
Group 8 Case Study
Group 8 Case Study
You might also like
- Case Presentation On Urinary Tract InfectionDocument56 pagesCase Presentation On Urinary Tract InfectionJohn Alvin Yoro92% (24)
- Case Study On CVADocument34 pagesCase Study On CVAGimcy Dela Fuente50% (2)
- CarQuest Wearever Brake Parts Cleaner WES W5089 PDFDocument1 pageCarQuest Wearever Brake Parts Cleaner WES W5089 PDFYoutube For EducationNo ratings yet
- Cambridge IGCSE: 0500/12 First Language EnglishDocument16 pagesCambridge IGCSE: 0500/12 First Language EnglishOM WARENo ratings yet
- Case StudyDocument28 pagesCase Studyakoeljames8543No ratings yet
- Endocrinology Clinical Case Write-UpDocument5 pagesEndocrinology Clinical Case Write-UpNoelle Jiyana SingsonNo ratings yet
- Takayasu'S Arteritis: A Case StudyDocument42 pagesTakayasu'S Arteritis: A Case StudyErnesto Trinidad Jr RNNo ratings yet
- Lumbar Compression FractureDocument47 pagesLumbar Compression FractureAngelie Sanchez50% (2)
- GoutDocument75 pagesGoutVan Talawec100% (2)
- Ortho Week 1Document24 pagesOrtho Week 1Jamie John EsplanadaNo ratings yet
- CaseStudyTuberculosis Quindala TanoDocument102 pagesCaseStudyTuberculosis Quindala TanoLiz G. QuindalaNo ratings yet
- Case Analysis ON Cholelithiasis S/P CholecystectomyDocument18 pagesCase Analysis ON Cholelithiasis S/P CholecystectomyAllyssa AnastacioNo ratings yet
- Complete Cholelithiasis Case AnalysisDocument18 pagesComplete Cholelithiasis Case AnalysisAllyssa AnastacioNo ratings yet
- Case Analysis ON Cholelithiasis S/P CholecystectomyDocument18 pagesCase Analysis ON Cholelithiasis S/P CholecystectomyAllyssa AnastacioNo ratings yet
- Lumbar Compression Fracture: A Case StudyDocument46 pagesLumbar Compression Fracture: A Case StudyOlivia SolomonNo ratings yet
- OsteosarcomaDocument87 pagesOsteosarcomaCob CornNo ratings yet
- FT - 116 A1 - Clinicals-Week 12 - Gen Task 1Document79 pagesFT - 116 A1 - Clinicals-Week 12 - Gen Task 1Megan BarreraNo ratings yet
- CHOLECYSTOLITHIASISDocument77 pagesCHOLECYSTOLITHIASISMarkie ArqueroNo ratings yet
- Myoma Final Power PointDocument45 pagesMyoma Final Power Pointicesexy100% (1)
- College of Nursing Ozamiz City: La Salle UniversityDocument4 pagesCollege of Nursing Ozamiz City: La Salle UniversityJb RosillosaNo ratings yet
- Lourdes College College of Nursing Capistrano Street, Cagayan de Oro CityDocument21 pagesLourdes College College of Nursing Capistrano Street, Cagayan de Oro Cityapplecringe100% (1)
- KEL 1-KASUS OSTEPOROSIS DAN KONTRASEPSI-S1 - 5a-DikonversiDocument31 pagesKEL 1-KASUS OSTEPOROSIS DAN KONTRASEPSI-S1 - 5a-DikonversiNadarahmatulNo ratings yet
- Case StudyDocument20 pagesCase StudyMae Alexes TamañoNo ratings yet
- Reza Well Elder 3.0Document11 pagesReza Well Elder 3.0Alireza ParishaniNo ratings yet
- 2014 Cellular Healing Diet EbookDocument42 pages2014 Cellular Healing Diet Ebookdenis75% (4)
- A Victim No More: Overcoming Irritable Bowel Syndrome: Safe, Effective Therapies for Relief from Bowel ComplaintsFrom EverandA Victim No More: Overcoming Irritable Bowel Syndrome: Safe, Effective Therapies for Relief from Bowel ComplaintsNo ratings yet
- UY - Final CHN StudyDocument32 pagesUY - Final CHN StudyKim TangoNo ratings yet
- Comprehensive Health History Output: Sam Albert J. RenaciaDocument7 pagesComprehensive Health History Output: Sam Albert J. RenaciaSam Albert RenaciaNo ratings yet
- Pattern Before Present Interpretation AnalysisDocument8 pagesPattern Before Present Interpretation AnalysisJorelyn FriasNo ratings yet
- Typhoid FeverDocument38 pagesTyphoid Fevermhamaenphapa27No ratings yet
- Cholelithiasis Case PresentationDocument25 pagesCholelithiasis Case PresentationMarcos AquinoNo ratings yet
- Gordon's AssessmentDocument3 pagesGordon's AssessmentAzy Joy ViñasNo ratings yet
- Dengue Fever Case Pre WordDocument26 pagesDengue Fever Case Pre WordBjörn DaamoNo ratings yet
- Chief ComplaintDocument4 pagesChief ComplaintJen GatchalianNo ratings yet
- Group 3 Presents: AspergillomaDocument70 pagesGroup 3 Presents: AspergillomaGilian DacanayNo ratings yet
- Irene's Care StudyDocument68 pagesIrene's Care StudyLawrence AckahNo ratings yet
- Chronic Kidney DiseaseDocument50 pagesChronic Kidney Diseasejuvylynuy06No ratings yet
- Role-Taking 223143219 Lenient Anele NkalaDocument8 pagesRole-Taking 223143219 Lenient Anele NkalaAnele NkalaNo ratings yet
- Patient Health HistoryDocument8 pagesPatient Health HistoryRafi LabNo ratings yet
- Most Memorable Patient ArticleDocument2 pagesMost Memorable Patient ArticleVirginia Savely DNPNo ratings yet
- At The DOCTOR Dialogues and Vocabulary ListDocument12 pagesAt The DOCTOR Dialogues and Vocabulary ListMax Tapia CastilloNo ratings yet
- Case Study 150908172854 Lva1 App6891Document18 pagesCase Study 150908172854 Lva1 App6891RENEROSE TORRESNo ratings yet
- HEALTH HISTORY WPS Office - Docx 1Document7 pagesHEALTH HISTORY WPS Office - Docx 1Cy PilapilNo ratings yet
- E-Folio IDocument8 pagesE-Folio Iapi-318152697No ratings yet
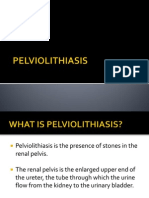
- PELVIOLITHIASISDocument45 pagesPELVIOLITHIASISAriane VidalNo ratings yet
- One Step Ahead of Osteoarthritis: Stay Flexible and Keep MovingFrom EverandOne Step Ahead of Osteoarthritis: Stay Flexible and Keep MovingNo ratings yet
- Case Presentation Cornelio SumbadDocument33 pagesCase Presentation Cornelio SumbadCheer May Cabason De GraciaNo ratings yet
- DM Case PresDocument23 pagesDM Case PresZent AquinoNo ratings yet
- Case Study Activity 1-4Document7 pagesCase Study Activity 1-4kuma phNo ratings yet
- Dieta Anti Inflamatoria PDFDocument43 pagesDieta Anti Inflamatoria PDFTimóteo100% (1)
- NP Colon Cancer by 13-2Document9 pagesNP Colon Cancer by 13-2Melody Medina100% (1)
- NCP - DM, CKD, HPNDocument5 pagesNCP - DM, CKD, HPNMargueretti Delos ReyesNo ratings yet
- Critical ThinkingDocument3 pagesCritical ThinkingJuliezel IringanNo ratings yet
- Severe Pre EclampsiaDocument110 pagesSevere Pre EclampsiaJachel Kathleen LaguioNo ratings yet
- Gordon's Functional Assessment HistoryDocument5 pagesGordon's Functional Assessment HistoryJachel Kathleen Laguio100% (1)
- Cerebrovascular Disease (Bleed)Document25 pagesCerebrovascular Disease (Bleed)Margaret Jenaw JenawNo ratings yet
- Case Study Uro FinalDocument44 pagesCase Study Uro FinalDan Ataniel EnsaladaNo ratings yet
- Community Acquired Pneumonia (CAP)Document48 pagesCommunity Acquired Pneumonia (CAP)lei2x100% (1)
- A Whole-Body Approach to Slowing Down Aging: Helping You Live Healthier and LongerFrom EverandA Whole-Body Approach to Slowing Down Aging: Helping You Live Healthier and LongerNo ratings yet
- Case Pres Cerebrovascular DiseaseDocument34 pagesCase Pres Cerebrovascular DiseaseADRIATICO JAROSLUVNo ratings yet
- Family Homeostasis and The Physician 1965Document4 pagesFamily Homeostasis and The Physician 1965Luis BernardoNo ratings yet
- FAQ Regarding FacemasksDocument5 pagesFAQ Regarding FacemasksDanaNo ratings yet
- World Kidney Program 2022: ProspectusDocument3 pagesWorld Kidney Program 2022: ProspectusNuranisaNo ratings yet
- PEDSQLDocument4 pagesPEDSQLAmaranto100% (1)
- Literature Review On Dental CalculusDocument7 pagesLiterature Review On Dental Calculuszyfepyfej0p2100% (1)
- Pterygopalatine and Otic GanglionDocument54 pagesPterygopalatine and Otic GanglionAKSHRAA K VNo ratings yet
- Stok Opname 2020Document63 pagesStok Opname 2020Hafizh JhunkoNo ratings yet
- 2.1. Miêu Tả Và So Sánh Số LiệuDocument13 pages2.1. Miêu Tả Và So Sánh Số Liệuthvl3105No ratings yet
- Economically DisadvantagedDocument7 pagesEconomically DisadvantagedAhm SamNo ratings yet
- Thesis Taekwondo Black BeltDocument5 pagesThesis Taekwondo Black Beltgbx272pg100% (1)
- Positive Guidance TechniquesDocument5 pagesPositive Guidance TechniquesChrismoonNo ratings yet
- ATEC Console Operators Manual (MAN-03327) Rev 005 7 - 2017Document36 pagesATEC Console Operators Manual (MAN-03327) Rev 005 7 - 2017colladoluzangelaNo ratings yet
- College of Arts & Sciences: Google Meet Link - 1 Semester AY 2022-2023Document2 pagesCollege of Arts & Sciences: Google Meet Link - 1 Semester AY 2022-2023TrixieNo ratings yet
- PHC-1 Mid Term Exam-Final Questions With Answers-2023Document4 pagesPHC-1 Mid Term Exam-Final Questions With Answers-2023Galakpai KolubahNo ratings yet
- Brigada Eskwela 2021 (Immersion)Document61 pagesBrigada Eskwela 2021 (Immersion)APRIL MULANo ratings yet
- g9 Thi TH GVTV 2021-004 WordDocument3 pagesg9 Thi TH GVTV 2021-004 WordAnh ThuNo ratings yet
- Siasatan Kes Ibu Hamil Hiv PositifDocument12 pagesSiasatan Kes Ibu Hamil Hiv PositifPooneethawathi SantranNo ratings yet
- A Conceptual Model and Framework Of.7Document7 pagesA Conceptual Model and Framework Of.7ariniNo ratings yet
- A Seminar Report (BCH 418) : Biochemistry ProgrammeDocument69 pagesA Seminar Report (BCH 418) : Biochemistry ProgrammeMamatha RahulNo ratings yet
- Hematology Sop (Revise 2023)Document8 pagesHematology Sop (Revise 2023)Jeffrey GaliciaNo ratings yet
- Abnormal Psyc Session 1 SlidesDocument70 pagesAbnormal Psyc Session 1 SlidesDaniel Naawenkangua AbukuriNo ratings yet
- Nurse Job Interview Questions About Rude DoctorsDocument1 pageNurse Job Interview Questions About Rude DoctorsDnr PhsNo ratings yet
- Magsaysay Marine Inc. V, Michael Atraje, July 23, 2018Document2 pagesMagsaysay Marine Inc. V, Michael Atraje, July 23, 2018Russ TuazonNo ratings yet
- kg10 DescaleDocument8 pageskg10 DescaleMohammed SamyNo ratings yet
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
- Unit 6 Growth and Development and Care of The AdolescentDocument17 pagesUnit 6 Growth and Development and Care of The AdolescentKyla CapituloNo ratings yet
- Evaluation of Artocarus Odoratissimus (Marang) Seeds As An Alternative Source or Low-Gluten FlourDocument8 pagesEvaluation of Artocarus Odoratissimus (Marang) Seeds As An Alternative Source or Low-Gluten FlourCatherine Joy MenesNo ratings yet
- Energetic Kinesiology24Document1 pageEnergetic Kinesiology24Marius Dan GiolgauNo ratings yet
























































































Download as pdf or txt
You might also like
- Case Presentation On Urinary Tract InfectionDocument56 pagesCase Presentation On Urinary Tract InfectionJohn Alvin Yoro92% (24)
- Case Study On CVADocument34 pagesCase Study On CVAGimcy Dela Fuente50% (2)
- CarQuest Wearever Brake Parts Cleaner WES W5089 PDFDocument1 pageCarQuest Wearever Brake Parts Cleaner WES W5089 PDFYoutube For EducationNo ratings yet
- Cambridge IGCSE: 0500/12 First Language EnglishDocument16 pagesCambridge IGCSE: 0500/12 First Language EnglishOM WARENo ratings yet
- Case StudyDocument28 pagesCase Studyakoeljames8543No ratings yet
- Endocrinology Clinical Case Write-UpDocument5 pagesEndocrinology Clinical Case Write-UpNoelle Jiyana SingsonNo ratings yet
- Takayasu'S Arteritis: A Case StudyDocument42 pagesTakayasu'S Arteritis: A Case StudyErnesto Trinidad Jr RNNo ratings yet
- Lumbar Compression FractureDocument47 pagesLumbar Compression FractureAngelie Sanchez50% (2)
- GoutDocument75 pagesGoutVan Talawec100% (2)
- Ortho Week 1Document24 pagesOrtho Week 1Jamie John EsplanadaNo ratings yet
- CaseStudyTuberculosis Quindala TanoDocument102 pagesCaseStudyTuberculosis Quindala TanoLiz G. QuindalaNo ratings yet
- Case Analysis ON Cholelithiasis S/P CholecystectomyDocument18 pagesCase Analysis ON Cholelithiasis S/P CholecystectomyAllyssa AnastacioNo ratings yet
- Complete Cholelithiasis Case AnalysisDocument18 pagesComplete Cholelithiasis Case AnalysisAllyssa AnastacioNo ratings yet
- Case Analysis ON Cholelithiasis S/P CholecystectomyDocument18 pagesCase Analysis ON Cholelithiasis S/P CholecystectomyAllyssa AnastacioNo ratings yet
- Lumbar Compression Fracture: A Case StudyDocument46 pagesLumbar Compression Fracture: A Case StudyOlivia SolomonNo ratings yet
- OsteosarcomaDocument87 pagesOsteosarcomaCob CornNo ratings yet
- FT - 116 A1 - Clinicals-Week 12 - Gen Task 1Document79 pagesFT - 116 A1 - Clinicals-Week 12 - Gen Task 1Megan BarreraNo ratings yet
- CHOLECYSTOLITHIASISDocument77 pagesCHOLECYSTOLITHIASISMarkie ArqueroNo ratings yet
- Myoma Final Power PointDocument45 pagesMyoma Final Power Pointicesexy100% (1)
- College of Nursing Ozamiz City: La Salle UniversityDocument4 pagesCollege of Nursing Ozamiz City: La Salle UniversityJb RosillosaNo ratings yet
- Lourdes College College of Nursing Capistrano Street, Cagayan de Oro CityDocument21 pagesLourdes College College of Nursing Capistrano Street, Cagayan de Oro Cityapplecringe100% (1)
- KEL 1-KASUS OSTEPOROSIS DAN KONTRASEPSI-S1 - 5a-DikonversiDocument31 pagesKEL 1-KASUS OSTEPOROSIS DAN KONTRASEPSI-S1 - 5a-DikonversiNadarahmatulNo ratings yet
- Case StudyDocument20 pagesCase StudyMae Alexes TamañoNo ratings yet
- Reza Well Elder 3.0Document11 pagesReza Well Elder 3.0Alireza ParishaniNo ratings yet
- 2014 Cellular Healing Diet EbookDocument42 pages2014 Cellular Healing Diet Ebookdenis75% (4)
- A Victim No More: Overcoming Irritable Bowel Syndrome: Safe, Effective Therapies for Relief from Bowel ComplaintsFrom EverandA Victim No More: Overcoming Irritable Bowel Syndrome: Safe, Effective Therapies for Relief from Bowel ComplaintsNo ratings yet
- UY - Final CHN StudyDocument32 pagesUY - Final CHN StudyKim TangoNo ratings yet
- Comprehensive Health History Output: Sam Albert J. RenaciaDocument7 pagesComprehensive Health History Output: Sam Albert J. RenaciaSam Albert RenaciaNo ratings yet
- Pattern Before Present Interpretation AnalysisDocument8 pagesPattern Before Present Interpretation AnalysisJorelyn FriasNo ratings yet
- Typhoid FeverDocument38 pagesTyphoid Fevermhamaenphapa27No ratings yet
- Cholelithiasis Case PresentationDocument25 pagesCholelithiasis Case PresentationMarcos AquinoNo ratings yet
- Gordon's AssessmentDocument3 pagesGordon's AssessmentAzy Joy ViñasNo ratings yet
- Dengue Fever Case Pre WordDocument26 pagesDengue Fever Case Pre WordBjörn DaamoNo ratings yet
- Chief ComplaintDocument4 pagesChief ComplaintJen GatchalianNo ratings yet
- Group 3 Presents: AspergillomaDocument70 pagesGroup 3 Presents: AspergillomaGilian DacanayNo ratings yet
- Irene's Care StudyDocument68 pagesIrene's Care StudyLawrence AckahNo ratings yet
- Chronic Kidney DiseaseDocument50 pagesChronic Kidney Diseasejuvylynuy06No ratings yet
- Role-Taking 223143219 Lenient Anele NkalaDocument8 pagesRole-Taking 223143219 Lenient Anele NkalaAnele NkalaNo ratings yet
- Patient Health HistoryDocument8 pagesPatient Health HistoryRafi LabNo ratings yet
- Most Memorable Patient ArticleDocument2 pagesMost Memorable Patient ArticleVirginia Savely DNPNo ratings yet
- At The DOCTOR Dialogues and Vocabulary ListDocument12 pagesAt The DOCTOR Dialogues and Vocabulary ListMax Tapia CastilloNo ratings yet
- Case Study 150908172854 Lva1 App6891Document18 pagesCase Study 150908172854 Lva1 App6891RENEROSE TORRESNo ratings yet
- HEALTH HISTORY WPS Office - Docx 1Document7 pagesHEALTH HISTORY WPS Office - Docx 1Cy PilapilNo ratings yet
- E-Folio IDocument8 pagesE-Folio Iapi-318152697No ratings yet
- PELVIOLITHIASISDocument45 pagesPELVIOLITHIASISAriane VidalNo ratings yet
- One Step Ahead of Osteoarthritis: Stay Flexible and Keep MovingFrom EverandOne Step Ahead of Osteoarthritis: Stay Flexible and Keep MovingNo ratings yet
- Case Presentation Cornelio SumbadDocument33 pagesCase Presentation Cornelio SumbadCheer May Cabason De GraciaNo ratings yet
- DM Case PresDocument23 pagesDM Case PresZent AquinoNo ratings yet
- Case Study Activity 1-4Document7 pagesCase Study Activity 1-4kuma phNo ratings yet
- Dieta Anti Inflamatoria PDFDocument43 pagesDieta Anti Inflamatoria PDFTimóteo100% (1)
- NP Colon Cancer by 13-2Document9 pagesNP Colon Cancer by 13-2Melody Medina100% (1)
- NCP - DM, CKD, HPNDocument5 pagesNCP - DM, CKD, HPNMargueretti Delos ReyesNo ratings yet
- Critical ThinkingDocument3 pagesCritical ThinkingJuliezel IringanNo ratings yet
- Severe Pre EclampsiaDocument110 pagesSevere Pre EclampsiaJachel Kathleen LaguioNo ratings yet
- Gordon's Functional Assessment HistoryDocument5 pagesGordon's Functional Assessment HistoryJachel Kathleen Laguio100% (1)
- Cerebrovascular Disease (Bleed)Document25 pagesCerebrovascular Disease (Bleed)Margaret Jenaw JenawNo ratings yet
- Case Study Uro FinalDocument44 pagesCase Study Uro FinalDan Ataniel EnsaladaNo ratings yet
- Community Acquired Pneumonia (CAP)Document48 pagesCommunity Acquired Pneumonia (CAP)lei2x100% (1)
- A Whole-Body Approach to Slowing Down Aging: Helping You Live Healthier and LongerFrom EverandA Whole-Body Approach to Slowing Down Aging: Helping You Live Healthier and LongerNo ratings yet
- Case Pres Cerebrovascular DiseaseDocument34 pagesCase Pres Cerebrovascular DiseaseADRIATICO JAROSLUVNo ratings yet
- Family Homeostasis and The Physician 1965Document4 pagesFamily Homeostasis and The Physician 1965Luis BernardoNo ratings yet
- FAQ Regarding FacemasksDocument5 pagesFAQ Regarding FacemasksDanaNo ratings yet
- World Kidney Program 2022: ProspectusDocument3 pagesWorld Kidney Program 2022: ProspectusNuranisaNo ratings yet
- PEDSQLDocument4 pagesPEDSQLAmaranto100% (1)
- Literature Review On Dental CalculusDocument7 pagesLiterature Review On Dental Calculuszyfepyfej0p2100% (1)
- Pterygopalatine and Otic GanglionDocument54 pagesPterygopalatine and Otic GanglionAKSHRAA K VNo ratings yet
- Stok Opname 2020Document63 pagesStok Opname 2020Hafizh JhunkoNo ratings yet
- 2.1. Miêu Tả Và So Sánh Số LiệuDocument13 pages2.1. Miêu Tả Và So Sánh Số Liệuthvl3105No ratings yet
- Economically DisadvantagedDocument7 pagesEconomically DisadvantagedAhm SamNo ratings yet
- Thesis Taekwondo Black BeltDocument5 pagesThesis Taekwondo Black Beltgbx272pg100% (1)
- Positive Guidance TechniquesDocument5 pagesPositive Guidance TechniquesChrismoonNo ratings yet
- ATEC Console Operators Manual (MAN-03327) Rev 005 7 - 2017Document36 pagesATEC Console Operators Manual (MAN-03327) Rev 005 7 - 2017colladoluzangelaNo ratings yet
- College of Arts & Sciences: Google Meet Link - 1 Semester AY 2022-2023Document2 pagesCollege of Arts & Sciences: Google Meet Link - 1 Semester AY 2022-2023TrixieNo ratings yet
- PHC-1 Mid Term Exam-Final Questions With Answers-2023Document4 pagesPHC-1 Mid Term Exam-Final Questions With Answers-2023Galakpai KolubahNo ratings yet
- Brigada Eskwela 2021 (Immersion)Document61 pagesBrigada Eskwela 2021 (Immersion)APRIL MULANo ratings yet
- g9 Thi TH GVTV 2021-004 WordDocument3 pagesg9 Thi TH GVTV 2021-004 WordAnh ThuNo ratings yet
- Siasatan Kes Ibu Hamil Hiv PositifDocument12 pagesSiasatan Kes Ibu Hamil Hiv PositifPooneethawathi SantranNo ratings yet
- A Conceptual Model and Framework Of.7Document7 pagesA Conceptual Model and Framework Of.7ariniNo ratings yet
- A Seminar Report (BCH 418) : Biochemistry ProgrammeDocument69 pagesA Seminar Report (BCH 418) : Biochemistry ProgrammeMamatha RahulNo ratings yet
- Hematology Sop (Revise 2023)Document8 pagesHematology Sop (Revise 2023)Jeffrey GaliciaNo ratings yet
- Abnormal Psyc Session 1 SlidesDocument70 pagesAbnormal Psyc Session 1 SlidesDaniel Naawenkangua AbukuriNo ratings yet
- Nurse Job Interview Questions About Rude DoctorsDocument1 pageNurse Job Interview Questions About Rude DoctorsDnr PhsNo ratings yet
- Magsaysay Marine Inc. V, Michael Atraje, July 23, 2018Document2 pagesMagsaysay Marine Inc. V, Michael Atraje, July 23, 2018Russ TuazonNo ratings yet
- kg10 DescaleDocument8 pageskg10 DescaleMohammed SamyNo ratings yet
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
- Unit 6 Growth and Development and Care of The AdolescentDocument17 pagesUnit 6 Growth and Development and Care of The AdolescentKyla CapituloNo ratings yet
- Evaluation of Artocarus Odoratissimus (Marang) Seeds As An Alternative Source or Low-Gluten FlourDocument8 pagesEvaluation of Artocarus Odoratissimus (Marang) Seeds As An Alternative Source or Low-Gluten FlourCatherine Joy MenesNo ratings yet
- Energetic Kinesiology24Document1 pageEnergetic Kinesiology24Marius Dan GiolgauNo ratings yet