maxillofacial ElastomerDocument5 pagesStain Removal From A Silicone Maxillofacial ElastomerAmar BhochhibhoyaNo ratings yet
- Loss of Heterozygosity at Chromosomes 8P, 9P, and 14Q Is Associated With Stage and Grade of Non-Papillary Renal Cell CarcinomasDocument5 pagesLoss of Heterozygosity at Chromosomes 8P, 9P, and 14Q Is Associated With Stage and Grade of Non-Papillary Renal Cell CarcinomasSarly FebrianaNo ratings yet
- DRAQ5 InfoDocument2 pagesDRAQ5 InfoHenry AmirNo ratings yet
- IJMLR121603Document7 pagesIJMLR121603sandeep raiNo ratings yet
- Problem 08 Just A Heel PrickDocument18 pagesProblem 08 Just A Heel PrickHid Dymple AhmadNo ratings yet
- Light and Colour Theories, and their relation to light and colour standardizationFrom EverandLight and Colour Theories, and their relation to light and colour standardizationNo ratings yet
- Alan PocinkiDocument33 pagesAlan PocinkiGèniaNo ratings yet
- SACE-2: SECTION 309-According To Section 309 of The Indian Penal Code (IPC) "Whoever AttemptsDocument6 pagesSACE-2: SECTION 309-According To Section 309 of The Indian Penal Code (IPC) "Whoever AttemptsSankalp PariharNo ratings yet
- W Wom Manual 112712Document18 pagesW Wom Manual 112712wahyuhendrosNo ratings yet
- Egress & Fire Protection L&I v1Document29 pagesEgress & Fire Protection L&I v1Areiffz IsmailNo ratings yet
- Current Good Manufacturing Practice - Fda CGMPDocument3 pagesCurrent Good Manufacturing Practice - Fda CGMPckbhaiNo ratings yet
- Evidence Based PracticeDocument4 pagesEvidence Based PracticeChandu RajNo ratings yet
- Full Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All ChapterDocument69 pagesFull Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All Chapterjustinesmedt868100% (5)
- DX Infective Endocarditis PDFDocument7 pagesDX Infective Endocarditis PDFSherree HayesNo ratings yet
- Efficacy of Computer Based Developmental Pediatric Screening (CBDPS)Document5 pagesEfficacy of Computer Based Developmental Pediatric Screening (CBDPS)RuchitaNo ratings yet
- Capella Arts Technical & Vocational Institute IncDocument6 pagesCapella Arts Technical & Vocational Institute IncHestia HDNo ratings yet
- Office of The Secretary: OpcjwDocument2 pagesOffice of The Secretary: OpcjwRichard FallegaNo ratings yet
- Finance (Pay Cell) Department G.O.Ms - No.306, Dated 13 October 2017Document15 pagesFinance (Pay Cell) Department G.O.Ms - No.306, Dated 13 October 2017manikandan andiappanNo ratings yet
- Office of The District Medical and Health Officer: Kurnool Notification No.03/NHM/2021, Dated: 07.08.2021Document9 pagesOffice of The District Medical and Health Officer: Kurnool Notification No.03/NHM/2021, Dated: 07.08.2021srikanth PosaNo ratings yet
- Material Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseDocument14 pagesMaterial Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseAri BinukoNo ratings yet
- Ca4 - The Use of Enzyme Supplements in Shrimp DietsDocument20 pagesCa4 - The Use of Enzyme Supplements in Shrimp DietsSrivatsava RajagopalanNo ratings yet
- Prioritization of Health Problems: ParenthoodDocument3 pagesPrioritization of Health Problems: ParenthoodMariana Mikaela AlagarNo ratings yet
- Miliaria-An Update: August 2017Document9 pagesMiliaria-An Update: August 2017Shafira TamaraNo ratings yet
- Sec 1 2023 NEW Unit 7Document7 pagesSec 1 2023 NEW Unit 7Wagdy MohammedNo ratings yet
- TeksolDocument5 pagesTeksolniki fitraNo ratings yet
- Current Therapeutic Research: SciencedirectDocument7 pagesCurrent Therapeutic Research: SciencedirectannisNo ratings yet
- The Rehabilitation Council of India Act, 1992Document12 pagesThe Rehabilitation Council of India Act, 1992Disability Rights AllianceNo ratings yet
- Biosafety SOPDocument4 pagesBiosafety SOPIsam SalehNo ratings yet
- Shell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsDocument2 pagesShell Advance 4T AX5 10W-30 (SL/MA) : Performance, Features & Benefits Specifications, Approvals & RecommendationsandriNo ratings yet
- Try Out 3 2019: Mata Pelajaran: Bahasa Inggris Jenjang: Sma/Ma Ipa Waktu: 120 MenitDocument50 pagesTry Out 3 2019: Mata Pelajaran: Bahasa Inggris Jenjang: Sma/Ma Ipa Waktu: 120 MenitEnglish ClassNo ratings yet
- Office of The Family and Children'S OmbudsDocument79 pagesOffice of The Family and Children'S OmbudsKING 5 NewsNo ratings yet
- Data Sheet Sample For SlaeemDocument3 pagesData Sheet Sample For SlaeemmuhannadNo ratings yet
- Role of Digital Therapeutics and The Changing Future of HealthcareDocument7 pagesRole of Digital Therapeutics and The Changing Future of HealthcareDavy DaveNo ratings yet