Download as docx, pdf, or txt
You might also like
- Occupational Profile FinalDocument20 pagesOccupational Profile Finalapi-238703581100% (1)
- Occt651 - Occupational Profile Paper - FinalDocument20 pagesOcct651 - Occupational Profile Paper - Finalapi-293182319No ratings yet
- Stroke Occupational Profile Paper - 651Document21 pagesStroke Occupational Profile Paper - 651api-290919325100% (1)
- Occupational Profile PaperDocument20 pagesOccupational Profile Paperapi-292814113No ratings yet
- Occupational Therapy Discharge SummaryDocument3 pagesOccupational Therapy Discharge Summaryapi-3806812240% (1)
- SOP 003 Floor Scrubbing - MachineDocument2 pagesSOP 003 Floor Scrubbing - MachineMade Gilee100% (1)
- SantaCountyWTv0 7 2-b1Document35 pagesSantaCountyWTv0 7 2-b1AlfredoNo ratings yet
- Revised National Plumbing Code: of The PhilippinesDocument49 pagesRevised National Plumbing Code: of The PhilippinesAlskduiNo ratings yet
- Occupational Therapy Discontinuation ReportDocument2 pagesOccupational Therapy Discontinuation Reportapi-273311864No ratings yet
- Community Client Discharge SummaryDocument3 pagesCommunity Client Discharge Summaryapi-271980676No ratings yet
- AOTA Occupational Profile TemplateDocument2 pagesAOTA Occupational Profile TemplateVIJAYA DHARSHINI M Bachelor in Occupational Therapy (BOT)No ratings yet
- Case Study Paper FinalDocument19 pagesCase Study Paper Finalapi-240832658No ratings yet
- About The NBCOT OTR and Cota Exams: Exam BasicsDocument2 pagesAbout The NBCOT OTR and Cota Exams: Exam BasicsJennifer gomezNo ratings yet
- 630 Occupational Profile and Intervention PlanDocument22 pages630 Occupational Profile and Intervention Planapi-282538590100% (1)
- AOTA Occupational Profile Template PDFDocument2 pagesAOTA Occupational Profile Template PDFShamiso ChidongoNo ratings yet
- Occupational Therapy Survival GuideDocument12 pagesOccupational Therapy Survival Guideapi-256686248No ratings yet
- Model of Human OccupationDocument5 pagesModel of Human OccupationPatrick IlaoNo ratings yet
- Soap NoteDocument2 pagesSoap Noteapi-285542134No ratings yet
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Occupational Profile and Intervention Plan FinalDocument21 pagesOccupational Profile and Intervention Plan Finalapi-263352281No ratings yet
- Occupational Therapy Evaluation Report and Initial Intervention PlanDocument12 pagesOccupational Therapy Evaluation Report and Initial Intervention Planapi-488383880100% (1)
- Eval Soap Note 2Document9 pagesEval Soap Note 2api-435763096No ratings yet
- 630 Occupational Profile AssignmentDocument13 pages630 Occupational Profile Assignmentapi-201999002No ratings yet
- Dickson Occupational ProfileDocument18 pagesDickson Occupational Profileapi-255001706No ratings yet
- Occupational Therapy Discharge SummaryDocument4 pagesOccupational Therapy Discharge Summaryapi-518285126No ratings yet
- 630 Submitted Occupational Profile and AnalysisDocument21 pages630 Submitted Occupational Profile and Analysisapi-310815315No ratings yet
- Occupational Therapy Practice FrameworkDocument31 pagesOccupational Therapy Practice FrameworkLian Michael0% (1)
- 4th Sem 651 Occupational ProfileDocument19 pages4th Sem 651 Occupational Profileapi-291545292100% (1)
- Occupational Profile and Intervention Plan FinalDocument21 pagesOccupational Profile and Intervention Plan Finalapi-293223028No ratings yet
- Pediatric SpaDocument11 pagesPediatric Spaapi-420919156100% (2)
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Document54 pages2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18No ratings yet
- Occupational Profile and Intervention PlanDocument13 pagesOccupational Profile and Intervention Planapi-251993533No ratings yet
- Kristen Kincaid Occupational Analysis & Intervention PlanDocument23 pagesKristen Kincaid Occupational Analysis & Intervention Planapi-282525755100% (1)
- Evaluation ReportDocument3 pagesEvaluation Reportapi-547360536No ratings yet
- Study ResourcesDocument3 pagesStudy Resourcesapi-405162391No ratings yet
- Occupational ProfileDocument21 pagesOccupational Profileapi-293223028100% (1)
- Occupations Profile & Intervention PlanDocument20 pagesOccupations Profile & Intervention Planapi-282223043No ratings yet
- Running Head: Occupational Profile and Intervention Plan 1Document19 pagesRunning Head: Occupational Profile and Intervention Plan 1api-292735638No ratings yet
- Dick, Elisa - Occupational ProfileDocument10 pagesDick, Elisa - Occupational Profileapi-234536968No ratings yet
- 15 Ot Sop Aota Exam PrepDocument46 pages15 Ot Sop Aota Exam PrepJarred AdamsNo ratings yet
- A Model of Human Occupation ApproachDocument55 pagesA Model of Human Occupation Approachllloo100% (8)
- Ethics Occupational TherapyDocument7 pagesEthics Occupational TherapyGeyanne GeyrosagaNo ratings yet
- OT and Eating DysfunctionDocument1 pageOT and Eating DysfunctionMCris EsSemNo ratings yet
- Occt630 Occupational Profile InterventionDocument19 pagesOcct630 Occupational Profile Interventionapi-290880850No ratings yet
- Occupational Analysis Intervention PlanDocument19 pagesOccupational Analysis Intervention Planapi-293223028No ratings yet
- Occupational Therapy ProcessDocument3 pagesOccupational Therapy Processapi-339841373100% (1)
- Occupational Profile & Intervention PlanDocument20 pagesOccupational Profile & Intervention Planapi-262531856No ratings yet
- Frame of ReferenceDocument10 pagesFrame of ReferenceGustavo CabanasNo ratings yet
- Artifact 5 Soap NoteDocument3 pagesArtifact 5 Soap Noteapi-517998988No ratings yet
- Occupational Profile and Intervention PlanDocument18 pagesOccupational Profile and Intervention Planapi-282525755No ratings yet
- OT Practice FrameworkDocument12 pagesOT Practice Frameworkenrico_aguila100% (2)
- Occupational Therapy: Skills For LivingDocument14 pagesOccupational Therapy: Skills For Livingkalik67% (3)
- Position Paper OT For People With LDDocument10 pagesPosition Paper OT For People With LDLytiana WilliamsNo ratings yet
- Stroke Rehab Fact SheetDocument2 pagesStroke Rehab Fact SheetHendra PrayogaNo ratings yet
- Soap 11Document4 pagesSoap 11api-436429414No ratings yet
- Study TipsDocument2 pagesStudy Tipsapi-405162391No ratings yet
- Occupational Therapy Catalog - 2009Document12 pagesOccupational Therapy Catalog - 2009rrockel100% (1)
- Fieldwork Case Study Treatment Plan AssignmentDocument11 pagesFieldwork Case Study Treatment Plan Assignmentapi-398892840No ratings yet
- Occupational Profile WeeblyDocument34 pagesOccupational Profile Weeblyapi-293253519100% (1)
- Student Treatment Session Soap 8Document9 pagesStudent Treatment Session Soap 8api-340625860100% (1)
- Instrumental Activities Daily Living: Try ThisDocument11 pagesInstrumental Activities Daily Living: Try ThisbalryoNo ratings yet
- Senior Occupational Therapist: Passbooks Study GuideFrom EverandSenior Occupational Therapist: Passbooks Study GuideNo ratings yet
- Osce Evaluation RevisedDocument5 pagesOsce Evaluation Revisedapi-582889983No ratings yet
- Reflective Theories Writing AssignmentDocument7 pagesReflective Theories Writing Assignmentapi-582889983No ratings yet
- Sensory Room Presentation Due 12Document9 pagesSensory Room Presentation Due 12api-582889983No ratings yet
- Discharge SummaryDocument3 pagesDischarge Summaryapi-582889983No ratings yet
- Intervention Plan For Community Client With ReflectionDocument2 pagesIntervention Plan For Community Client With Reflectionapi-582889983No ratings yet
- Grant ProposalDocument18 pagesGrant Proposalapi-582889983No ratings yet
- 1restaurant-Model GFDocument1 page1restaurant-Model GFchandhramohannNo ratings yet
- Hotpoint-Ariston LL 42Document13 pagesHotpoint-Ariston LL 42Octavian CordosNo ratings yet
- Test 5 A+bDocument4 pagesTest 5 A+bBoBa PRONo ratings yet
- The Dominion of Sin Book Two of The Origins Daughter Series Alexandra ST Pierre Full ChapterDocument60 pagesThe Dominion of Sin Book Two of The Origins Daughter Series Alexandra ST Pierre Full Chapterivy.crawford638100% (6)
- Manual Masina de Spalat Vase Beko 15 SeturiDocument49 pagesManual Masina de Spalat Vase Beko 15 SeturiPerfectreviewNo ratings yet
- 3 BedDocument36 pages3 Bedemmanuel SiawNo ratings yet
- Prepositions and The Haunted HouseDocument6 pagesPrepositions and The Haunted HouseHanna MykhalskaNo ratings yet
- Lakme MakeupDocument114 pagesLakme MakeupContract100% (1)
- 83TR Tork+Hand+Towel+Roll+Dispenser,+LeverDocument2 pages83TR Tork+Hand+Towel+Roll+Dispenser,+LevercasildogonzalesNo ratings yet
- Free Time Speaking Cards Fun Activities Games Icebreakers Oneonone Activiti - 76064Document1 pageFree Time Speaking Cards Fun Activities Games Icebreakers Oneonone Activiti - 76064ReveszNikiNo ratings yet
- Bettys House Fun Activities Games - 481Document1 pageBettys House Fun Activities Games - 481Lorena D CaviaNo ratings yet
- KG 1Document11 pagesKG 1Oluwafisayomi JoshuaNo ratings yet
- Soal PAT Kelas VII 2 - Bahasa InggrisDocument7 pagesSoal PAT Kelas VII 2 - Bahasa InggrisNurur RahayuNo ratings yet
- Radisson Blu HotelDocument2 pagesRadisson Blu Hotelrafaqathussain8710No ratings yet
- GROHE F-Digital PDFDocument24 pagesGROHE F-Digital PDFDanny LamNo ratings yet
- Resources For Fire Protection ProfessionalsDocument1 pageResources For Fire Protection Professionalshitokiri_knives0% (1)
- Confirmation NiceDocument2 pagesConfirmation NiceNiyas Bin Abdul AzeezNo ratings yet
- Instalasi Air Kotor & BekasDocument1 pageInstalasi Air Kotor & BekasRatih WulandariNo ratings yet
- Independent Practice ReflexiveDocument2 pagesIndependent Practice ReflexiveJoaquinNo ratings yet
- Housekeeping Assessment TestDocument4 pagesHousekeeping Assessment TestKunal Prajapati100% (2)
- GROHE Bathroom Brochure PDFDocument296 pagesGROHE Bathroom Brochure PDFdmakaricNo ratings yet
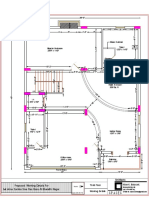
- Anne Samba Siva Rao Garu Final Plans Working-ModelDocument1 pageAnne Samba Siva Rao Garu Final Plans Working-ModelAneo AbhiNo ratings yet
- Hotel Room 1Document9 pagesHotel Room 1Yvonne Janet Cosico-Dela FuenteNo ratings yet
- BCBC2018 3.8 AccessibilityDocument19 pagesBCBC2018 3.8 Accessibilitylin xuNo ratings yet
- 2023.10.10 Plan Review CommentsDocument18 pages2023.10.10 Plan Review CommentsXuân LaNo ratings yet
- ConfirmationDocument1 pageConfirmationSibonginkosi NxumaloNo ratings yet
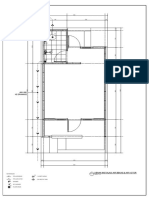
- Residential Building: First Floor PlansDocument1 pageResidential Building: First Floor PlansmomenNo ratings yet