Download as pdf or txt
You might also like
- Shares Sale AgreementDocument14 pagesShares Sale AgreementIan Ling100% (1)
- Proposed Workflow For PLS-CADD: Power Line SystemsDocument19 pagesProposed Workflow For PLS-CADD: Power Line SystemsVictor DoyoganNo ratings yet
- Application For Leave of Absence: Billing No.Document1 pageApplication For Leave of Absence: Billing No.fgrfvrnmsNo ratings yet
- Format For Enrollment Cancellation Application For StudentDocument2 pagesFormat For Enrollment Cancellation Application For Studentmanish_iitrNo ratings yet
- 2.0 Alco Leave of AbsenceDocument1 page2.0 Alco Leave of AbsenceRaphael Patrick AlcorizaNo ratings yet
- Application For Subsequent Release of Educational Assistance LoanDocument2 pagesApplication For Subsequent Release of Educational Assistance LoanNikkiQuiranteNo ratings yet
- BatStateU-FO-TAO-01-C - Application Form For GS, PEU, COL, COM Admission - Rev. 02Document2 pagesBatStateU-FO-TAO-01-C - Application Form For GS, PEU, COL, COM Admission - Rev. 02my.donnabelcaleNo ratings yet
- BatStateU FO TAO 01 C Application Form For GS PEU COL COM Admission Rev. 02Document2 pagesBatStateU FO TAO 01 C Application Form For GS PEU COL COM Admission Rev. 02Rudyliza RosalNo ratings yet
- Spes Form 2019Document1 pageSpes Form 2019Benz GarciaNo ratings yet
- Application Form 2022 23Document2 pagesApplication Form 2022 23aftab aliNo ratings yet
- Admission Form Post RN - Fall 2021Document2 pagesAdmission Form Post RN - Fall 2021FurqanNo ratings yet
- CDE Common Application FormDocument2 pagesCDE Common Application FormOppili yappanNo ratings yet
- Application Form 2023-24Document2 pagesApplication Form 2023-24Saeed Ahmed ChacharNo ratings yet
- Fm-Ro-31-02 - Application For Transcript of Records (BS)Document1 pageFm-Ro-31-02 - Application For Transcript of Records (BS)CardoNo ratings yet
- Spes Form 2Document1 pageSpes Form 2Akhira AceNo ratings yet
- Request For Aca Demic Credentials Verification: Physical Therapist Credentials EvaluationDocument2 pagesRequest For Aca Demic Credentials Verification: Physical Therapist Credentials EvaluationMark Danniel SaludNo ratings yet
- Titijaya Scholarship Fund: Part A: Particular of ApplicantDocument6 pagesTitijaya Scholarship Fund: Part A: Particular of ApplicantA. HanaNo ratings yet
- Internship Application FormDocument2 pagesInternship Application FormizuhairNo ratings yet
- OSA-SFAD Form 4B Request Form To Avail 100% SLB (Revised November 2018)Document2 pagesOSA-SFAD Form 4B Request Form To Avail 100% SLB (Revised November 2018)Batchee Awa-aoNo ratings yet
- C:/Users/Neville - Ruwanpathurana/desktop/forms/Course Deferral Request Page 1 of 3Document3 pagesC:/Users/Neville - Ruwanpathurana/desktop/forms/Course Deferral Request Page 1 of 3Dilum EshanNo ratings yet
- Application Form For Pre Matric Scholarship To Minority StudentsDocument6 pagesApplication Form For Pre Matric Scholarship To Minority StudentsNikitaNo ratings yet
- SPES FORM 2 - APPLICATION FORM - Dec2016.finalDocument2 pagesSPES FORM 2 - APPLICATION FORM - Dec2016.finalPeso TitayNo ratings yet
- Request For Official Withdrawal of Course: - QUARTER, AYDocument1 pageRequest For Official Withdrawal of Course: - QUARTER, AYDarryl ArpilledaNo ratings yet
- Certificate of Non-EnrollmentDocument1 pageCertificate of Non-EnrollmentIan PalmaNo ratings yet
- Uoc Refund FormDocument2 pagesUoc Refund Formezwan2198No ratings yet
- SPES FORM 2 - APPLICATION FORM - Dec2016.finalDocument2 pagesSPES FORM 2 - APPLICATION FORM - Dec2016.finalAlisa TurcatoNo ratings yet
- Spes Form 2 - Application Form - Dec2016.finalDocument1 pageSpes Form 2 - Application Form - Dec2016.finalLinette Orense Macato67% (3)
- Application Form: Sggs Engineers' Alumni Association (Seaa)Document4 pagesApplication Form: Sggs Engineers' Alumni Association (Seaa)Priya BahetiNo ratings yet
- Form of SpesDocument2 pagesForm of SpesMark Dave SambranoNo ratings yet
- Application Readmit or Transfer s1 PDFDocument1 pageApplication Readmit or Transfer s1 PDFyankeeNo ratings yet
- Spes Application FormDocument1 pageSpes Application FormShiori Chang100% (2)
- Spes Form 2 Application FormDocument1 pageSpes Form 2 Application FormOMG by NEWJEANSNo ratings yet
- GSR Form No. 03 ACE FORM - ADDING OF SUBJECTDocument1 pageGSR Form No. 03 ACE FORM - ADDING OF SUBJECTJenilyn ManzonNo ratings yet
- Delen Christine Joy Pontines 18-53346 11-01-1999 22 Brgy. Conde Itaas, Batangas City Filipino 09165982354Document3 pagesDelen Christine Joy Pontines 18-53346 11-01-1999 22 Brgy. Conde Itaas, Batangas City Filipino 09165982354Christine Joy DelenNo ratings yet
- Application Form 2020-21Document2 pagesApplication Form 2020-21aqsa soomroNo ratings yet
- Application Form 2020-21Document2 pagesApplication Form 2020-21aqsa soomroNo ratings yet
- Application Form 2020-21Document2 pagesApplication Form 2020-21aqsa soomroNo ratings yet
- 07 - 0221 Faculty - Department Confirmation Sheet On Student Status - For An Extension of Stay in Hong KongDocument1 page07 - 0221 Faculty - Department Confirmation Sheet On Student Status - For An Extension of Stay in Hong KongChun KinNo ratings yet
- Borang Pendaftaran Kursus Pindaan 2019Document3 pagesBorang Pendaftaran Kursus Pindaan 2019Nurul Najwa Binti Othman H20A1946No ratings yet
- Refund Form: To Be Acomplished by The Accounting OfficeDocument1 pageRefund Form: To Be Acomplished by The Accounting OfficeKim Kelley AngNo ratings yet
- SBS Course Registration FormDocument1 pageSBS Course Registration FormHAFIZ IMRAN AKHTERNo ratings yet
- Migration CertificateDocument2 pagesMigration CertificateDivyesh DeshmukhNo ratings yet
- Borang Pengambilan Transkrip AkademikDocument3 pagesBorang Pengambilan Transkrip AkademikDila OthmanNo ratings yet
- Form No GJS1Document6 pagesForm No GJS1NIKHIL SWAMY B C0% (1)
- Pit Loa Template 2022Document2 pagesPit Loa Template 2022atejoy12jesuscaresNo ratings yet
- Application Form: (Facebook, Twitter, Instagram, Etc.)Document1 pageApplication Form: (Facebook, Twitter, Instagram, Etc.)Merylcyne Bangsao SimsimNo ratings yet
- Terms of Payment 1 Pay't.-Due Date Amount 2 Pay't. - Due Date Amount Full Pay't. - Due Date AmountDocument1 pageTerms of Payment 1 Pay't.-Due Date Amount 2 Pay't. - Due Date Amount Full Pay't. - Due Date AmountwahahahahahahahaNo ratings yet
- Dai, Yang YiDocument2 pagesDai, Yang YiyangyiNo ratings yet
- Orca Share Media1674683686186 7024132483704734148Document1 pageOrca Share Media1674683686186 7024132483704734148kimNo ratings yet
- Registration Form: Institute of Cost & Management Accountants of PakistanDocument1 pageRegistration Form: Institute of Cost & Management Accountants of PakistanHira Kanwal MirzaNo ratings yet
- Registration FormDocument2 pagesRegistration Formelyas mustefaNo ratings yet
- Directorate of Iba Community Colleges & Schools: Bank ChallanDocument2 pagesDirectorate of Iba Community Colleges & Schools: Bank Challanirfan_icil2099No ratings yet
- Student Request Form May 2020Document1 pageStudent Request Form May 2020Randhawa SukhmanNo ratings yet
- Admission - Readmission FormDocument1 pageAdmission - Readmission FormSiddesh PingaleNo ratings yet
- Annexure-1 (Revised in July 2019) Bonafide Certificate For Renewal of Scholarship (Use Blue Ink Pen Only)Document2 pagesAnnexure-1 (Revised in July 2019) Bonafide Certificate For Renewal of Scholarship (Use Blue Ink Pen Only)ANAND JOSE VARGHESENo ratings yet
- Admission Form PHD Public Health Spring 2023Document2 pagesAdmission Form PHD Public Health Spring 2023Irfan SalimNo ratings yet
- ClearanceDocument1 pageClearancehumacadeyt12No ratings yet
- Borang GraDocument4 pagesBorang GraNUR SUHANA HAMZAHNo ratings yet
- Study Permit: Working While Studying, Exemptions & How to ApplyFrom EverandStudy Permit: Working While Studying, Exemptions & How to ApplyNo ratings yet
- Higher Education Student Financial Aid: Compare and Contrast State Managed Higher Education Student Financial Aid in Canada and the America with the Ngo-Managed Grameen Bank Higher Education Financial Aid Services in BangladeshFrom EverandHigher Education Student Financial Aid: Compare and Contrast State Managed Higher Education Student Financial Aid in Canada and the America with the Ngo-Managed Grameen Bank Higher Education Financial Aid Services in BangladeshNo ratings yet
- Module 1 Lesson 1 Laplace TransformDocument13 pagesModule 1 Lesson 1 Laplace TransformVictor DoyoganNo ratings yet
- Fourier Series AnalysisDocument23 pagesFourier Series AnalysisVictor DoyoganNo ratings yet
- 1.1 Off-Grid+Complete+ProgramDocument15 pages1.1 Off-Grid+Complete+ProgramVictor DoyoganNo ratings yet
- Half Range Fourier SeriesDocument18 pagesHalf Range Fourier SeriesVictor DoyoganNo ratings yet
- Title: Click Here To Add SubtitleDocument2 pagesTitle: Click Here To Add SubtitleVictor DoyoganNo ratings yet
- Proposed Workflow For PLS-POLE: Power Line SystemsDocument17 pagesProposed Workflow For PLS-POLE: Power Line SystemsVictor DoyoganNo ratings yet
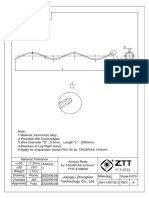
- 5 Drawing ZTT Line HardwareDocument2 pages5 Drawing ZTT Line HardwareVictor DoyoganNo ratings yet
- 12 Drawing TBEA Earthing Wire 240mm2Document2 pages12 Drawing TBEA Earthing Wire 240mm2Victor DoyoganNo ratings yet
- 6 Drawing ZTT OPGW AccessoriesDocument5 pages6 Drawing ZTT OPGW AccessoriesVictor DoyoganNo ratings yet
- WEJLOK Wedge Connector: Features and BenefitsDocument1 pageWEJLOK Wedge Connector: Features and BenefitsVictor DoyoganNo ratings yet
- Alumacore Opgw: Fiber Optic CableDocument2 pagesAlumacore Opgw: Fiber Optic CableVictor DoyoganNo ratings yet
- ZTT 66kV PDFDocument1 pageZTT 66kV PDFVictor DoyoganNo ratings yet
- ZTT Duct Cable 20-109788-2-ADocument8 pagesZTT Duct Cable 20-109788-2-AVictor DoyoganNo ratings yet
- Kew4105a 2eDocument2 pagesKew4105a 2eVictor DoyoganNo ratings yet
- Specs ZTT OPGW 24 Fibers PDFDocument9 pagesSpecs ZTT OPGW 24 Fibers PDFVictor DoyoganNo ratings yet
- Specs ZTT TACSR AW 410 PDFDocument5 pagesSpecs ZTT TACSR AW 410 PDFVictor DoyoganNo ratings yet
- American Wire Company ProfileDocument29 pagesAmerican Wire Company ProfileVictor DoyoganNo ratings yet
- Technical Data Sheet 3#5 Copper Clad Steel Wire: ITEM CODE - 600305Document2 pagesTechnical Data Sheet 3#5 Copper Clad Steel Wire: ITEM CODE - 600305Victor DoyoganNo ratings yet
- Hdpe Technical Data Sheet 150Mm 20200201v5Document1 pageHdpe Technical Data Sheet 150Mm 20200201v5Victor Doyogan100% (1)
- 1994-A Simplified Synthesis of Transmission Lines With A Tree Structure PDFDocument12 pages1994-A Simplified Synthesis of Transmission Lines With A Tree Structure PDFVictor DoyoganNo ratings yet
- United States Department of Agriculture Rural Utilities ServiceDocument55 pagesUnited States Department of Agriculture Rural Utilities ServiceVictor DoyoganNo ratings yet
- Mscmpds PDFDocument1 pageMscmpds PDFVictor DoyoganNo ratings yet
- UnitedStates 20210507 EpochTimesDocument28 pagesUnitedStates 20210507 EpochTimesKeithStewartNo ratings yet
- CDMA Non Availability Certificate For Death Application Form PDFDocument1 pageCDMA Non Availability Certificate For Death Application Form PDFjeeva prakash AmarlapudiNo ratings yet
- SHANMUGAM V PUBLIC PROSECUTOR, (1971) 1 MLJ 283 - EditedDocument3 pagesSHANMUGAM V PUBLIC PROSECUTOR, (1971) 1 MLJ 283 - EditedHayatul husnaNo ratings yet
- Department of Justice Lawsuit Against Yale University For Racial DiscriminationDocument32 pagesDepartment of Justice Lawsuit Against Yale University For Racial DiscriminationThe College FixNo ratings yet
- J SoxDocument3 pagesJ SoxJ LNo ratings yet
- VOID AGREEMENTS Expressly DeclaredDocument3 pagesVOID AGREEMENTS Expressly DeclaredBharathi Priya.SNo ratings yet
- Notice of Hearing (Criminal) For Bryan KohbergerDocument1 pageNotice of Hearing (Criminal) For Bryan KohbergerStephanie Pagones100% (1)
- Class 6 Unit 7 Fair PlayDocument3 pagesClass 6 Unit 7 Fair PlayThiagarajan KamananNo ratings yet
- Guidance On Involuntary and Emergency AdmissionsDocument8 pagesGuidance On Involuntary and Emergency AdmissionsMarianNo ratings yet
- Tamil Nadu Medical Services Corporation Limited: WWW - Tenders.tn - Gov.inDocument15 pagesTamil Nadu Medical Services Corporation Limited: WWW - Tenders.tn - Gov.inpraveenramanujamNo ratings yet
- Petition For Judicial Separation Section 10Document2 pagesPetition For Judicial Separation Section 10rachit mishraNo ratings yet
- Legal Issues On EducationDocument76 pagesLegal Issues On Educationasher pascoNo ratings yet
- Concerned Officials of The Mwss v. VasquezDocument2 pagesConcerned Officials of The Mwss v. VasquezVian O.No ratings yet
- FIN 630.assignmentDocument2 pagesFIN 630.assignmentMuhammad ArbazNo ratings yet
- 1 Au Meng NamDocument16 pages1 Au Meng NamSellamal ServaiNo ratings yet
- Glossary English Nepali-TypedDocument52 pagesGlossary English Nepali-TypedSusmita PariyarNo ratings yet
- Name: Quiz: Places Around Town: DateDocument5 pagesName: Quiz: Places Around Town: DateIsabel EcheverriaNo ratings yet
- Press Laws and Press in PakistanDocument41 pagesPress Laws and Press in PakistanNaveera AliNo ratings yet
- Barbuco Vs BeltranDocument5 pagesBarbuco Vs Beltrancertiorari19No ratings yet
- Dipa 1040 Introduction To Government and Politics IDocument105 pagesDipa 1040 Introduction To Government and Politics IJonathanNo ratings yet
- School Admission Appeals Code 1 February 2012 PDFDocument29 pagesSchool Admission Appeals Code 1 February 2012 PDFasismondNo ratings yet
- Tourist Tax ApplicationDocument4 pagesTourist Tax ApplicationBogdan MateiNo ratings yet
- Crim 5 - ModuleDocument9 pagesCrim 5 - ModuleShe Lah Fene QuitoNo ratings yet
- Motion For Reduction of BailbondDocument3 pagesMotion For Reduction of BailbondJo FallarmeNo ratings yet
- Directions To CHS For Corona Virus PDFDocument3 pagesDirections To CHS For Corona Virus PDFsujit0% (1)
- House Concurrent Resolution 013Document5 pagesHouse Concurrent Resolution 013LarryDCurtisNo ratings yet
- 69 Am JComp L44Document50 pages69 Am JComp L44Rakesh KumarNo ratings yet
- Germany JSV - Eligibility Assessment Report - Positive (Bangalore RegDocument19 pagesGermany JSV - Eligibility Assessment Report - Positive (Bangalore RegPaturu VijayNo ratings yet
- Special Power Attorney ATPDocument1 pageSpecial Power Attorney ATPRobert MarollanoNo ratings yet