Download as pdf or txt
You might also like
- DigoxinDocument8 pagesDigoxinAnditapitalokaNo ratings yet
- IRF Quality Measures Users Manual V20Document114 pagesIRF Quality Measures Users Manual V20ngockihoangNo ratings yet
- Courier WedgeDocument19 pagesCourier WedgesurfnewmediaNo ratings yet
- Remote Patient Monitoring in Chronic Heart FailureDocument10 pagesRemote Patient Monitoring in Chronic Heart FailureTony TuestaNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- Nihms 271845Document17 pagesNihms 271845Andres Mauricio MuñozNo ratings yet
- 4Document10 pages4Destira Heffiyana3No ratings yet
- Ihj 53 11Document7 pagesIhj 53 11Ivan Lucas PiconeNo ratings yet
- Ewss PDFDocument6 pagesEwss PDFChintia Meliana Kathy SiraitNo ratings yet
- Peters 2017Document5 pagesPeters 2017Friska Permatasari NababanNo ratings yet
- Diagnostics: A Machine-Learning-Based Prediction Method For Hypertension Outcomes Based On Medical DataDocument21 pagesDiagnostics: A Machine-Learning-Based Prediction Method For Hypertension Outcomes Based On Medical DatafarzanaNo ratings yet
- Discharge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectDocument17 pagesDischarge Planning For Acute Coronary Syndrome Patients in A Tertiary Hospital: A Best Practice Implementation ProjectMukhlis HasNo ratings yet
- 1 s2.0 S2352906718301489 MainDocument5 pages1 s2.0 S2352906718301489 MainMinh Hai TranNo ratings yet
- CMRP0218Document14 pagesCMRP0218cherish60126No ratings yet
- Mobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournDocument7 pagesMobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournStefan LaurentiuNo ratings yet
- CC 11396Document12 pagesCC 11396Dhavala Shree B JainNo ratings yet
- International Journal of Cardiology: SciencedirectDocument6 pagesInternational Journal of Cardiology: SciencedirectRobsonBorgesNo ratings yet
- Ronald V. Maier, M.D.: Awards: FundingDocument5 pagesRonald V. Maier, M.D.: Awards: Fundingyanuar andaniNo ratings yet
- An Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialDocument7 pagesAn Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialcharmyshkuNo ratings yet
- Baugh Et Al-2017-Academic Emergency MedicineDocument9 pagesBaugh Et Al-2017-Academic Emergency MedicineRovanNo ratings yet
- International Journal of Medical Informatics: Zhe Wang, Lijuan Yao, Dongdong Li, Tong Ruan, Min Liu, Ju GaoDocument8 pagesInternational Journal of Medical Informatics: Zhe Wang, Lijuan Yao, Dongdong Li, Tong Ruan, Min Liu, Ju GaoMuzamilNo ratings yet
- ElevatedDocument12 pagesElevatedTimothy Eduard A. SupitNo ratings yet
- EPOC COPD Annals of Internal Medicine Article 2012Document18 pagesEPOC COPD Annals of Internal Medicine Article 2012Meléndez CarlosNo ratings yet
- Mobile Health Technology For Atrial Fibrillation Management Integrating Decision Support, Education, and Patient Involvement: mAF App TrialDocument15 pagesMobile Health Technology For Atrial Fibrillation Management Integrating Decision Support, Education, and Patient Involvement: mAF App TrialPsycolo techNo ratings yet
- End of Life Care For Lung CancerDocument7 pagesEnd of Life Care For Lung CancerPhilip R. MarallagNo ratings yet
- Heart FailureDocument7 pagesHeart FailureTiti SulistiowatiNo ratings yet
- OutDocument10 pagesOutErwinNo ratings yet
- The Complexity Score: Towards A Clinically-Relevant, Clinician-Friendly Measure of Patient Multi-MorbidityDocument6 pagesThe Complexity Score: Towards A Clinically-Relevant, Clinician-Friendly Measure of Patient Multi-MorbidityValtesondaSilvaNo ratings yet
- Academic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredDocument14 pagesAcademic Emergency Medicine - 2020 - Ebell - Accuracy of Signs and Symptoms For The Diagnosis of Community AcquiredOnilis RiveraNo ratings yet
- Early ViewDocument34 pagesEarly Viewyesid urregoNo ratings yet
- Blood PresureDocument8 pagesBlood Presurerisda aulia putriNo ratings yet
- NOAF en Paciente Critico RevisionDocument11 pagesNOAF en Paciente Critico RevisionARTURO YOSHIMAR LUQUE MAMANINo ratings yet
- ECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityDocument11 pagesECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityjuanpbagurNo ratings yet
- Multicentre Analysis CancerDocument8 pagesMulticentre Analysis Cancersilvio da costa guerreiroNo ratings yet
- Randomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureDocument7 pagesRandomized Trial of An Education and Support Intervention To Prevent Readmission of Patients With Heart FailureThyka MayasariNo ratings yet
- Benatar Outcomes of CHFDocument6 pagesBenatar Outcomes of CHFychow1No ratings yet
- Annals of General PsychiatryDocument9 pagesAnnals of General PsychiatryPutu Agus GrantikaNo ratings yet
- BMC Medical Research MethodologyDocument12 pagesBMC Medical Research MethodologyAngie OsorioNo ratings yet
- Antibiotics 02 00001Document10 pagesAntibiotics 02 00001Jenny AlmagroNo ratings yet
- Development of A Wearable Cardiac Monitoring System For Behavioral Neurocardiac Training: A Usability StudyDocument11 pagesDevelopment of A Wearable Cardiac Monitoring System For Behavioral Neurocardiac Training: A Usability StudyGabriella CsernákNo ratings yet
- ResearchDocument4 pagesResearchCarl Dela CruzNo ratings yet
- Puskarich 2014Document6 pagesPuskarich 2014Martha AcevesNo ratings yet
- Chan (2018)Document16 pagesChan (2018)Aprilla Ayu WulandariNo ratings yet
- Radiation Exposure and Cost Influence Physician Medical Image Decision MakingDocument5 pagesRadiation Exposure and Cost Influence Physician Medical Image Decision Makingكن صديقيNo ratings yet
- Makalah KesehatanDocument9 pagesMakalah KesehatanNini RahmiNo ratings yet
- Week2 Submitter PaperDocument3 pagesWeek2 Submitter Paperapi-299189797No ratings yet
- Biomarkers in Heart FailureDocument6 pagesBiomarkers in Heart Failurekevin ortegaNo ratings yet
- Tevis2018 Article Patient-ReportedOutcomesForBreDocument7 pagesTevis2018 Article Patient-ReportedOutcomesForBreGonzalo ZieglerNo ratings yet
- J Aem 2007 06 035Document8 pagesJ Aem 2007 06 035kingkinresmytaNo ratings yet
- Acad Emerg Med 2007 p1114Document6 pagesAcad Emerg Med 2007 p1114Handris SupriadiNo ratings yet
- JJJGJHGJHGHDocument6 pagesJJJGJHGJHGHTaufik NurohmanNo ratings yet
- Jcs 9 13Document7 pagesJcs 9 13kampret berbagiNo ratings yet
- ArticleDocument11 pagesArticlejesica_loNo ratings yet
- Critical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020Document13 pagesCritical Care After Major Surgery A Systematic Review of Risk Factors Unplanned Admission - Onwochei UK 2020Fransisca Dewi KumalaNo ratings yet
- Management of High Blood Pressure in Morocco:what Place For RGMPS ?Document9 pagesManagement of High Blood Pressure in Morocco:what Place For RGMPS ?IJAR JOURNALNo ratings yet
- Journal Review Final PaperDocument10 pagesJournal Review Final Paperapi-464793486No ratings yet
- A High-Volume Specialist Palliative Care Unit and Team May Reduce In-Hospital End-of-Life Care CostsDocument8 pagesA High-Volume Specialist Palliative Care Unit and Team May Reduce In-Hospital End-of-Life Care CostsNurbaiti Indah LestariNo ratings yet
- 2 General Principles of Research Design and AnalysisDocument6 pages2 General Principles of Research Design and AnalysisMohamed Elprince AdelNo ratings yet
- Systems-Basedpracticein Burncare: Prevention, Management, and Economic Impact of Health Care-Associated InfectionsDocument8 pagesSystems-Basedpracticein Burncare: Prevention, Management, and Economic Impact of Health Care-Associated InfectionsanjarwatiNo ratings yet
- An Early Warning System Improves Patient Safety and Clinical Outcomes in A Community Academic HospitalDocument9 pagesAn Early Warning System Improves Patient Safety and Clinical Outcomes in A Community Academic HospitalAnasthasia hutagalungNo ratings yet
- Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsDocument10 pagesMedication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsmadhurocksktmNo ratings yet
- MBC Significantly-Longer-Time-To-Deterioration-Of-QualDocument10 pagesMBC Significantly-Longer-Time-To-Deterioration-Of-QualAhmad Azhar Ab HamidNo ratings yet
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- 2018 Syllabus 8th SEMDocument40 pages2018 Syllabus 8th SEM18ME045No ratings yet
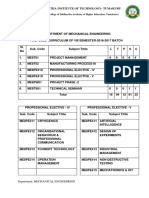
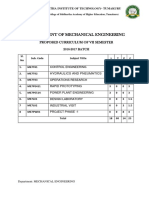
- 2018 Syllabus 7th SEMDocument25 pages2018 Syllabus 7th SEM18ME045No ratings yet
- Journal Pre-Proof: Journal of Cardiac FailureDocument72 pagesJournal Pre-Proof: Journal of Cardiac Failure18ME045No ratings yet
- Sri Siddhartha Institute of Technology, Tumkur Department of Electrical and Electronics EngineeringDocument3 pagesSri Siddhartha Institute of Technology, Tumkur Department of Electrical and Electronics Engineering18ME045No ratings yet
- OPPE Indicator List by DeparDocument11 pagesOPPE Indicator List by DeparYandiNo ratings yet
- Productivity: Prof. Christian TerwieschDocument46 pagesProductivity: Prof. Christian TerwieschSabila SanjraniNo ratings yet
- IDEAL Discharge Planning Overview, Process, and ChecklistDocument8 pagesIDEAL Discharge Planning Overview, Process, and Checklistrisa agustinaNo ratings yet
- A Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Document8 pagesA Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Eric KatškovskiNo ratings yet
- Reiss Sandborn 2015 Role of Psychosocial CareDocument6 pagesReiss Sandborn 2015 Role of Psychosocial CareAgata AgniNo ratings yet
- Advisory Board Womens Health Strategic Plan TemplateFinal MPLCDocument63 pagesAdvisory Board Womens Health Strategic Plan TemplateFinal MPLCKang DjoenNo ratings yet
- Physician Scorecards: Clinical Documentation and Coding ImprovementDocument5 pagesPhysician Scorecards: Clinical Documentation and Coding ImprovementBayu SaputeraNo ratings yet
- PH Orthooutcomesreport 0904 Final SampleDocument15 pagesPH Orthooutcomesreport 0904 Final Sampleapi-550152465No ratings yet
- Hpia & Specific Indicators Tech Spec 2022Document65 pagesHpia & Specific Indicators Tech Spec 2022Aslam AssandakaniNo ratings yet
- STRONG-HF TrialDocument16 pagesSTRONG-HF TrialyukeNo ratings yet
- Chapter 36 & 37 - Desiderio, Gomez, Limcangco (BSN2B)Document22 pagesChapter 36 & 37 - Desiderio, Gomez, Limcangco (BSN2B)Anji LimcangcoNo ratings yet
- Improving Quality and Productivity in Healthcare: White Paper - 2015Document8 pagesImproving Quality and Productivity in Healthcare: White Paper - 2015ismail taiwoNo ratings yet
- International Journal of Cardiology: SciencedirectDocument6 pagesInternational Journal of Cardiology: SciencedirectRobsonBorgesNo ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- Pennsylvania Health Care PerformanceDocument7 pagesPennsylvania Health Care PerformanceWHYY NewsNo ratings yet
- Quality Indicators & Safety PresentationDocument63 pagesQuality Indicators & Safety Presentationapi-28181342267% (3)
- Predicting Readmission of Diabetic Patients High PerformanceDocument10 pagesPredicting Readmission of Diabetic Patients High PerformancepedrofwNo ratings yet
- 5 Quality Measures That Matter For Value-Based CareDocument8 pages5 Quality Measures That Matter For Value-Based CareTuan Nguyen DangNo ratings yet
- Silow Carroll - Hosp - Quality - Improve - Strategies - Lessons - 1009 PDFDocument70 pagesSilow Carroll - Hosp - Quality - Improve - Strategies - Lessons - 1009 PDFSebrindaa GinaNo ratings yet
- Innovation in Health Care Delivery: Jonathan Wilt AVP, Center For Innovation Ochsner Health SystemDocument47 pagesInnovation in Health Care Delivery: Jonathan Wilt AVP, Center For Innovation Ochsner Health SystemMedika UtamaNo ratings yet
- Against Medical Advice Discharges: Choosing WiselyDocument3 pagesAgainst Medical Advice Discharges: Choosing WiselyAnj RodriguezNo ratings yet
- Aiken 2020Document9 pagesAiken 2020Cristhian LopezNo ratings yet
- A Practical Guide To Healthcare DataDocument20 pagesA Practical Guide To Healthcare DataGeorge Tanaruno100% (1)
- Burden of Surgical Site Infections in The NetherlandsDocument10 pagesBurden of Surgical Site Infections in The NetherlandsKanokwan BorwornphiphattanachaiNo ratings yet
- SB 530 531Document10 pagesSB 530 531WWMTNo ratings yet
- ClinicalbertDocument9 pagesClinicalbertZhiyuan LNo ratings yet
- Changing Practice PowerpointDocument18 pagesChanging Practice PowerpointSarah BayouthNo ratings yet