Download as pdf or txt
You might also like
- Anti-Bias Classroom Observation Checklist Environmental EvaluationDocument6 pagesAnti-Bias Classroom Observation Checklist Environmental EvaluationNatalieNo ratings yet
- Common App Secondary School ReportDocument5 pagesCommon App Secondary School Reportelica81topsNo ratings yet
- Form 101 NewDocument2 pagesForm 101 NewJuliana HectorNo ratings yet
- Sample ASD Team Report FormatDocument12 pagesSample ASD Team Report FormatravibhargavaraamNo ratings yet
- The Many Faces of Mental Health in KenyaDocument58 pagesThe Many Faces of Mental Health in KenyaEdward KakumuNo ratings yet
- WEL201A - Full Study Guide - 140814 PDFDocument162 pagesWEL201A - Full Study Guide - 140814 PDFkevinwoods786_863449No ratings yet
- 2018 Alp National Platform ConstitutionDocument310 pages2018 Alp National Platform ConstitutionMichael SmithNo ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- Intake Interview ChildDocument8 pagesIntake Interview ChildKaz AmosNo ratings yet
- Hand Outs For Special EducationDocument27 pagesHand Outs For Special EducationArjay JacobNo ratings yet
- Assessment and Planning Tool: Idaho Infant Toddler Program Individualized Family Service Plan - Part 1Document19 pagesAssessment and Planning Tool: Idaho Infant Toddler Program Individualized Family Service Plan - Part 1takemebrickNo ratings yet
- Form SSA-3368-BKDocument14 pagesForm SSA-3368-BKGARY SELLSNo ratings yet
- UntitledATTENTION DEFICIT HYPERACTIVITY DISDER (ADHD)Document6 pagesUntitledATTENTION DEFICIT HYPERACTIVITY DISDER (ADHD)Fábio PinheiroNo ratings yet
- Interview Consent FINLDocument5 pagesInterview Consent FINLChan Chanielou JavierNo ratings yet
- BSBDIV501 Assessment 1Document11 pagesBSBDIV501 Assessment 1carol vivasNo ratings yet
- The Developmental Disabilities Institute at Wayne State University Webinar With Autism NOW May 5, 2011Document41 pagesThe Developmental Disabilities Institute at Wayne State University Webinar With Autism NOW May 5, 2011The Autism NOW CenterNo ratings yet
- Kiera Groves EP Services School Information FormDocument7 pagesKiera Groves EP Services School Information Formcpark321No ratings yet
- 298 QuestionnaireDocument6 pages298 QuestionnaireAnna Jubairah DimaocorNo ratings yet
- Teacherspecialed BDocument15 pagesTeacherspecialed BAnlyn PegaNo ratings yet
- Adults With LD and AssessmentDocument4 pagesAdults With LD and AssessmentramaaNo ratings yet
- Ldaamerica Org-Eligibility Determining Whether A Child Is Eligible For Special Education ServicesDocument4 pagesLdaamerica Org-Eligibility Determining Whether A Child Is Eligible For Special Education Servicesapi-340719486No ratings yet
- Focus Competency Essential Learning Competency (Melc)Document7 pagesFocus Competency Essential Learning Competency (Melc)Joseph Patrick OcapanNo ratings yet
- Rightsrev 2009Document21 pagesRightsrev 2009api-262004790No ratings yet
- Autism Program: Welcome PacketDocument17 pagesAutism Program: Welcome PacketMNo ratings yet
- Template Parental Permission (Reference)Document4 pagesTemplate Parental Permission (Reference)Rodziyah DahalanNo ratings yet
- Application FormDocument6 pagesApplication FormSanjeevan BaraNo ratings yet
- Nottinghamshire Hospice External Employment Application Form 2021Document8 pagesNottinghamshire Hospice External Employment Application Form 2021drtengheesaucho1980No ratings yet
- Assessment GuidanceDocument46 pagesAssessment GuidancetiggieNo ratings yet
- Institutional Review BoardDocument5 pagesInstitutional Review Boardapi-609434428No ratings yet
- ParentguidenovDocument54 pagesParentguidenovapi-296414662No ratings yet
- ACT - Child and Adolescent Intake Questionnaire PDFDocument16 pagesACT - Child and Adolescent Intake Questionnaire PDFPatty CrawfordNo ratings yet
- Human Subject Research Sample Letter of ConsentDocument7 pagesHuman Subject Research Sample Letter of ConsentKaloy KamaoNo ratings yet
- P01A: Personal Illness/Disability: What You Need To DoDocument4 pagesP01A: Personal Illness/Disability: What You Need To DoHenry OkoyeNo ratings yet
- Hca Application FormDocument8 pagesHca Application Formkawsarahmed7651No ratings yet
- Parent Notice of Procedural SafeguardsDocument15 pagesParent Notice of Procedural Safeguardsapi-269097655No ratings yet
- Exhibit F Template For Parental PermissionDocument2 pagesExhibit F Template For Parental PermissionKasthuri SubramaniamNo ratings yet
- Guidance Asd 08-1Document5 pagesGuidance Asd 08-1api-252404660No ratings yet
- SLP Student Intake Form Referral Consent Case HistoryDocument3 pagesSLP Student Intake Form Referral Consent Case Historyapi-617678622No ratings yet
- Aailyah - Pre Refferal Form PortfolioDocument4 pagesAailyah - Pre Refferal Form Portfolioapi-643371905No ratings yet
- InterviewDocument6 pagesInterviewMUSYOKA KITUKUNo ratings yet
- Function Report - Adult - Form Ssa-3373-Bk: Read All of This Information Before You Begin Completing This FormDocument10 pagesFunction Report - Adult - Form Ssa-3373-Bk: Read All of This Information Before You Begin Completing This FormDouglas NogueiraNo ratings yet
- Psychoeducational Report Shell TemplateDocument68 pagesPsychoeducational Report Shell TemplateDeborah Schneider100% (1)
- UT Dallas Syllabus For cldp3342.501.11s Taught by John Barfoot (jwb043000)Document4 pagesUT Dallas Syllabus For cldp3342.501.11s Taught by John Barfoot (jwb043000)UT Dallas Provost's Technology GroupNo ratings yet
- PECS Example SLD Dyslexia Dysgraphia Dyscalculia Report - 1 - M 16857773Document30 pagesPECS Example SLD Dyslexia Dysgraphia Dyscalculia Report - 1 - M 16857773peachypeachyNo ratings yet
- MPAS SurveyDocument4 pagesMPAS SurveyABrennan88No ratings yet
- b23 Eval - AssesguidanceDocument11 pagesb23 Eval - AssesguidanceKaren ClarkNo ratings yet
- Inform Consent CompletedDocument4 pagesInform Consent Completedapi-547830791No ratings yet
- Parent Expectations SurveyDocument6 pagesParent Expectations SurveyAiza BabaoNo ratings yet
- Individual Inventory Form LongDocument3 pagesIndividual Inventory Form LongNica Talampas LunaNo ratings yet
- QUESTIONNAIRE For Providers - EngDocument8 pagesQUESTIONNAIRE For Providers - EngLighto RyusakiNo ratings yet
- Inbound 7386960521384046796Document2 pagesInbound 7386960521384046796Kaitlyn Ferretti DivineNo ratings yet
- Ssa 3369Document10 pagesSsa 3369Allison CriderNo ratings yet
- UT Dallas Syllabus For Psy3342.501.10s Taught by John Barfoot (jwb043000)Document4 pagesUT Dallas Syllabus For Psy3342.501.10s Taught by John Barfoot (jwb043000)UT Dallas Provost's Technology GroupNo ratings yet
- UT Dallas Syllabus For Psy3342.501.08s Taught by John Barfoot (jwb043000)Document4 pagesUT Dallas Syllabus For Psy3342.501.08s Taught by John Barfoot (jwb043000)UT Dallas Provost's Technology GroupNo ratings yet
- Suspecting Disability: Contents of This SectionDocument30 pagesSuspecting Disability: Contents of This SectionDavid RitterNo ratings yet
- Description: Tags: AppendixDStudentInterviewQuestionsDocument5 pagesDescription: Tags: AppendixDStudentInterviewQuestionsanon-24797No ratings yet
- Special Education Crash CourseDocument10 pagesSpecial Education Crash CourseSteven Beech100% (1)
- Participant Information Sheet - YouthDocument6 pagesParticipant Information Sheet - YouthYhuon Gheine Cariño LnameNo ratings yet
- Financial Aid ReflectionDocument4 pagesFinancial Aid Reflectionapi-616168546No ratings yet
- PECS Example Autism ReportDocument40 pagesPECS Example Autism ReportgenerjustnNo ratings yet
- Forensic Mental Health Assistant: Passbooks Study GuideFrom EverandForensic Mental Health Assistant: Passbooks Study GuideNo ratings yet
- UNITED STATES HISTORY AND GOVERNMENT: Passbooks Study GuideFrom EverandUNITED STATES HISTORY AND GOVERNMENT: Passbooks Study GuideNo ratings yet
- Senior Clinical Psychologist: Passbooks Study GuideFrom EverandSenior Clinical Psychologist: Passbooks Study GuideNo ratings yet
- Final Reggio LNMDocument34 pagesFinal Reggio LNMtadilakshmikiranNo ratings yet
- 1326473753ap Course Book July 2011Document87 pages1326473753ap Course Book July 2011tadilakshmikiranNo ratings yet
- E Bank ManualDocument9 pagesE Bank ManualtadilakshmikiranNo ratings yet
- Brigham Young University College of NursingDocument6 pagesBrigham Young University College of NursingtadilakshmikiranNo ratings yet
- 2021 Mpfs Proposed Rule RvusDocument14 pages2021 Mpfs Proposed Rule RvustadilakshmikiranNo ratings yet
- Government Schemes For Senior CitizensDocument12 pagesGovernment Schemes For Senior CitizenstadilakshmikiranNo ratings yet
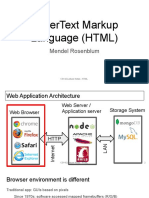
- Hypertext Markup Language (HTML) : Mendel RosenblumDocument22 pagesHypertext Markup Language (HTML) : Mendel RosenblumtadilakshmikiranNo ratings yet
- BA in International Relations (570142) MAP SheetDocument4 pagesBA in International Relations (570142) MAP SheettadilakshmikiranNo ratings yet
- Brigham Young University: Campus Map & ServicesDocument2 pagesBrigham Young University: Campus Map & ServicestadilakshmikiranNo ratings yet
- Volume Correction Factors - Diesel Fuel: Issued: July 2018Document5 pagesVolume Correction Factors - Diesel Fuel: Issued: July 2018tadilakshmikiranNo ratings yet
- Failures of The VCG Mechanism in Combinatorial Auctions and ExchangesDocument8 pagesFailures of The VCG Mechanism in Combinatorial Auctions and ExchangestadilakshmikiranNo ratings yet
- Bidding To The Top: VCG and Equilibria of Position-Based AuctionsDocument14 pagesBidding To The Top: VCG and Equilibria of Position-Based AuctionstadilakshmikiranNo ratings yet
- Vcgfailures AAMAS06Document8 pagesVcgfailures AAMAS06tadilakshmikiranNo ratings yet
- Vickrey AuctionDocument23 pagesVickrey AuctiontadilakshmikiranNo ratings yet
- Exemption Under Section 54B of The Income-Tax Act Is Available To A Taxpayer Only When The Asset Is Purchased in Its Own NameDocument3 pagesExemption Under Section 54B of The Income-Tax Act Is Available To A Taxpayer Only When The Asset Is Purchased in Its Own NametadilakshmikiranNo ratings yet
- Information Brochure - 2022Document35 pagesInformation Brochure - 2022Manjushree InfratechNo ratings yet
- Embracing Special Education Chapter 4Document24 pagesEmbracing Special Education Chapter 4Sevillano GerraNo ratings yet
- Theme 7 Task SheetDocument14 pagesTheme 7 Task Sheetალექსანდრე იაშაღაშვილიNo ratings yet
- PERSONALITY DISORDER prt3Document2 pagesPERSONALITY DISORDER prt3Maria Franchisca AsioNo ratings yet
- Acs 4Document25 pagesAcs 4Carolina UrrutiaNo ratings yet
- Delusional DisorderDocument4 pagesDelusional DisorderNajm Us Saqib BhatNo ratings yet
- TPA Advertise 2023Document3 pagesTPA Advertise 2023amethyst amberNo ratings yet
- Carballo2019 Article PsychosocialRiskFactorsForSuicDocument18 pagesCarballo2019 Article PsychosocialRiskFactorsForSuicAngelina Sosa LoveraNo ratings yet
- Early Mobilitation For Critically Ill Patients in ICUDocument34 pagesEarly Mobilitation For Critically Ill Patients in ICUririNo ratings yet
- Education Sciences: Inclusion and Special EducationDocument17 pagesEducation Sciences: Inclusion and Special Educationzed cozNo ratings yet
- Use of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyDocument5 pagesUse of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyRafael MartinsNo ratings yet
- Marginalized EssayDocument4 pagesMarginalized EssayAhyyaNo ratings yet
- October 2, 2015 Strathmore TimesDocument32 pagesOctober 2, 2015 Strathmore TimesStrathmore TimesNo ratings yet
- Case Study PsychologyDocument5 pagesCase Study PsychologysymbianizeNo ratings yet
- Eye Injuries PDFDocument9 pagesEye Injuries PDFfirdausrizaNo ratings yet
- HumanDocument6 pagesHumanVesna BratovcicNo ratings yet
- A Beautiful MindDocument3 pagesA Beautiful Mindapi-31479794675% (4)
- Term Paper in Record ManagementDocument46 pagesTerm Paper in Record ManagementJonicaJaneJoseNo ratings yet
- III Magna Carta For PWDsDocument25 pagesIII Magna Carta For PWDsDiannah Anne Cuevas ZendonNo ratings yet
- Rights of Physically and Mentally Disabled PersonsDocument11 pagesRights of Physically and Mentally Disabled Personsluis capulongNo ratings yet
- Philippians 4 13 - PPT DEFENSEDocument17 pagesPhilippians 4 13 - PPT DEFENSESherwina Marie del RosarioNo ratings yet
- Checklist MseDocument6 pagesChecklist MseHerlene Lyneth ZalamedaNo ratings yet
- Kearney Albano 2004 School RefusalDocument15 pagesKearney Albano 2004 School Refusalrahmah.hayya00No ratings yet
- Gmail - Your ADHD Test Results Are InsideDocument2 pagesGmail - Your ADHD Test Results Are InsideЛьшаNo ratings yet
- Use of Icf To Build A Common Language Among Professionals in Disability Management and RehabilitationDocument3 pagesUse of Icf To Build A Common Language Among Professionals in Disability Management and RehabilitationIJAR JOURNALNo ratings yet
- Initial Nurse - Docx NPI NPIDocument22 pagesInitial Nurse - Docx NPI NPIIyanna BaylonNo ratings yet