Download as pdf or txt
You might also like
- Gestational Diabetes Brochure ENGDocument2 pagesGestational Diabetes Brochure ENGP Zamora100% (2)
- Partus LamaDocument11 pagesPartus LamaSulis SipinNo ratings yet
- Journal Ectopic Pregnancy-A Rising TrendDocument5 pagesJournal Ectopic Pregnancy-A Rising TrendEricNo ratings yet
- Peripartum Hysterectomy: A Life Saving Procedure: Original ArticleDocument4 pagesPeripartum Hysterectomy: A Life Saving Procedure: Original ArticleEdwin MasholaNo ratings yet
- Screenshot 2023-08-12 at 8.06.08 AMDocument7 pagesScreenshot 2023-08-12 at 8.06.08 AMTahseenNo ratings yet
- Trial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsDocument8 pagesTrial of Labor at The Maternity Department of The Sourosanou University Hospital (Chuss) : Clinical Aspects, The Maternal and Perinatal PrognosticsIJAR JOURNALNo ratings yet
- Management of Obstetric Emergencies at The Maternity Center of The University Hospital Center of Ouemeplateau Chud Op in Benin 2167 0420 1000398Document6 pagesManagement of Obstetric Emergencies at The Maternity Center of The University Hospital Center of Ouemeplateau Chud Op in Benin 2167 0420 1000398zahalina90No ratings yet
- Rukhsana Turnitin Originality ReportDocument7 pagesRukhsana Turnitin Originality ReportMominah MayamNo ratings yet
- Maternal and Fetal Outcome of Placenta PDocument5 pagesMaternal and Fetal Outcome of Placenta Pfamelalusu eaNo ratings yet
- Merced 2019Document14 pagesMerced 2019Vanessa CarinoNo ratings yet
- An Analysis of Uterine Rupture at The Nnamdi AzikiweDocument5 pagesAn Analysis of Uterine Rupture at The Nnamdi AzikiweNublah Permata LestariNo ratings yet
- 1238 8440 1 PBDocument6 pages1238 8440 1 PBKriti KumariNo ratings yet
- Jsafog 9 323 PDFDocument4 pagesJsafog 9 323 PDFSul FadlyNo ratings yet
- Jurnal Internasional Plasenta PreviaDocument9 pagesJurnal Internasional Plasenta Previaptlanna1234No ratings yet
- Observational Study On Placenta Accreta Spectrum Disorders in A Tertiary Centre For Two YearsDocument7 pagesObservational Study On Placenta Accreta Spectrum Disorders in A Tertiary Centre For Two YearsIJAR JOURNALNo ratings yet
- Thesis On Ectopic Pregnancy in IndiaDocument7 pagesThesis On Ectopic Pregnancy in Indiaynwtcpwff100% (2)
- Clinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeDocument7 pagesClinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeIOSRjournalNo ratings yet
- Jurnal FetoDocument4 pagesJurnal FetoAl NaifNo ratings yet
- Study On Outcomes of PROMDocument5 pagesStudy On Outcomes of PROMRohit MaliNo ratings yet
- Moxibustion To Correct A Breech Presentation of The Fetus Author IDEASSDocument13 pagesMoxibustion To Correct A Breech Presentation of The Fetus Author IDEASSVraciul din VeciniNo ratings yet
- 04 Shehla20Noor 20PREVALANCE20OF20PRROM20AND20ITS20OUTCOMEDocument5 pages04 Shehla20Noor 20PREVALANCE20OF20PRROM20AND20ITS20OUTCOMEMirachel AugustNo ratings yet
- 2.april 2020 Estimation of Risk Factors For MultiparousDocument4 pages2.april 2020 Estimation of Risk Factors For MultiparousTushar BahetiNo ratings yet
- The Role of Ultrasound in ObstetricsDocument9 pagesThe Role of Ultrasound in ObstetricsHanun FaizaNo ratings yet
- 2017 - Maternal and Fetal OutcomesDocument4 pages2017 - Maternal and Fetal OutcomesTaklu Marama M. BaatiiNo ratings yet
- Journal Gyn KETDocument8 pagesJournal Gyn KETImaylani S. SitanggangNo ratings yet
- Caesarean in Rural Environment of Eastern Kasai (R.D. Congo) Cover of The Needs and Quality of The Services With Kasansa and TshilengeDocument8 pagesCaesarean in Rural Environment of Eastern Kasai (R.D. Congo) Cover of The Needs and Quality of The Services With Kasansa and TshilengeAnonymous SMEU6r2No ratings yet
- Forceps Deliveries and Fetomaternal Outcome in Modern ObstetricsDocument4 pagesForceps Deliveries and Fetomaternal Outcome in Modern ObstetricsKriti SinhaNo ratings yet
- Jurnal Internasional Ruptur UteriDocument5 pagesJurnal Internasional Ruptur UteriNovita MayasariNo ratings yet
- Rupture Uterus: A Clinical Analysis: Soma Bandyopadhyay, Sipra SinghDocument4 pagesRupture Uterus: A Clinical Analysis: Soma Bandyopadhyay, Sipra SinghanggiNo ratings yet
- Maternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanDocument12 pagesMaternal and Fetal Outcome in Emergency Caesarean Sections in Wad Medani Obstetrics and Gynaecology Hospital Gezira State-SudanIJAR JOURNALNo ratings yet
- Cervical Cerclage and It's Significance in Preventing Second Trimester Abortions Because of Cervical IncompetenceDocument7 pagesCervical Cerclage and It's Significance in Preventing Second Trimester Abortions Because of Cervical IncompetenceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ojog 2023071715223408Document12 pagesOjog 2023071715223408Julien BwamaNo ratings yet
- A Retrospective Study On Ectopic Pregnancy: A Two Year StudyDocument4 pagesA Retrospective Study On Ectopic Pregnancy: A Two Year StudyGung GiscaNo ratings yet
- Midtrimester Sonographic Cervical Length Measurement in Prediction of Preterm BirthDocument6 pagesMidtrimester Sonographic Cervical Length Measurement in Prediction of Preterm BirthIJAR JOURNALNo ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Clinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingDocument7 pagesClinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingNazia BhatNo ratings yet
- 1 PDFDocument7 pages1 PDFAlfa FebriandaNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Journal 1 - Plasenta PreviaDocument5 pagesJournal 1 - Plasenta Previarizky ferdina kevinNo ratings yet
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDocument8 pagesAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyNo ratings yet
- The Rate and Indication of Caesarean Section in ADocument7 pagesThe Rate and Indication of Caesarean Section in AdhananjayNo ratings yet
- MJCU Volume 86 Issue December Pages 4259-4265Document7 pagesMJCU Volume 86 Issue December Pages 4259-4265SamarNo ratings yet
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- Maternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018Document27 pagesMaternal and Perinatal Outcomes After Elective Labor Induction at 39 Weeks in Uncomplicated Singleton Pregnancies - A Meta-Analysis-sotiriadis2018trongnguyen2232000No ratings yet
- Arabin Pessary To Prevent Adverse Perinatal Outcomes in Twin Pregnancies With A Short Cervix, PESSARONE. Marion GroussollesDocument13 pagesArabin Pessary To Prevent Adverse Perinatal Outcomes in Twin Pregnancies With A Short Cervix, PESSARONE. Marion GroussollesqmfddnhdjmNo ratings yet
- Ojsadmin, 993Document6 pagesOjsadmin, 993pondyNo ratings yet
- Sociodemographic Profile and Outcome of Preterm Premature Rupture ofDocument8 pagesSociodemographic Profile and Outcome of Preterm Premature Rupture ofRohit MaliNo ratings yet
- Overview#a8: Uterine Rupture in PregnancyDocument13 pagesOverview#a8: Uterine Rupture in PregnancyFadillaLovianaIrwanNo ratings yet
- Objectives:: CorrespondenceDocument5 pagesObjectives:: Correspondenceraudatul jannahNo ratings yet
- Skor Tokolitik PDFDocument5 pagesSkor Tokolitik PDFrahayu muhsiNo ratings yet
- Metroplastia HisteroscopicaDocument8 pagesMetroplastia Histeroscopicaguerreroh38No ratings yet
- Obstetrical Outcomes in Women With ChorioamnionitisDocument6 pagesObstetrical Outcomes in Women With ChorioamnionitisCentral Asian StudiesNo ratings yet
- Good18.Prenatally Diagnosed Vasa Previa A.30Document9 pagesGood18.Prenatally Diagnosed Vasa Previa A.30wije0% (1)
- Awareness of Obstetric Danger Signs Among Pregnant Women in Tertiary Care Teaching HospitalDocument5 pagesAwareness of Obstetric Danger Signs Among Pregnant Women in Tertiary Care Teaching HospitalRachmat B SaputraNo ratings yet
- Evaluation of Clinical and Instrumental Results of Patients With A Risk of Development of Recurrent MissionDocument7 pagesEvaluation of Clinical and Instrumental Results of Patients With A Risk of Development of Recurrent MissionCentral Asian StudiesNo ratings yet
- SHDJDJDocument5 pagesSHDJDJkhusnulNo ratings yet
- Hemorragias Post PartoDocument58 pagesHemorragias Post PartoSael Vicente VidaurreNo ratings yet
- A Descriptive Study To Assess The Knowledge and Attitude Regarding Use of Emergency Contraceptive Pills As A Method of Contraception Among Female Staff Nurses of Rajindera Hospital PatialaDocument29 pagesA Descriptive Study To Assess The Knowledge and Attitude Regarding Use of Emergency Contraceptive Pills As A Method of Contraception Among Female Staff Nurses of Rajindera Hospital PatialaEditor IJTSRDNo ratings yet
- Comparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131Document4 pagesComparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131muhammad maadaNo ratings yet
- Ultrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolDocument7 pagesUltrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolPutu Gede WidyatamaNo ratings yet
- Employee Stress, Engagement, and Work OutcomesDocument21 pagesEmployee Stress, Engagement, and Work OutcomesErena HairunisaNo ratings yet
- Presentation APDIS Hodge Podge ICD 10 CM PCS Coding Issues 03.01.18Document17 pagesPresentation APDIS Hodge Podge ICD 10 CM PCS Coding Issues 03.01.18Erena HairunisaNo ratings yet
- Pathogenesis of Acne Vulgaris: Simplified: Review ArticleDocument5 pagesPathogenesis of Acne Vulgaris: Simplified: Review ArticleErena HairunisaNo ratings yet
- Pato HEP BDocument6 pagesPato HEP BErena HairunisaNo ratings yet
- MainDocument10 pagesMainErena HairunisaNo ratings yet
- Staphyloccocus AureusDocument11 pagesStaphyloccocus AureusErena HairunisaNo ratings yet
- Gambaran Radiologis BronkiolitisDocument7 pagesGambaran Radiologis BronkiolitisErena HairunisaNo ratings yet
- Research Article: Does Comorbidity Increase The Risk of Dengue Hemorrhagic Fever and Dengue Shock Syndrome?Document6 pagesResearch Article: Does Comorbidity Increase The Risk of Dengue Hemorrhagic Fever and Dengue Shock Syndrome?Erena HairunisaNo ratings yet
- Prevention of Preterm LabDocument6 pagesPrevention of Preterm LabDanTe D' WinchesterNo ratings yet
- CV Peneliti UtamaDocument14 pagesCV Peneliti Utamabidan lidiafNo ratings yet
- Pregnant Women Attending Antenatal Care and First Antenatal Care Visit in EthiopiaDocument8 pagesPregnant Women Attending Antenatal Care and First Antenatal Care Visit in EthiopiaAbu HajerahNo ratings yet
- Awareness About Janani Shishu Suraksha Karyakram (JSSK) Among Pregnant Mothers - A Community Based Study in A Rural Area of West Bengal, India.Document5 pagesAwareness About Janani Shishu Suraksha Karyakram (JSSK) Among Pregnant Mothers - A Community Based Study in A Rural Area of West Bengal, India.IOSRjournalNo ratings yet
- Breech Baby - Causes, Complications, Turning & DeliveryDocument5 pagesBreech Baby - Causes, Complications, Turning & DeliveryJoshua TomoNo ratings yet
- Diagnostic TestsDocument6 pagesDiagnostic TestsKelsey MacaraigNo ratings yet
- Partograph NextDocument50 pagesPartograph NextPrag GK Subedi0% (1)
- Creed Rise 2022 Topics - For Artps and NartpsDocument3 pagesCreed Rise 2022 Topics - For Artps and NartpsReg LagartejaNo ratings yet
- Proposal: JAKARTA UPDATE ON Gynecology Obstetrics 2Document22 pagesProposal: JAKARTA UPDATE ON Gynecology Obstetrics 2Costan Tryono Parulian RumapeaNo ratings yet
- Alarm I: Ourth Dition of The Nternational RogramDocument10 pagesAlarm I: Ourth Dition of The Nternational RogramayfanNo ratings yet
- Morning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsDocument8 pagesMorning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsEra MoetzNo ratings yet
- Obg Unit - PlanDocument2 pagesObg Unit - PlansimranNo ratings yet
- Determining Gravidity and Parity: I. GravidaDocument6 pagesDetermining Gravidity and Parity: I. GravidaDanica CorpuzNo ratings yet
- Text of Reproductive Rights Amendment For Ballot in November 2023Document1 pageText of Reproductive Rights Amendment For Ballot in November 2023Jo InglesNo ratings yet
- Challenges Faced by Pakistani Healthcare SystemDocument4 pagesChallenges Faced by Pakistani Healthcare SystemMustafa MahmoodNo ratings yet
- Daftar Pustaka - SalinDocument3 pagesDaftar Pustaka - SalinKikiNo ratings yet
- Family Welfare ServicesDocument47 pagesFamily Welfare ServicesAjay DNo ratings yet
- Barbara Katz Rothman-Childbirth-The Social Construction of BirthDocument10 pagesBarbara Katz Rothman-Childbirth-The Social Construction of Birthr3gister_400160006No ratings yet
- Obese ParturientDocument7 pagesObese Parturientbilly wilsonNo ratings yet
- SOSCG 6jul2013 v5Document32 pagesSOSCG 6jul2013 v5Suhazeli Abdullah100% (2)
- Mrs. Shwetha Rani C.MDocument38 pagesMrs. Shwetha Rani C.MSanthosh.S.UNo ratings yet
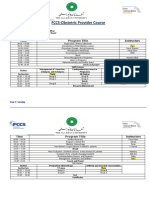
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- Recap Obstetrics Day 1 Post TestDocument1 pageRecap Obstetrics Day 1 Post TestJANEL BUENAVENTURANo ratings yet
- Final Update On Antenatal Steroids - DR PadmeshDocument66 pagesFinal Update On Antenatal Steroids - DR PadmeshAhalia NicuNo ratings yet
- Cmca Transes PrelimDocument33 pagesCmca Transes Prelimangelalorin.balano.cvt100% (1)
- Diagnosis Dini Preeklampsia Dan Eklampsia Dan Pencegahan Preeklampsia Dan EklampsiaDocument22 pagesDiagnosis Dini Preeklampsia Dan Eklampsia Dan Pencegahan Preeklampsia Dan EklampsiaAbigail Bl SiagianNo ratings yet
- Bemonc Capable Facility or ProviderDocument1 pageBemonc Capable Facility or ProviderAngelica AycardoNo ratings yet
- Fetal Death in Utero Radiology Reference Article PDFDocument1 pageFetal Death in Utero Radiology Reference Article PDFMoe Wai MyintNo ratings yet
- Placenta Previa (OB)Document4 pagesPlacenta Previa (OB)Winj BudayNo ratings yet