Download as pdf or txt
You might also like
- Management of Preterm LaborDocument2 pagesManagement of Preterm LaborpolygoneNo ratings yet
- Quality Control Tests For CapsulesDocument11 pagesQuality Control Tests For CapsulesM Afan100% (3)
- FDA Pregnancy CategoriesDocument3 pagesFDA Pregnancy CategoriesAnggaNo ratings yet
- Psychotropic Medications During PregnancyDocument20 pagesPsychotropic Medications During PregnancyMaria Von ShaftNo ratings yet
- Drugs For The Geriatric PatientDocument1,413 pagesDrugs For The Geriatric Patientjulio.testi698295100% (1)
- The New Pregnancy and Lactation Labeling RuleDocument3 pagesThe New Pregnancy and Lactation Labeling RuleVijendra RNo ratings yet
- Editorials: FDA Implements New Labeling For Medications Used During Pregnancy and LactationDocument2 pagesEditorials: FDA Implements New Labeling For Medications Used During Pregnancy and LactationRaul DoctoNo ratings yet
- Drugs in Pregnancy and Lactation: Improved Benefit-Risk InformationDocument2 pagesDrugs in Pregnancy and Lactation: Improved Benefit-Risk InformationYunan Syahban MaskatNo ratings yet
- Pregnant and Breastfeeding Women: ©ICAP/Sven TorfinnDocument16 pagesPregnant and Breastfeeding Women: ©ICAP/Sven TorfinnMarc FresNo ratings yet
- Medication Safety During Pregnancy: Improving Evidence-Based PracticeDocument16 pagesMedication Safety During Pregnancy: Improving Evidence-Based PracticeANGELNo ratings yet
- Anatomical and Physiological Alterations of PregnancyDocument15 pagesAnatomical and Physiological Alterations of PregnancyMateo BermeoNo ratings yet
- Medications in Pregnancy 2Document16 pagesMedications in Pregnancy 2Franklin GarzaNo ratings yet
- 02 Pharmacotherapy in Pregnancy and LactationDocument10 pages02 Pharmacotherapy in Pregnancy and LactationAlejandra RequesensNo ratings yet
- 17-Evaluation of The Safety of Drugs WorkshopDocument9 pages17-Evaluation of The Safety of Drugs WorkshopsasNo ratings yet
- Review MEC 2016Document7 pagesReview MEC 2016Leydi Laura QuirozNo ratings yet
- Medications and Pregnancy The Role of Community PHDocument15 pagesMedications and Pregnancy The Role of Community PHJaikapil KachhawaNo ratings yet
- Amer Peds Recomm Re Psy Drugs and PregnancyDocument10 pagesAmer Peds Recomm Re Psy Drugs and Pregnancyscribd4kmhNo ratings yet
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiNo ratings yet
- New Changes in Pregnancy and Lactation Labelling RDocument11 pagesNew Changes in Pregnancy and Lactation Labelling RraidasilvabrNo ratings yet
- Farmacologia en El EmbrazoDocument12 pagesFarmacologia en El EmbrazoAlejandra Soledad Alvarado NeiraNo ratings yet
- 458 Galley 628 1 10 20171106Document7 pages458 Galley 628 1 10 20171106Evelyn LimNo ratings yet
- J 1744-4667 2012 00096 x@10 1002 - (ISSN) 1744-4667 (CAT) Subspecialities (VI) PerinatalMedicine2015 PDFDocument6 pagesJ 1744-4667 2012 00096 x@10 1002 - (ISSN) 1744-4667 (CAT) Subspecialities (VI) PerinatalMedicine2015 PDFDrAnisha PatelNo ratings yet
- Obat Pada Kehamilan Dan LaktasiDocument11 pagesObat Pada Kehamilan Dan LaktasiChristian RobbyNo ratings yet
- Pregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Document14 pagesPregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Sam YousryNo ratings yet
- DIsease, Compli, and DT in Obstetrics PDFDocument549 pagesDIsease, Compli, and DT in Obstetrics PDFKiki Afifana100% (2)
- Medical Management of Prgenancy LossDocument11 pagesMedical Management of Prgenancy LossAnonymous l6Q1ROq2No ratings yet
- Pregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeDocument14 pagesPregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeIslam FathiNo ratings yet
- Fda PDFDocument40 pagesFda PDFMarhama MagarangNo ratings yet
- Pi Is 0002937813005139Document5 pagesPi Is 0002937813005139fenskaNo ratings yet
- Basic Obstetric PharmacologyDocument24 pagesBasic Obstetric PharmacologyjokosudibyoNo ratings yet
- Pharmacology and Pharmacogenomics of Neurological Medications Used in Pregnancy 2013Document12 pagesPharmacology and Pharmacogenomics of Neurological Medications Used in Pregnancy 2013Ricardo Robles AlfaroNo ratings yet
- Clinical Assessment of Fetal Well-Being and FetalDocument12 pagesClinical Assessment of Fetal Well-Being and Fetalhenri kaneNo ratings yet
- Competency Assessment Module - Obstetric CareDocument17 pagesCompetency Assessment Module - Obstetric CareJeremy HamptonNo ratings yet
- Medication Use During Pregnancy, With Particular Focus On Prescription Drugs: 1976-2008Document8 pagesMedication Use During Pregnancy, With Particular Focus On Prescription Drugs: 1976-2008MARIA KARINA HERNANDEZ PEREZNo ratings yet
- Labio y Paladar Hendido 1Document8 pagesLabio y Paladar Hendido 1Karina HernandezNo ratings yet
- FDA Pregnancy Rules (Updated) (Medex - Com.bd)Document3 pagesFDA Pregnancy Rules (Updated) (Medex - Com.bd)darikaribeiroNo ratings yet
- Risco Potencial Do Uso de Medicamentos Durante A Gravidez e A LactaçãoDocument6 pagesRisco Potencial Do Uso de Medicamentos Durante A Gravidez e A LactaçãoAnna Elisa Borges BarcelosNo ratings yet
- Academia Americana de Pediatrie - Transferul Medicamentelor Și Altor Substanțe În Laptele MaternDocument21 pagesAcademia Americana de Pediatrie - Transferul Medicamentelor Și Altor Substanțe În Laptele Maternadytt20005155No ratings yet
- 06 Adam Pharm3c PPT 06Document49 pages06 Adam Pharm3c PPT 06rachel.m.johnson9780No ratings yet
- Implementation and Organization of A Perioperative Lactation Program: A Descriptive StudyDocument9 pagesImplementation and Organization of A Perioperative Lactation Program: A Descriptive StudypkmpsNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptRaquel Orozco VargasNo ratings yet
- Focus Dorney Preconception 1Document6 pagesFocus Dorney Preconception 1Muvindu JayasingheNo ratings yet
- SKS Drug Safety Evaluation in Pregnancy and LactationDocument18 pagesSKS Drug Safety Evaluation in Pregnancy and LactationgariNo ratings yet
- Cme Reviewarticle: Preconception CareDocument13 pagesCme Reviewarticle: Preconception CareUziel Ávila GrimaldoNo ratings yet
- Trabajo Farmaco Quinto.Document4 pagesTrabajo Farmaco Quinto.sebastian yanezNo ratings yet
- PIIS0016508506008651Document29 pagesPIIS0016508506008651Ongoongoseven b. e. bNo ratings yet
- ABM Clinical Protocol #13: Contraception During Breastfeeding, Revised 2015Document10 pagesABM Clinical Protocol #13: Contraception During Breastfeeding, Revised 2015Dany DiasNo ratings yet
- Ovulación en SOPDocument10 pagesOvulación en SOPbeaprinaNo ratings yet
- 256 FullDocument7 pages256 FullAngga M RahmanNo ratings yet
- Napro Ireland 2008Document10 pagesNapro Ireland 2008Poliklinika LAB PLUSNo ratings yet
- Research Paper Medication ErrorsDocument6 pagesResearch Paper Medication Errorsegxtc6y3100% (1)
- MW3501 Pharmacology For Midwifery Practice PDFDocument2 pagesMW3501 Pharmacology For Midwifery Practice PDFLerma Navarro Reyes-Valencia100% (1)
- Breastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementDocument2 pagesBreastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementBayna Lestari LubisNo ratings yet
- Assessment of Knowledge, Attitude, and Practice On Self-Care With Over-The-Counter Medicines Among Pregnant WomenDocument6 pagesAssessment of Knowledge, Attitude, and Practice On Self-Care With Over-The-Counter Medicines Among Pregnant Womenmuhammad noor aswadNo ratings yet
- This Document Is Scheduled To Be Published in The Federal Register On 12/04/2014 and Available Online atDocument149 pagesThis Document Is Scheduled To Be Published in The Federal Register On 12/04/2014 and Available Online atVijendra RNo ratings yet
- Pregnancy CAM TurkeyDocument10 pagesPregnancy CAM TurkeyTuğba ÖzcanNo ratings yet
- Vajda 2020Document6 pagesVajda 2020María TeGeNo ratings yet
- Society For Maternal-Fetal Medicine Special Statement: Maternal-Fetal Medicine Subspecialist Survey On Abortion Training and Service ProvisionDocument10 pagesSociety For Maternal-Fetal Medicine Special Statement: Maternal-Fetal Medicine Subspecialist Survey On Abortion Training and Service Provisionmayang fabiolaNo ratings yet
- MeliyaDocument4 pagesMeliyaAni MustikaNo ratings yet
- Contraception for the Medically Challenging PatientFrom EverandContraception for the Medically Challenging PatientRebecca H. AllenNo ratings yet
- Formularium Rs Meta IndustriDocument36 pagesFormularium Rs Meta Industritiara dinantiNo ratings yet
- 17.alekhya Research ArticleDocument8 pages17.alekhya Research ArticleBaru Chandrasekhar RaoNo ratings yet
- Unit 1. Clinical PharmacyDocument5 pagesUnit 1. Clinical PharmacyAashish BhattaraiNo ratings yet
- Role and Responsibility of Pharmacy Assistant in Community PharmacyDocument4 pagesRole and Responsibility of Pharmacy Assistant in Community PharmacyUntouchable Monster 2No ratings yet
- BCS PrácticaDocument17 pagesBCS PrácticaEarvin GonzálezNo ratings yet
- Case Study DR Reddy-Industry PDFDocument61 pagesCase Study DR Reddy-Industry PDFSyed0% (2)
- Merck Gen Eurofarma Gen Sandoz Medley Ranbaxy Ache Gen Ems Gen Germed GSK RX SanofiDocument13 pagesMerck Gen Eurofarma Gen Sandoz Medley Ranbaxy Ache Gen Ems Gen Germed GSK RX SanofiLuiz PereiraNo ratings yet
- WHOPIR Ajanta DeskAssess 16-18nov2020Document11 pagesWHOPIR Ajanta DeskAssess 16-18nov2020Rosella PlantaNo ratings yet
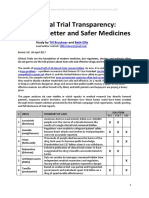
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Document21 pagesClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerNo ratings yet
- Melandari Stok PatenDocument12 pagesMelandari Stok PatennadiaNo ratings yet
- Atanasov Et Al (2015) Discovery and Resupply of Pharmacologically Active Plant-Derived Natural Product A ReviewDocument33 pagesAtanasov Et Al (2015) Discovery and Resupply of Pharmacologically Active Plant-Derived Natural Product A ReviewGenio Concedo TresdeseosNo ratings yet
- Saldo Penerimaan & Pengeluaran07 - Maret - 2021Document34 pagesSaldo Penerimaan & Pengeluaran07 - Maret - 2021Desi Yuliana HarahapNo ratings yet
- 022221s000 Lidocaine Clinical PREADocument13 pages022221s000 Lidocaine Clinical PREAjoelrequenaNo ratings yet
- IP121lec - Topic 3 - Calculation of Doses PDFDocument47 pagesIP121lec - Topic 3 - Calculation of Doses PDFBj LarracasNo ratings yet
- Stability Studies - An Overview: - What Is Stability? - Why It Is Required? - What Are The Guidelines?Document24 pagesStability Studies - An Overview: - What Is Stability? - Why It Is Required? - What Are The Guidelines?VidyaNo ratings yet
- Effects of Curcumin On The Pharmacokinetics of Amlodipine in Rats and Its Potential MechanismDocument5 pagesEffects of Curcumin On The Pharmacokinetics of Amlodipine in Rats and Its Potential MechanismShahid IqbalNo ratings yet
- Guidelines FOR Implementing Drug Utilization Review Programs IN HospitalsDocument58 pagesGuidelines FOR Implementing Drug Utilization Review Programs IN HospitalsMuhammad Faris MahmudNo ratings yet
- Prescription Verbs and Routes of AdminDocument2 pagesPrescription Verbs and Routes of AdminKingg AdjeiNo ratings yet
- ARTEMETHER Injectable - MSF Medical GuidelinesDocument2 pagesARTEMETHER Injectable - MSF Medical GuidelinesOjong YvesNo ratings yet
- PharmacopoeiasDocument18 pagesPharmacopoeiaslomje lNo ratings yet
- Atenolol FormDocument2 pagesAtenolol FormsevenssNo ratings yet
- Pharma OutlineDocument2 pagesPharma OutlineHassen ZabalaNo ratings yet
- 1 PBDocument14 pages1 PBindah marhaniNo ratings yet
- Introduction To Industrial PharmacyDocument27 pagesIntroduction To Industrial PharmacyHammad MurtazaNo ratings yet
- Bioavailability and First Pass MetabolismDocument37 pagesBioavailability and First Pass MetabolismFitrye Yhana Rayyi KurniawanNo ratings yet
- Testbankworld orDocument95 pagesTestbankworld orchip chipsNo ratings yet
- Biowaiver Approaches For Solid Oral Dosage Forms in New Drug Applications - V8 - FinalDocument47 pagesBiowaiver Approaches For Solid Oral Dosage Forms in New Drug Applications - V8 - FinalSrinivas Reddy MaramNo ratings yet
- Complete List of Subreddits To Build Drug Topic Corpus - JDI Supplementary MaterialDocument34 pagesComplete List of Subreddits To Build Drug Topic Corpus - JDI Supplementary MaterialJ CantuNo ratings yet