Download as docx, pdf, or txt
You might also like
- Chapter 12: Heart: Functions of The HeartDocument12 pagesChapter 12: Heart: Functions of The Heartchristian anchetaNo ratings yet
- Cardiovascular System Heart ReviewerDocument8 pagesCardiovascular System Heart ReviewerImmanuel Cris PalasigueNo ratings yet
- First Aid Emergencies: Call/DialDocument5 pagesFirst Aid Emergencies: Call/DialKhalilahmad Khatri100% (1)
- Blodd Cell Poster PDFDocument2 pagesBlodd Cell Poster PDFGustavo Adolfo Piñero BorgesNo ratings yet
- Third Spacing - Where Has All The Fluid GoneDocument14 pagesThird Spacing - Where Has All The Fluid Gonedbryant0101100% (15)
- Anatomy of The HeartDocument3 pagesAnatomy of The HeartCanan YilmazNo ratings yet
- MEDIASTINUMDocument3 pagesMEDIASTINUMlilac.poppy.48No ratings yet
- Cardiovascular SystemDocument9 pagesCardiovascular SystemCrazy StrangerNo ratings yet
- اشرف بيركارديوم اند هارتDocument35 pagesاشرف بيركارديوم اند هارتبيلسان 'نNo ratings yet
- Anatomia InimiiDocument5 pagesAnatomia InimiiMariaa MariutssaNo ratings yet
- HeartDocument7 pagesHeartlilac.poppy.48No ratings yet
- Hap - Circulatory System HeartDocument13 pagesHap - Circulatory System HeartKyle LumingkitNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemHannah Grace CorveraNo ratings yet
- Four Chambers of The HeartDocument7 pagesFour Chambers of The HeartJohn TecsonNo ratings yet
- 10th Week Practical LessonsDocument11 pages10th Week Practical LessonstheodorastanerNo ratings yet
- Four Chambers of The HeartDocument7 pagesFour Chambers of The HeartJohn TecsonNo ratings yet
- Whitaker 2010Document3 pagesWhitaker 2010Gabriel Jose CarvajalNo ratings yet
- Cardiovascular SystemDocument57 pagesCardiovascular SystemSarah Shane Cortes CortesNo ratings yet
- ANPH Wk12 - Cardiovascular SystemDocument17 pagesANPH Wk12 - Cardiovascular SystemSin I GangNo ratings yet
- Heart Finals ReviewerDocument7 pagesHeart Finals ReviewershannenmaehfajanilanNo ratings yet
- Anatomi Kardio PDFDocument49 pagesAnatomi Kardio PDFDestrini Anjani LandaNo ratings yet
- Anatomy Heart PericardiumDocument34 pagesAnatomy Heart PericardiumMICHAEL KEPSEUNo ratings yet
- Surfacwe Anatomy of Cvs and Arterial Puls AreasDocument6 pagesSurfacwe Anatomy of Cvs and Arterial Puls AreasHisham ChomanyNo ratings yet
- Anatomy & Histology of PericardiumDocument2 pagesAnatomy & Histology of PericardiumDila Larasati100% (1)
- CARDIODocument17 pagesCARDIORayana Ubas100% (1)
- Anaphy HeartDocument6 pagesAnaphy HeartAngellene GraceNo ratings yet
- A12. MediastinumDocument29 pagesA12. MediastinumUmerNo ratings yet
- Cardiovascular System: The HeartDocument28 pagesCardiovascular System: The HeartTania Pal ChoudhuryNo ratings yet
- HEARTDocument11 pagesHEARTcatalinaNo ratings yet
- Cardiovascular System WordDocument18 pagesCardiovascular System WordLapitan Jared Anne S.No ratings yet
- CARDIO VASCULAR SYSTEM TransesDocument4 pagesCARDIO VASCULAR SYSTEM TransesBianca Paulyn CastilloNo ratings yet
- CIRCULATORY SYSTEM (Heart)Document4 pagesCIRCULATORY SYSTEM (Heart)Andrei NicoleNo ratings yet
- AP Heart ReviewerDocument7 pagesAP Heart Revieweryes noNo ratings yet
- Kuliah 1 OVERVIEW Titipan Dari (DR Pipiet)Document465 pagesKuliah 1 OVERVIEW Titipan Dari (DR Pipiet)Gangsar DamaiNo ratings yet
- Heart and Blood Vessels, BloodDocument13 pagesHeart and Blood Vessels, BloodDaniel DanielNo ratings yet
- Heart and Its External Features For Paramedical StudentsDocument26 pagesHeart and Its External Features For Paramedical Studentslakshmiraman1770No ratings yet
- 3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumDocument3 pages3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumAebee Alcaraz100% (1)
- CH - 10 - THE CARDIOVASCULAR SYSTEMDocument122 pagesCH - 10 - THE CARDIOVASCULAR SYSTEMCheska DillupacNo ratings yet
- Cardiovascular System - The HeartDocument37 pagesCardiovascular System - The HeartCecil AlbaNo ratings yet
- CARDIOLOGYDocument15 pagesCARDIOLOGYPatty RomeroNo ratings yet
- 9 PericardiumDocument19 pages9 PericardiumAuza Moses Ibrahim100% (2)
- The Cardiovascular SystemDocument17 pagesThe Cardiovascular SystemChris Deinielle Marcoleta Sumaoang100% (1)
- Cardiovascular SystemDocument103 pagesCardiovascular System2022105340No ratings yet
- Anaphy Lab CardioDocument3 pagesAnaphy Lab CardioRyan Dave UmayamNo ratings yet
- CH 21: Cardiovascular System - The HeartDocument21 pagesCH 21: Cardiovascular System - The HeartMadhuri DandamudiNo ratings yet
- Cardiovascular - SummaryDocument18 pagesCardiovascular - Summarys.tinaja.marieantonetteNo ratings yet
- CHAP11Document12 pagesCHAP11Crystal ARIETANo ratings yet
- Heart External AnatomyDocument6 pagesHeart External AnatomyKrissia BaasisNo ratings yet
- BY Ifenna Nnachi Salvator REG NO: 2019070000636Document35 pagesBY Ifenna Nnachi Salvator REG NO: 2019070000636nnachi ifennaNo ratings yet
- MC1 Lec12 13 CardiovascularDocument119 pagesMC1 Lec12 13 CardiovascularVERGEL, Sophia Luis V.No ratings yet
- AnatomyDocument8 pagesAnatomyOM BAWNENo ratings yet
- 1 Pericardium - MbbsDocument34 pages1 Pericardium - MbbsmwadramannNo ratings yet
- CARDIOVASDocument3 pagesCARDIOVASFrama Intan MiguelNo ratings yet
- HeartDocument11 pagesHeartAdamNo ratings yet
- Corazón AnatomicoDocument19 pagesCorazón Anatomicojoselyngarciaga2005No ratings yet
- Mammalian Heart PDFDocument5 pagesMammalian Heart PDFKhaled TurkNo ratings yet
- 1-Heart 2015Document27 pages1-Heart 2015smeersalalNo ratings yet
- Anatomy of The Heart & Its ValvesDocument9 pagesAnatomy of The Heart & Its ValvesJustine CastilloNo ratings yet
- Heart and Neck VesselsDocument31 pagesHeart and Neck Vesselsshellacayetano2No ratings yet
- Cardiology. Section 1. Anatomy of HeartDocument13 pagesCardiology. Section 1. Anatomy of HeartJennifer SteffiNo ratings yet
- CVS and Blood Anatomy - 2Document55 pagesCVS and Blood Anatomy - 2Tharushi PereraNo ratings yet
- Cardiovascular System 1Document66 pagesCardiovascular System 1Mary joy DavidNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- DAN AG Monte Aribal Family Final PaperDocument81 pagesDAN AG Monte Aribal Family Final Paperallenh016No ratings yet
- Batch 2025 (Spirare) : Cebu Institute of Medicine Class ListDocument1 pageBatch 2025 (Spirare) : Cebu Institute of Medicine Class Listallenh016No ratings yet
- Hypothyroidism: Radioiodine Uptake and Thyroid ScanningDocument6 pagesHypothyroidism: Radioiodine Uptake and Thyroid Scanningallenh016No ratings yet
- 2021 Third Exam CoverageDocument3 pages2021 Third Exam Coverageallenh016No ratings yet
- Retinopathy of Prematurity & Retinoblastoma: Salinas & EstellaDocument23 pagesRetinopathy of Prematurity & Retinoblastoma: Salinas & Estellaallenh016No ratings yet
- DOTA 2 Rules Regulations Intramurals 2019Document3 pagesDOTA 2 Rules Regulations Intramurals 2019allenh016No ratings yet
- Strabismus and Amblyopia: Allen Habajab Samantha ReyesDocument23 pagesStrabismus and Amblyopia: Allen Habajab Samantha Reyesallenh016No ratings yet
- Ocular Pharmacology: Salinas EstellaDocument26 pagesOcular Pharmacology: Salinas Estellaallenh016No ratings yet
- MICROB3 - Chapter3 - Cell Structure and FunctionDocument40 pagesMICROB3 - Chapter3 - Cell Structure and FunctionAdriana Corrêa0% (1)
- L3, 16-18 Gross Anatomy of Pelvis and PerineumDocument37 pagesL3, 16-18 Gross Anatomy of Pelvis and PerineumБеатриса ШипNo ratings yet
- 404 - Lipid - ZC# 25-30Document47 pages404 - Lipid - ZC# 25-30fatehatun noorNo ratings yet
- Bahan SupervisiDocument21 pagesBahan SupervisiMeta BachtiarNo ratings yet
- Sepsis and Septic ShockDocument28 pagesSepsis and Septic ShockHayk MinasyanNo ratings yet
- Amino Acids Metabol Synth of UreaDocument32 pagesAmino Acids Metabol Synth of UreaAnastasiafynn100% (1)
- Cap. 06 - Avian Anatomy and PhysiologyDocument65 pagesCap. 06 - Avian Anatomy and PhysiologyNailson JúniorNo ratings yet
- Pain PathwayDocument46 pagesPain PathwayAnil Kumar ReddyNo ratings yet
- Postnatal AssessmentDocument9 pagesPostnatal Assessmentsaleha sultana100% (1)
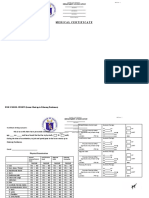
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Peachy FreezyNo ratings yet
- Lab 3 - Dissection Guide - EarthwormDocument15 pagesLab 3 - Dissection Guide - Earthwormbszool006No ratings yet
- Cell Structure and Functions: Class 8 NCERT Biology Chapter 4Document29 pagesCell Structure and Functions: Class 8 NCERT Biology Chapter 4Chitranshee RastogiNo ratings yet
- Chest PainDocument13 pagesChest Paing3murtulu100% (1)
- SMARTLYTE Quick Setup GuideDocument2 pagesSMARTLYTE Quick Setup GuideSandy KompengNo ratings yet
- Olmetec-Ci e PDFDocument3 pagesOlmetec-Ci e PDFAlyssa Dannah RodriguezNo ratings yet
- Biological Classification Class 11 Notes Biology CDocument14 pagesBiological Classification Class 11 Notes Biology Cdharun0704No ratings yet
- Blood Group Incompatibility RH DiseaseDocument35 pagesBlood Group Incompatibility RH DiseaseRay SadisNo ratings yet
- Chapter 1 The World Through Our SensesDocument18 pagesChapter 1 The World Through Our SensesNurul Ain RazaliNo ratings yet
- Anatomy - Board Ii: Abdomen - Oral PartDocument25 pagesAnatomy - Board Ii: Abdomen - Oral Partbadiuzzaman2010No ratings yet
- Such Thing As An Anion Gap Metabolic Alkalosis. There Is Also No Such ThingDocument3 pagesSuch Thing As An Anion Gap Metabolic Alkalosis. There Is Also No Such ThingMwanja MosesNo ratings yet
- Fatty Acid BiosynthesisDocument7 pagesFatty Acid BiosynthesisJeremiah Eyo AmanamNo ratings yet
- Rules and Regulations For BPTDocument54 pagesRules and Regulations For BPTSherin KNo ratings yet
- An Efficient Chronic Unpredictable Stress Protocol To Induce Stress-Related Responses in C57BL-6 MiceDocument11 pagesAn Efficient Chronic Unpredictable Stress Protocol To Induce Stress-Related Responses in C57BL-6 MiceVampyrgirlNo ratings yet
- Respiratory System ReviewerDocument7 pagesRespiratory System ReviewerVictoria Ellex TiomicoNo ratings yet
- JUJ Pahang SPM 2014 Biology K3 Set 2 SkemaDocument14 pagesJUJ Pahang SPM 2014 Biology K3 Set 2 SkemaCikgu FaizalNo ratings yet
- Test A AnsweredDocument15 pagesTest A AnsweredSarah FathimaNo ratings yet