Download as pdf or txt
You might also like
- Magic MouthwashDocument5 pagesMagic MouthwashAdiAri Rosiu100% (3)
- Hashimoto ThyroiditisDocument6 pagesHashimoto Thyroiditismananginsiang100% (1)
- Bleeding DisordersDocument92 pagesBleeding DisordersIsaac MwangiNo ratings yet
- w4364b46a 1674498684489-КопияDocument41 pagesw4364b46a 1674498684489-КопияSultan HaiderNo ratings yet
- Far-Print OutDocument92 pagesFar-Print OutChandru ManjunathNo ratings yet
- Path 548 Coag Disorders 20150323Document38 pagesPath 548 Coag Disorders 20150323Bakul DalalNo ratings yet
- Platelets PDFDocument65 pagesPlatelets PDFLana AmerieNo ratings yet
- HemostasisDocument48 pagesHemostasisBintang Ruth Cecilia FebrinaNo ratings yet
- HemostasisDocument48 pagesHemostasissianturisuryaNo ratings yet
- Perdarahan: DR - Suhaemi, SPPD, FinasimDocument27 pagesPerdarahan: DR - Suhaemi, SPPD, Finasimwie_wie_wieNo ratings yet
- Platelets: Veena ShriramDocument58 pagesPlatelets: Veena ShriramVeena ShriramNo ratings yet
- Platelets in Cardiovascular Disease: DR Isobel Ford Dept of Medicine & TherapeuticsDocument41 pagesPlatelets in Cardiovascular Disease: DR Isobel Ford Dept of Medicine & Therapeuticsapi-19916399No ratings yet
- PATH - Bleeding Disorders (7p)Document7 pagesPATH - Bleeding Disorders (7p)Omar HamwiNo ratings yet
- Kasus 1Document64 pagesKasus 1drroytambunanNo ratings yet
- Ilovepdf Merged-3Document59 pagesIlovepdf Merged-3idon'tgiveachogiwaNo ratings yet
- 3.1 HaemostasisDocument53 pages3.1 HaemostasisFarnida Jamhal100% (1)
- 25-26 Vascular and Platelet Abnormalities &TMA FinalDocument34 pages25-26 Vascular and Platelet Abnormalities &TMA FinalAhmed MansourNo ratings yet
- Examinations of Coagulation Disturbances: Jan Živný Department of PathophysiologyDocument68 pagesExaminations of Coagulation Disturbances: Jan Živný Department of Pathophysiologyivana.begic.1960No ratings yet
- Bleeding DisordersDocument35 pagesBleeding Disorderskholoud220100% (3)
- 3 Hemostasis, Hemorrhagic Diathesis and ThrombosisDocument55 pages3 Hemostasis, Hemorrhagic Diathesis and ThrombosisSuman MahmoodNo ratings yet
- Hemostasis in The Surgical PatientDocument39 pagesHemostasis in The Surgical Patientninjahattori1No ratings yet
- Hemophilia and Coagulation Disorders: DR Nishant VermaDocument68 pagesHemophilia and Coagulation Disorders: DR Nishant VermaЮлия ЦыгановаNo ratings yet
- Lecture 5Document48 pagesLecture 5Ahed ShaerNo ratings yet
- Coagulation DisordersDocument40 pagesCoagulation DisordersDr. Shatdal Chaudhary100% (6)
- 2 Thrombocyte ImmunologyDocument29 pages2 Thrombocyte ImmunologyDinda KusumaNo ratings yet
- Hematology: A/Prof. Nguyen Thi Hue 2023 University of ScienceDocument74 pagesHematology: A/Prof. Nguyen Thi Hue 2023 University of ScienceMai Ly NguyễnNo ratings yet
- How To Handle The Bleeding Patient: Nick BexfieldDocument40 pagesHow To Handle The Bleeding Patient: Nick Bexfieldapi-270059878No ratings yet
- He Most AsiaDocument59 pagesHe Most AsiaUlises VillanuevaNo ratings yet
- Week 5: Trigger 3 Theme of The Week: Haemostasis: Full Blood CountDocument30 pagesWeek 5: Trigger 3 Theme of The Week: Haemostasis: Full Blood CountFrances Lau Yee ChinNo ratings yet
- Path Hematology ReviewDocument19 pagesPath Hematology ReviewChristopher MuellerNo ratings yet
- 10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)Document45 pages10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)MUHAMMAD BAGIR ALJUFRINo ratings yet
- Bleeding TestsDocument66 pagesBleeding TestsMohiedine AbouljoudNo ratings yet
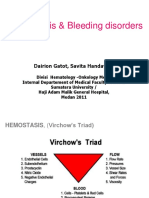
- Bleeding Disorders: Dairion Gatot, Soegiarto Gani, Savita HandayaniDocument50 pagesBleeding Disorders: Dairion Gatot, Soegiarto Gani, Savita HandayaniririsNo ratings yet
- Coagulation disorders-MS1Document46 pagesCoagulation disorders-MS1Chamika Huruggamuwa100% (1)
- The Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsDocument12 pagesThe Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsTamara Silva FabresNo ratings yet
- Disseminated Intravascular CoagulationDocument7 pagesDisseminated Intravascular CoagulationSunaina AdhikariNo ratings yet
- Bleeding Disorders: Vascular AbnormalitiesDocument21 pagesBleeding Disorders: Vascular AbnormalitiesFirman AmalNo ratings yet
- Aspek Klinis Fibrinogen Dan D-DimerDocument43 pagesAspek Klinis Fibrinogen Dan D-DimerDyan JeanovaNo ratings yet
- Anticoagulant Anti Platelet Fibrinolytic Drugs08 Black and WhiteDocument28 pagesAnticoagulant Anti Platelet Fibrinolytic Drugs08 Black and WhiteJagdesh SajnaniNo ratings yet
- Lecture - Platelet, Haemostasis - 2Document19 pagesLecture - Platelet, Haemostasis - 2eman el saeedNo ratings yet
- Hemorrhagic Diatheses Engl. PP1Document90 pagesHemorrhagic Diatheses Engl. PP1Natalia MinzatuNo ratings yet
- Bleeding Disorders Tandem Desember 2019Document47 pagesBleeding Disorders Tandem Desember 2019reshaNo ratings yet
- Bleeding Disorders Tandem Desember 2019Document47 pagesBleeding Disorders Tandem Desember 2019reshaNo ratings yet
- Clinical Approach of Bleeding Problems in Childhood: Novie Amelia ChozieDocument38 pagesClinical Approach of Bleeding Problems in Childhood: Novie Amelia ChoziebennyrolandnababanNo ratings yet
- 2 Thrombocyte ImmunologyDocument30 pages2 Thrombocyte ImmunologyDinda KusumaNo ratings yet
- Merged 2022 11 30 21-19-53Document45 pagesMerged 2022 11 30 21-19-53DTM FHKNo ratings yet
- Haemostasis: Case StudyDocument19 pagesHaemostasis: Case StudyTusabe FredNo ratings yet
- Whydoesmypatienthave Thrombocytopenia?: Ellice Y. Wong,, Michal G. RoseDocument22 pagesWhydoesmypatienthave Thrombocytopenia?: Ellice Y. Wong,, Michal G. RoseLilasNo ratings yet
- Kelainan Perdarahan Kelainan PembekuanDocument28 pagesKelainan Perdarahan Kelainan PembekuanEga FlorenceNo ratings yet
- Disorder of HemostasisDocument26 pagesDisorder of HemostasisHassan Al SinanNo ratings yet
- Hema - PointersDocument5 pagesHema - PointersLUALHATI VILLASNo ratings yet
- Hema Platelet DisordersDocument13 pagesHema Platelet DisordersJennie Grace MaloomNo ratings yet
- 1 Blood HemostasisDocument32 pages1 Blood Hemostasisarlinda noviana100% (2)
- Bleeding Disorders 082508Document46 pagesBleeding Disorders 082508Muhammad ShaikhNo ratings yet
- Hematology Board Review 2Document33 pagesHematology Board Review 2Edwin OkonNo ratings yet
- 5 Bleeding Disorders PPT EditedDocument87 pages5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNo ratings yet
- Bleeding Disorders: Dr. Vishal Saxena MBBS, MD (Path), FicmrDocument59 pagesBleeding Disorders: Dr. Vishal Saxena MBBS, MD (Path), Ficmrmus zaharaNo ratings yet
- Bleeding DisordersDocument62 pagesBleeding DisordersxtineNo ratings yet
- Fast Facts: Deficit di piruvato chinasi: Per una maggiore sensibilizzazione su questa rara malattia geneticaFrom EverandFast Facts: Deficit di piruvato chinasi: Per una maggiore sensibilizzazione su questa rara malattia geneticaNo ratings yet
- Deep Vein Thrombosis and Pulmonary Embolism: A guide for practitioners 2/edFrom EverandDeep Vein Thrombosis and Pulmonary Embolism: A guide for practitioners 2/edRating: 5 out of 5 stars5/5 (1)
- The Seqirus Portfolio of Influenza Vaccines-2021-2022 SeasonDocument2 pagesThe Seqirus Portfolio of Influenza Vaccines-2021-2022 SeasonKari BallardNo ratings yet
- 564-Article Text-1743-1-10-20210707Document14 pages564-Article Text-1743-1-10-20210707JL CalvinNo ratings yet
- Self-Declaration / Undertaking by Research Scholar / Student / (Returning To IITM Hostel)Document3 pagesSelf-Declaration / Undertaking by Research Scholar / Student / (Returning To IITM Hostel)Laxmith ShettyNo ratings yet
- 2005 - Recommendations For DX and TTMT of Acute PorphyriasDocument13 pages2005 - Recommendations For DX and TTMT of Acute PorphyriasDavidArangoNo ratings yet
- MJHS 17 (3) 0Document154 pagesMJHS 17 (3) 0Andrei ChiriacNo ratings yet
- Adhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyDocument6 pagesAdhesive Capsulitis of The Shoulder: Protocol For The Adhesive Capsulitis Biomarker (Adcab) StudyRuben FigueroaNo ratings yet
- Pharma Midterms Review UwuDocument11 pagesPharma Midterms Review UwuAJ BayNo ratings yet
- NCM 106 AntiviralDocument34 pagesNCM 106 AntiviralJod BellNo ratings yet
- Presented By: Course Code: PHR510 Section: 1 Submitted To: Ms. Tahmina YasminDocument25 pagesPresented By: Course Code: PHR510 Section: 1 Submitted To: Ms. Tahmina YasminXd DipNo ratings yet
- Pathogenic Yield of Genetic Testing in Autism Spectrum DisorderDocument11 pagesPathogenic Yield of Genetic Testing in Autism Spectrum DisorderRaul Morales VillegasNo ratings yet
- Jurnal Anemia Bahasa InggrisDocument9 pagesJurnal Anemia Bahasa InggrisonyourmargotNo ratings yet
- Diagnosis and Management of Ureteric Injury: An Evidence-Based AnalysisDocument13 pagesDiagnosis and Management of Ureteric Injury: An Evidence-Based AnalysisqalbiNo ratings yet
- Drug StudyDocument10 pagesDrug StudyNine SaguiboNo ratings yet
- Maribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNDocument46 pagesMaribel D. Fuentes, SN Jimson Altomia, SN: Kieth Amei Falalimpa, SNJam CorrosNo ratings yet
- Chapter - 9 The Spurious Drug Menance & Remedy: AbstractDocument12 pagesChapter - 9 The Spurious Drug Menance & Remedy: Abstractbindu3No ratings yet
- Steroid Injections: Read This If You Are Planning On Having A Steroid InjectionDocument3 pagesSteroid Injections: Read This If You Are Planning On Having A Steroid InjectionyudhaNo ratings yet
- Cancer CaDocument6 pagesCancer CaRocco WalksNo ratings yet
- Technical Specification: Nutritional AssessmentDocument2 pagesTechnical Specification: Nutritional AssessmentBjörn Þór SigurbjörnssonNo ratings yet
- BEKAMDocument26 pagesBEKAMeko rustamajiNo ratings yet
- DrugsDocument7 pagesDrugsCaine ReganNo ratings yet
- 627-Texto Do Artigo-1922-1-10-20201125Document5 pages627-Texto Do Artigo-1922-1-10-20201125Daniel GuimarãesNo ratings yet
- Comprehensive Notes For AB PsychDocument8 pagesComprehensive Notes For AB PsychCaila Ann PaglasNo ratings yet
- Breast ImplantDocument7 pagesBreast ImplantStevo JjNo ratings yet
- Concept MapDocument2 pagesConcept MapAngeline de GalaNo ratings yet
- Module 5-7Document37 pagesModule 5-7Clifford Lachica100% (1)
- Coronavirus or Covid-19 A Force Majeure Event?: Covid19-Forcemajeureeventarticlerevfwmlogo/Bke/19-Mar-20Document6 pagesCoronavirus or Covid-19 A Force Majeure Event?: Covid19-Forcemajeureeventarticlerevfwmlogo/Bke/19-Mar-20JaxSuperflyNo ratings yet
- Reset &restart Planning Guide DRAFTDocument12 pagesReset &restart Planning Guide DRAFTWKYC.com100% (3)
- Preeclampsia in PregnancyDocument15 pagesPreeclampsia in PregnancyCheru DugaseNo ratings yet