Download as pdf or txt
You might also like
- SLRC-Handouts CHN OutlineDocument18 pagesSLRC-Handouts CHN OutlineJingle Domingo CanonizadoNo ratings yet
- 600R003137 Cured WEB PDFDocument545 pages600R003137 Cured WEB PDFEdie M Murgia100% (9)
- Palliative Care HandbookDocument81 pagesPalliative Care Handbookgeoaisla50% (2)
- SOP For Specialist in Family MedicineDocument13 pagesSOP For Specialist in Family Medicinesaba_zafar0% (1)
- Pafp Foundation CoursesDocument3 pagesPafp Foundation CoursesPasDoc Soriano100% (1)
- Palliative Care 11918Document69 pagesPalliative Care 11918meldelsNo ratings yet
- NURSING PROCEDURES FOR CHN Converted 1Document25 pagesNURSING PROCEDURES FOR CHN Converted 1Genki Fay B. Lequigan100% (1)
- CHCPA301B Deliver Care Services Using A Palliative ApproachDocument73 pagesCHCPA301B Deliver Care Services Using A Palliative ApproachBhakta Chand ThakuriNo ratings yet
- Integrative Support and Interprofessional Collaboration in Palliative Care ServicesDocument56 pagesIntegrative Support and Interprofessional Collaboration in Palliative Care Servicesrose fania100% (1)
- Draft Palliative Care Needs Assessment - A Guide For Health Care ProfessionalsDocument10 pagesDraft Palliative Care Needs Assessment - A Guide For Health Care ProfessionalsSenja TsamrotulNo ratings yet
- JOB RESPONSIBILITIES OF CHOs AT HWCsDocument4 pagesJOB RESPONSIBILITIES OF CHOs AT HWCsMallappa OdomaneNo ratings yet
- Mental Health MDRM 503 John Rainer TalabisDocument13 pagesMental Health MDRM 503 John Rainer TalabisEy-ey ChioNo ratings yet
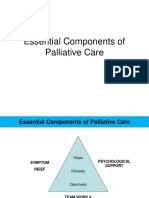
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano60% (5)
- Palliative Care For Adults.Document28 pagesPalliative Care For Adults.Madalina TalpauNo ratings yet
- GERIADocument48 pagesGERIAGleza MirallesNo ratings yet
- Healthcare ProcessDocument40 pagesHealthcare ProcessSJO1 G6- Escaro,Shaira JoyNo ratings yet
- End of Life CareDocument18 pagesEnd of Life CareArifBijaksanaBijaksiniNo ratings yet
- Telehealth Best Practice Guide FINAL April30Document16 pagesTelehealth Best Practice Guide FINAL April30jklNo ratings yet
- Palliative CareDocument6 pagesPalliative CareVILLEJO JHOVIALENNo ratings yet
- Nursing Theory and Practice - 6 Lecture 4Document46 pagesNursing Theory and Practice - 6 Lecture 4nethmi kaushalyaNo ratings yet
- Emergency Nursing Notes 1Document12 pagesEmergency Nursing Notes 1pauchanmnl100% (2)
- NS1p1 Theory and Clinical Workbook FALL 13 07-12-13 - CLeeDocument98 pagesNS1p1 Theory and Clinical Workbook FALL 13 07-12-13 - CLeefranciaeleazarNo ratings yet
- The Nature of CHN Practice Requires That Current Knowledge Derived From TheDocument17 pagesThe Nature of CHN Practice Requires That Current Knowledge Derived From TheAlexis TrinidadNo ratings yet
- Aged Care (Silver Book) - Part ADocument25 pagesAged Care (Silver Book) - Part AXin gNo ratings yet
- CHN NotesDocument7 pagesCHN NotesRoy SalvadorNo ratings yet
- DM Critical Care Medicine PDFDocument23 pagesDM Critical Care Medicine PDFArun Sahaya RajaNo ratings yet
- Neonatal GoalsDocument5 pagesNeonatal GoalsJehanie LukmanNo ratings yet
- EBP Smoking CessationDocument3 pagesEBP Smoking CessationAli KayNo ratings yet
- Section5 111-130Document20 pagesSection5 111-130Nurliana Lina AchmadNo ratings yet
- Palliative Care Needs Assessment GuidanceDocument13 pagesPalliative Care Needs Assessment Guidancenovia100% (1)
- Konsep Palliative Care Pada AnakDocument48 pagesKonsep Palliative Care Pada AnakDayu Dani100% (1)
- كويز ميديكال 5Document14 pagesكويز ميديكال 5Nansy DaasNo ratings yet
- CU02A WEEK02-NursingProcessinPMHNPractice28VAL2928129MODULEDocument8 pagesCU02A WEEK02-NursingProcessinPMHNPractice28VAL2928129MODULEduca.danrainer02No ratings yet
- "DNR'' Do Not Resuscitate Status: Division: Department: SectionDocument8 pages"DNR'' Do Not Resuscitate Status: Division: Department: SectionKathleen Sharmaine S. CatubigNo ratings yet
- Palliative Care Guidelines-20 November2013Document69 pagesPalliative Care Guidelines-20 November2013Olga ŢiuNo ratings yet
- Nurs 3021 - Midterm Evaluation - AkDocument9 pagesNurs 3021 - Midterm Evaluation - Akapi-240864098No ratings yet
- GUIDLINE 15 - CPG - Diagnosis - DepressionDocument49 pagesGUIDLINE 15 - CPG - Diagnosis - DepressioncaturNo ratings yet
- Long Term Care PresentationDocument19 pagesLong Term Care PresentationKkkkkggffNo ratings yet
- Pumarada BSN4A HCN00 PrelimAct1Document4 pagesPumarada BSN4A HCN00 PrelimAct1Lee BuelaNo ratings yet
- Palliative and Rehablitative CareDocument25 pagesPalliative and Rehablitative CareMulat AlemuNo ratings yet
- Bipolar QRGDocument24 pagesBipolar QRGRe LzNo ratings yet
- Chronic Illness Acute Illness: CharacteristicsDocument4 pagesChronic Illness Acute Illness: CharacteristicsFerdinand Sherwin MorataNo ratings yet
- Medical and Allied Health ProfessionDocument21 pagesMedical and Allied Health ProfessionAlthea RejaeNo ratings yet
- Palliative Care Needs Assessment GuidanceDocument13 pagesPalliative Care Needs Assessment GuidanceDedes SahpitraNo ratings yet
- Tugas Rangkuman InhsDocument6 pagesTugas Rangkuman InhsnaztyNo ratings yet
- Competency1. Patient Care: The Neonatal Intensive Care UnitDocument8 pagesCompetency1. Patient Care: The Neonatal Intensive Care UnitChristopher TibuleNo ratings yet
- Principles of Palliative and HospiceDocument15 pagesPrinciples of Palliative and HospiceChucky Vergara100% (1)
- End-of-Life Care For The Newly Licensed Practical Nurse: State of Nebraska Transition GrantDocument8 pagesEnd-of-Life Care For The Newly Licensed Practical Nurse: State of Nebraska Transition GrantGee YorkNo ratings yet
- Paliative Care ObjectiveDocument2 pagesPaliative Care ObjectiveHans AwuahNo ratings yet
- Analysis: Palliative Care From Diagnosis To DeathDocument5 pagesAnalysis: Palliative Care From Diagnosis To DeathFernanda FerreiraNo ratings yet
- Home Care and Family PhysicianDocument25 pagesHome Care and Family PhysicianHanif Alienda WardhaniNo ratings yet
- Mental Health and Mental DisordersDocument24 pagesMental Health and Mental DisordersLouie Kem Anthony BabaranNo ratings yet
- Booklet 7 Guidelines Withholding and Withdrawing Treatment September 2016Document14 pagesBooklet 7 Guidelines Withholding and Withdrawing Treatment September 2016Licence WiseNo ratings yet
- Continuum CareDocument24 pagesContinuum CareJovelyn EspanolaNo ratings yet
- Module 1: Health AssessmentDocument16 pagesModule 1: Health AssessmentAmberNo ratings yet
- Running Head: QSEN 1Document11 pagesRunning Head: QSEN 1Mariam AbedNo ratings yet
- Types of Public Health NursingDocument12 pagesTypes of Public Health NursingRaRe TVNo ratings yet
- Domains of Family MedicineDocument34 pagesDomains of Family MedicineTheop Ayodele100% (1)
- Medical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyFrom EverandMedical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyNo ratings yet
- Clinician's Guide to Chronic Disease Management of Long Term Conditions, TheFrom EverandClinician's Guide to Chronic Disease Management of Long Term Conditions, TheNo ratings yet
- La 1-Apn CatubigDocument23 pagesLa 1-Apn CatubigKathleen Sharmaine S. CatubigNo ratings yet
- La3 Apn CatubigDocument13 pagesLa3 Apn CatubigKathleen Sharmaine S. CatubigNo ratings yet
- La2 Apn CatubigDocument16 pagesLa2 Apn CatubigKathleen Sharmaine S. CatubigNo ratings yet
- Med Emd Ams 06 002Document2 pagesMed Emd Ams 06 002Kathleen Sharmaine S. CatubigNo ratings yet
- Anti CD20 MABsDocument22 pagesAnti CD20 MABsKathleen Sharmaine S. CatubigNo ratings yet
- Infusion Reaction-Initial InfusionDocument2 pagesInfusion Reaction-Initial InfusionKathleen Sharmaine S. CatubigNo ratings yet
- "DNR'' Do Not Resuscitate Status: Division: Department: SectionDocument8 pages"DNR'' Do Not Resuscitate Status: Division: Department: SectionKathleen Sharmaine S. CatubigNo ratings yet
- The Comparative Analysis of Philippines Nursing CuDocument12 pagesThe Comparative Analysis of Philippines Nursing CuKathleen Sharmaine S. CatubigNo ratings yet
- 12 Steps of Aseptic TechniqueDocument7 pages12 Steps of Aseptic TechniqueRobbie MejiaNo ratings yet
- Learning Strategy (Unit 2, Page 20, Reading)Document5 pagesLearning Strategy (Unit 2, Page 20, Reading)Leonela JamiNo ratings yet
- G.R. No. 130547 - Reyes v. Sisters of Mercy HospitalDocument15 pagesG.R. No. 130547 - Reyes v. Sisters of Mercy HospitalTeriz CastroNo ratings yet
- A Ciegas - Josh MalermanDocument6 pagesA Ciegas - Josh MalermanRooyValenciaNo ratings yet
- TB Hiv CoinfectionDocument29 pagesTB Hiv CoinfectionVinobhachowdary DondapatiNo ratings yet
- AMARACHI WORK FinalizedDocument67 pagesAMARACHI WORK FinalizedocNo ratings yet
- HMR TemplateDocument2 pagesHMR TemplatepharmacisticusNo ratings yet
- 10 Personality DisorderDocument3 pages10 Personality DisorderaninNo ratings yet
- Narayana Hrudayalaya - Section C - Group 5Document22 pagesNarayana Hrudayalaya - Section C - Group 5raushanrahulNo ratings yet
- NCM 101Document8 pagesNCM 101Anna LaritaNo ratings yet
- Working of Blood BanksDocument146 pagesWorking of Blood BanksRupali Vaiti100% (1)
- BTL-Aesthetics ED AE-guide-supplement EN100Document8 pagesBTL-Aesthetics ED AE-guide-supplement EN100joaquina.espinoza20No ratings yet
- Health Law Assignment List RegularDocument1 pageHealth Law Assignment List RegularMaaz AlamNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Beractant: Drug Class Therapeutic ActionsDocument4 pagesBeractant: Drug Class Therapeutic ActionsPrincess BartolomeNo ratings yet
- Acute InflammationDocument22 pagesAcute InflammationNicole Mae DavidNo ratings yet
- Sensory Abnormalities in Children With Autism SpecDocument9 pagesSensory Abnormalities in Children With Autism SpecceavilaNo ratings yet
- Jawaban 1Document52 pagesJawaban 1Stefannus Wibisono100% (2)
- Community Mental Health CareDocument43 pagesCommunity Mental Health CareAmnah AzaharNo ratings yet
- Nursing Care Plan - EVALUATION PHASEDocument3 pagesNursing Care Plan - EVALUATION PHASEChezka Orton Swift BolintiamNo ratings yet
- IMA News June 2018Document37 pagesIMA News June 2018adhishbasuNo ratings yet
- An Introduction To Botanical Medicines - History, Science, Uses and DangersDocument208 pagesAn Introduction To Botanical Medicines - History, Science, Uses and DangersSarah HudsonNo ratings yet
- Answers of 2012Document60 pagesAnswers of 2012MohsenNo ratings yet
- Advances in Acute Toxicity Testing: Strengths, Weaknesses and Regulatory AcceptanceDocument8 pagesAdvances in Acute Toxicity Testing: Strengths, Weaknesses and Regulatory AcceptanceMariel GentilesNo ratings yet
- Tiotropium Bromide: Spiriva Handihaler, Spiriva RespimatDocument9 pagesTiotropium Bromide: Spiriva Handihaler, Spiriva RespimatAssem Ashraf KhidhrNo ratings yet
- Statement of Purpose Example 47Document20 pagesStatement of Purpose Example 47akshayNo ratings yet
- Digital Health in India by Nishith Desai AssociatesDocument44 pagesDigital Health in India by Nishith Desai AssociatesManish SharmaNo ratings yet
- What Causes Malaria?Document8 pagesWhat Causes Malaria?Dulce M. LupaseNo ratings yet
- Introduction To General Pathology VPM 152: Web ReviewDocument41 pagesIntroduction To General Pathology VPM 152: Web ReviewRenien Khim BahayaNo ratings yet