Download as pdf or txt
You might also like
- Final FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future CandidatesDocument56 pagesFinal FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future Candidatesjahangirealam89% (9)
- Palliative Care HandbookDocument81 pagesPalliative Care Handbookgeoaisla50% (2)
- Understanding Bone Cement Implantation Syndrome: Cheryl B. Hines, Edd, CrnaDocument9 pagesUnderstanding Bone Cement Implantation Syndrome: Cheryl B. Hines, Edd, CrnaAgil Rumboko SumitroNo ratings yet
- Pain Assessment and ManagementDocument37 pagesPain Assessment and ManagementRNdrei dela Cruz100% (3)
- Effect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialDocument24 pagesEffect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialRiyan W. PratamaNo ratings yet
- Comparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaDocument3 pagesComparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaFranz Josef TariganNo ratings yet
- PIIS0007091219306270Document3 pagesPIIS0007091219306270irvan rahmanNo ratings yet
- Hyperbaric Spinal For Elective Cesarean Section: - Ropivacaine Vs BupivacaineDocument13 pagesHyperbaric Spinal For Elective Cesarean Section: - Ropivacaine Vs BupivacaineYayaNo ratings yet
- 226-Article Text-421-2-10-20180506 2Document6 pages226-Article Text-421-2-10-20180506 2jt9sh7gfb5No ratings yet
- Tiempo de ApendicectomíaDocument9 pagesTiempo de Apendicectomíagustavoazapata533No ratings yet
- Analgesic Efficacity of Pfannenstiel Incision Infiltration With Ropivacaine 7.5Mg/Ml For Caesarean SectionDocument17 pagesAnalgesic Efficacity of Pfannenstiel Incision Infiltration With Ropivacaine 7.5Mg/Ml For Caesarean SectionboblenazeNo ratings yet
- Br. J. Anaesth. 2012 Abdallah 679 87Document9 pagesBr. J. Anaesth. 2012 Abdallah 679 87Christian Adiputra WijayaNo ratings yet
- Preoperative Paravertebral Block and Chronic Pain After Breast Cancer Surgery: A Double-Blind Randomized TrialDocument13 pagesPreoperative Paravertebral Block and Chronic Pain After Breast Cancer Surgery: A Double-Blind Randomized TrialRafly SuwandhiNo ratings yet
- Original Article: ISSN: 0976 3325Document4 pagesOriginal Article: ISSN: 0976 3325Rizka Leonita FahmyNo ratings yet
- Efficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDocument4 pagesEfficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDr shehwarNo ratings yet
- International Journal of Obstetric AnesthesiaDocument6 pagesInternational Journal of Obstetric Anesthesiaanita pratiwiNo ratings yet
- A Comparative Study of Intravenous Paracetamol and Ketorolac For Postoperative Analgesia Following Laproscopic CholecystectomyDocument6 pagesA Comparative Study of Intravenous Paracetamol and Ketorolac For Postoperative Analgesia Following Laproscopic CholecystectomyAmrit singhNo ratings yet
- Anesth Analg 2009 Lee 252 4Document3 pagesAnesth Analg 2009 Lee 252 4Ican DoitNo ratings yet
- Chronobiology of Labour Pain Perception: An Observational StudyDocument3 pagesChronobiology of Labour Pain Perception: An Observational StudydrszigetilearnNo ratings yet
- Agonista GNRH Histeroscopia OKDocument5 pagesAgonista GNRH Histeroscopia OKDalva Silva LimaNo ratings yet
- Management of Acute Osteoporotic Vertebral FracturDocument9 pagesManagement of Acute Osteoporotic Vertebral Fracturdaniel martinNo ratings yet
- Evaluation of Atosiban Therapy in The Management of Preterm Labour in Indian PatientsDocument37 pagesEvaluation of Atosiban Therapy in The Management of Preterm Labour in Indian PatientsSanjay NavaleNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Osteoarthritis (OA) - CM Plex Cream Study by DR KraemerDocument9 pagesOsteoarthritis (OA) - CM Plex Cream Study by DR KraemerHisWellnessNo ratings yet
- 1 s2.0 S0007091217366175 MainDocument5 pages1 s2.0 S0007091217366175 MainMeutia LaksaniNo ratings yet
- Evaluation of Postoperative Analgesic Consumption After Emergency and Elective Cesarean SectionDocument4 pagesEvaluation of Postoperative Analgesic Consumption After Emergency and Elective Cesarean Sectionsikeu resrohulNo ratings yet
- Evaluation of Postoperative Analgesic Consumption After Emergency and Elective Cesarean SectionDocument4 pagesEvaluation of Postoperative Analgesic Consumption After Emergency and Elective Cesarean Sectionsikeu resrohulNo ratings yet
- Acta Obstet Gynecol Scand - 2003 - AndersenDocument4 pagesActa Obstet Gynecol Scand - 2003 - AndersenArnl HqNo ratings yet
- Randomized-Controlled Trial of Intravenous AcetaminophenDocument6 pagesRandomized-Controlled Trial of Intravenous Acetaminophenclara giovaniNo ratings yet
- Metamizole (Dipyrone) As An Additive To Lidocaine For Intravenous Regional AnesthesiaDocument5 pagesMetamizole (Dipyrone) As An Additive To Lidocaine For Intravenous Regional AnesthesiaelsahewuniNo ratings yet
- 96FB0D241252Document4 pages96FB0D241252Adzana Yasadhy Hangga PrasetyoNo ratings yet
- Tugas Analisa Journal Dengan Format Picot (Wayan)Document6 pagesTugas Analisa Journal Dengan Format Picot (Wayan)I wayan suryawidanaNo ratings yet
- Paracetamol vs. Dexketoprofen PDFDocument5 pagesParacetamol vs. Dexketoprofen PDFMikeNo ratings yet
- Articulo 1 ObesidadDocument4 pagesArticulo 1 ObesidadOsiris AleitaNo ratings yet
- Is Granisetron-Dexamethasone Combination Better ThanDocument8 pagesIs Granisetron-Dexamethasone Combination Better ThanGustomo PanantroNo ratings yet
- Mullin 2002Document6 pagesMullin 2002Khairun NisaNo ratings yet
- J Neurol Sci (Turk)Document9 pagesJ Neurol Sci (Turk)nulaeli Siti ANo ratings yet
- JC Oncology55211005Document32 pagesJC Oncology55211005Neenuch ManeenuchNo ratings yet
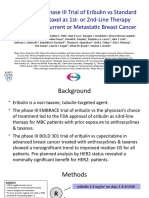
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocument14 pagesRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNo ratings yet
- Gastrectomia 2018Document5 pagesGastrectomia 2018Zara DekeNo ratings yet
- Table 1.: Assessment of ResponseDocument1 pageTable 1.: Assessment of ResponsejoycechicagoNo ratings yet
- Mccubbin 2015Document7 pagesMccubbin 2015Imelva GirsangNo ratings yet
- MIFEPREX™ (Mifepristone) Tablets, 200 MG For Oral Administration OnlyDocument16 pagesMIFEPREX™ (Mifepristone) Tablets, 200 MG For Oral Administration OnlyIniya RajendranNo ratings yet
- Perrone 2015Document6 pagesPerrone 2015alihumoodhasanNo ratings yet
- A Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeDocument10 pagesA Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeLibay Villamor IsmaelNo ratings yet
- Acupuncture and Related Techniques For Postoperative PainDocument10 pagesAcupuncture and Related Techniques For Postoperative PainmacbooklinoNo ratings yet
- Fsurg 05 00059Document10 pagesFsurg 05 00059nadaNo ratings yet
- 10 1016@j Jmig 2020 08 075Document1 page10 1016@j Jmig 2020 08 075Sedeeq Al-KhazrajiNo ratings yet
- Postoperative Pain ManagementDocument43 pagesPostoperative Pain ManagementPingKikiNo ratings yet
- OFA Bariatric Surgery Poster Euroanesthesia 2023Document1 pageOFA Bariatric Surgery Poster Euroanesthesia 2023Nataša SojčićNo ratings yet
- Hyaluronic Acid Single Intra-Articular Injection IDocument12 pagesHyaluronic Acid Single Intra-Articular Injection IMos Viorel DanutNo ratings yet
- MisoprostolDocument6 pagesMisoprostolmichelle1945No ratings yet
- Judul Kodetahundesign Study: 1 Agabegi 2011 Controlled, Prospective, RandomizedDocument20 pagesJudul Kodetahundesign Study: 1 Agabegi 2011 Controlled, Prospective, RandomizedRizky PratamaNo ratings yet
- Rhytmic Pattern Pca CancerDocument8 pagesRhytmic Pattern Pca CancerAida TantriNo ratings yet
- Effect of Ovariectomy On The Levels of Plasma Sex Hormones in Albino Rats E. A. Alagwu., R. O. NneliDocument5 pagesEffect of Ovariectomy On The Levels of Plasma Sex Hormones in Albino Rats E. A. Alagwu., R. O. NneliCaroline AgathaNo ratings yet
- Spinalvolfor LSCSDocument5 pagesSpinalvolfor LSCSmaurice falzonNo ratings yet
- Kelly 1996Document3 pagesKelly 1996Agustin CuryNo ratings yet
- Apm 20072Document7 pagesApm 20072ida wahyuni mapsanNo ratings yet
- Predictors of Pain Resolution After Varicocelectomy For Painful VaricoceleDocument5 pagesPredictors of Pain Resolution After Varicocelectomy For Painful VaricoceleMuhammad AndilaNo ratings yet
- Postoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - IdDocument23 pagesPostoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - Idsatria divaNo ratings yet
- Abstracts From The Global Embolization Sympo 2021 Journal of Vascular and inDocument21 pagesAbstracts From The Global Embolization Sympo 2021 Journal of Vascular and infreedy freedyNo ratings yet
- 360-Article Text-1516-1-10-20211019Document4 pages360-Article Text-1516-1-10-20211019Ottofianus Alvedo Hewick KalangiNo ratings yet
- 12076Document7 pages12076Muhammad ZiaNo ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- Doppler-Based Renal Resistive Index For Prediction of Acute Kidney Injury in Critically Ill Patients - A Systematic Review and Meta-AnalysisDocument14 pagesDoppler-Based Renal Resistive Index For Prediction of Acute Kidney Injury in Critically Ill Patients - A Systematic Review and Meta-AnalysisMiftah Furqon AuliaNo ratings yet
- Manuscrip SSH. EngDocument10 pagesManuscrip SSH. EngMiftah Furqon AuliaNo ratings yet
- Limratana 2020Document6 pagesLimratana 2020Miftah Furqon AuliaNo ratings yet
- Weiniger 2018Document8 pagesWeiniger 2018Miftah Furqon AuliaNo ratings yet
- Impact of Intra-Operative Dexamethasone After Scheduled Cesarean Delivery: A Retrospective StudyDocument8 pagesImpact of Intra-Operative Dexamethasone After Scheduled Cesarean Delivery: A Retrospective StudyMiftah Furqon AuliaNo ratings yet
- Pain Management Guidelines 15-11-2012Document62 pagesPain Management Guidelines 15-11-2012Galuh NurfadillahNo ratings yet
- Continuous Peripheral Nerve Block For PoDocument5 pagesContinuous Peripheral Nerve Block For PoBinNo ratings yet
- Curriculum Vitae of Paul Kempen, MDDocument16 pagesCurriculum Vitae of Paul Kempen, MDAssociation of American Physicians and Surgeons100% (1)
- Suturing WorkshopDocument87 pagesSuturing WorkshopVictor OpreaNo ratings yet
- Parenterals Unit IIIDocument117 pagesParenterals Unit IIIKrishna PrasadNo ratings yet
- Anesthesia Hub - QuestionsDocument15 pagesAnesthesia Hub - QuestionsMedicine Agency100% (3)
- Sample Nursing Care PlansDocument18 pagesSample Nursing Care Planslaritza100% (3)
- CTS 1 - Back PainDocument17 pagesCTS 1 - Back PainVikNo ratings yet
- Komplikasi Pain ManagementDocument60 pagesKomplikasi Pain ManagementSigit SutantoNo ratings yet
- On The Concept of Third Occipital HeadacDocument7 pagesOn The Concept of Third Occipital HeadacVladislav KotovNo ratings yet
- 2chain of DiseaseDocument43 pages2chain of Diseaseyuuki konno100% (1)
- Management of Failed Block - Harsh.Document48 pagesManagement of Failed Block - Harsh.Faeiz KhanNo ratings yet
- Introduction To AnaesthesiaDocument24 pagesIntroduction To AnaesthesiaDeobrat DwivediNo ratings yet
- Anaes FCPS 2 Mar 2023 Recalled Paper (Edited With Keys) LatestDocument29 pagesAnaes FCPS 2 Mar 2023 Recalled Paper (Edited With Keys) LatestDr IqraNo ratings yet
- Tinjauan Pustaka Persalinan NormalDocument31 pagesTinjauan Pustaka Persalinan NormalNurul Fathia Shafira AmiantiNo ratings yet
- Post Anaesthesia Shivering - N PadayacheeDocument19 pagesPost Anaesthesia Shivering - N Padayacheexxxvrgnt100% (2)
- Types of Anesthesia and Your AnesthesiologistDocument3 pagesTypes of Anesthesia and Your AnesthesiologistYamSomandarNo ratings yet
- Sub Arachnoid BlockDocument32 pagesSub Arachnoid Blockhendra_darmawan_4No ratings yet
- 4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Document13 pages4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Rupa Ghosh100% (1)
- Obstetric Neurological Injuries: ReviewDocument8 pagesObstetric Neurological Injuries: Reviewaish25No ratings yet
- Regional Anesthesia: LT Col Syed Majid Dept. of AnesthesiologyDocument49 pagesRegional Anesthesia: LT Col Syed Majid Dept. of AnesthesiologykhanmoinNo ratings yet
- Comparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringDocument6 pagesComparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringabdulNo ratings yet
- Dr. Senthil Priya Heart Disease in Pregnancy FINALDocument68 pagesDr. Senthil Priya Heart Disease in Pregnancy FINALKai ParkerNo ratings yet
- UCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Document5 pagesUCSF Antithrombotics Neuraxia Lnterventions Guideline Version4Olguita Huaccha PastorNo ratings yet
- BRS General SurgeryDocument2,923 pagesBRS General SurgeryIsnah BiaresNo ratings yet
- Anaesthesia For Pancreatic SurgeryDocument11 pagesAnaesthesia For Pancreatic SurgeryDianita P Ñáñez VaronaNo ratings yet