Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Case-Based Pace, ICDs, and CRT Volume 1Document234 pagesCase-Based Pace, ICDs, and CRT Volume 1oxequlalisNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson Plan On EcgDocument3 pagesLesson Plan On Ecganimesh panda100% (1)
- Lab Report 2 AutosavedDocument18 pagesLab Report 2 Autosavedapi-249482502100% (2)
- Brugada SyndromeDocument3 pagesBrugada SyndromeBogdan ClujNo ratings yet
- Management of Cardiac ArrestDocument10 pagesManagement of Cardiac ArrestAhmed VelićNo ratings yet
- CT 2Document16 pagesCT 2TGB LEGENDNo ratings yet
- Management of Coronary Artery SpasmDocument14 pagesManagement of Coronary Artery SpasmdcicareNo ratings yet
- Acute Coronary SyndromeDocument32 pagesAcute Coronary SyndromeCzarina jane MendozaNo ratings yet
- ABC of Pediatric ECGDocument5 pagesABC of Pediatric ECGThalita SophiaNo ratings yet
- MEANS ECG Physicians ' Manual For Welch Allyn CP Series ElectrocardiographsDocument63 pagesMEANS ECG Physicians ' Manual For Welch Allyn CP Series Electrocardiographscygnus8929No ratings yet
- PIIS109491942200007XDocument22 pagesPIIS109491942200007X60'041 Kanin TianbudNo ratings yet
- Latihan Ekg KD A III 2016Document15 pagesLatihan Ekg KD A III 2016Syamsul PutraNo ratings yet
- CardiologyDocument70 pagesCardiologyDharshini MohanNo ratings yet
- EKG StripsDocument10 pagesEKG StripsSaidel ElizondoNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- Labetacure - Pregnancy HTN-1Document9 pagesLabetacure - Pregnancy HTN-1Omar Nassir MoftahNo ratings yet
- 31 - DINAMAP SuperSTAT NIPB - White Paper - JB26543XX - Dec8Document4 pages31 - DINAMAP SuperSTAT NIPB - White Paper - JB26543XX - Dec8Jorio LemosNo ratings yet
- Lab Report 1Document14 pagesLab Report 1api-273323485No ratings yet
- Omron m4 I Users Manual 332434Document8 pagesOmron m4 I Users Manual 332434erkkiankaraNo ratings yet
- Fernalia, Devi Listiana, Harti Monica STIKES Tri Mandiri Sakti, BengkuluDocument10 pagesFernalia, Devi Listiana, Harti Monica STIKES Tri Mandiri Sakti, BengkuluSyafi udinNo ratings yet
- Atypical Bypass Tracts 2019Document21 pagesAtypical Bypass Tracts 2019Võ Từ NhấtNo ratings yet
- 5 Cardiac Cycle & Heart SoundsDocument32 pages5 Cardiac Cycle & Heart SoundsDisha SuvarnaNo ratings yet
- PPG-BP DatasetDocument18 pagesPPG-BP DatasetmohNo ratings yet
- S8 Specifications V2.0 20221208Document8 pagesS8 Specifications V2.0 20221208Declan WangNo ratings yet
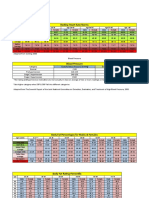
- Resting Heart Rate NormsDocument3 pagesResting Heart Rate Normstre100% (1)
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Arrhythmia: DR Maham SaleemDocument17 pagesArrhythmia: DR Maham SaleemMaham SaleemNo ratings yet
- Asuhan Keperawatan Kritis Dengan MCIDocument28 pagesAsuhan Keperawatan Kritis Dengan MCIsusi jNo ratings yet
- Materi Dasar EkgDocument52 pagesMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- Cardiovascular Pharmacology PDFDocument85 pagesCardiovascular Pharmacology PDFAhmed Shihab AhmedNo ratings yet