Download as pdf or txt
You might also like
- Essentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadDocument38 pagesEssentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadcarrielivingstonocifrtkgnyNo ratings yet
- Micro Lab Unknown Organism ReportDocument4 pagesMicro Lab Unknown Organism Reportapi-28115043250% (2)
- Diagnostics 13 03669Document15 pagesDiagnostics 13 03669Micran ThesisNo ratings yet
- 10 1200@jco 20 01661Document11 pages10 1200@jco 20 01661Pedro TurraNo ratings yet
- Int Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireDocument6 pagesInt Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireSid TNo ratings yet
- Keratocystic Odontogenic Tumour in A Hong Kong Community: The Clinical and Radiological FeaturesDocument9 pagesKeratocystic Odontogenic Tumour in A Hong Kong Community: The Clinical and Radiological FeaturesYenita AdetamaNo ratings yet
- Engel 2018Document11 pagesEngel 2018GonzaloNo ratings yet
- Abdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery A Series of 97Document8 pagesAbdi Et Al 2023 Operative Treatment of Tarlov Cysts Outcomes and Predictors of Improvement After Surgery A Series of 97jabarin.hNo ratings yet
- Hou, Et Al., 2021Document9 pagesHou, Et Al., 2021NyomantrianaNo ratings yet
- Review Article: Best Practice Management of Neck Pain in The Emergency Department (Part 6 of The Musculoskeletal Injuries Rapid Review Series)Document19 pagesReview Article: Best Practice Management of Neck Pain in The Emergency Department (Part 6 of The Musculoskeletal Injuries Rapid Review Series)Eduardo BarreraNo ratings yet
- Brain-Sparing Radiotherapy For Neuroblastoma Skull MetastasesDocument6 pagesBrain-Sparing Radiotherapy For Neuroblastoma Skull Metastasesasialoren74No ratings yet
- Incidence of Small Lymph Node Metastases in Patients With Nasopharyngeal Carcinoma: Clinical Implications For Prognosis and TreatmentDocument7 pagesIncidence of Small Lymph Node Metastases in Patients With Nasopharyngeal Carcinoma: Clinical Implications For Prognosis and TreatmentAdelin Luthfiana FajrinNo ratings yet
- 17-Potential Medicolegal RisksDocument1 page17-Potential Medicolegal RisksSUSANNo ratings yet
- Flexible CO2 Laser Treatment For Subglottic Stenosis, 2017Document2 pagesFlexible CO2 Laser Treatment For Subglottic Stenosis, 2017Araceli BarreraNo ratings yet
- Retrospective Study of Craniovertebral Junction (CVJ) Anomalies: A Clinical Profi Le and Outcome Analysis of Surgically Treated PatientsDocument7 pagesRetrospective Study of Craniovertebral Junction (CVJ) Anomalies: A Clinical Profi Le and Outcome Analysis of Surgically Treated PatientsNaga MuthuNo ratings yet
- 1530 Jul 27Document6 pages1530 Jul 27kelvin amahNo ratings yet
- DMFR 20170301Document7 pagesDMFR 20170301Ana PaulaNo ratings yet
- Journal RadiologiDocument8 pagesJournal RadiologiTenta Hartian HendyatamaNo ratings yet
- Gland CarcinomaDocument6 pagesGland CarcinomaVicko PratamaNo ratings yet
- Diagnostic Accuracy of Nasal Endoscopy As Compared To Computed Tomography in Chronic RhinosinusitisDocument6 pagesDiagnostic Accuracy of Nasal Endoscopy As Compared To Computed Tomography in Chronic RhinosinusitisJeffly Varro GilbertNo ratings yet
- 10 1097@scs 0000000000003278Document3 pages10 1097@scs 0000000000003278Meva'a RogerNo ratings yet
- Jurnal 3 Abses Leher DalamDocument6 pagesJurnal 3 Abses Leher DalamRohayu AsnawiNo ratings yet
- 2013 9 1 045 ChuangDocument8 pages2013 9 1 045 ChuangRamaMahardikaNo ratings yet
- 1 s2.0 S2452109422001890Document6 pages1 s2.0 S2452109422001890Raul Matute MartinNo ratings yet
- Koch 2009Document9 pagesKoch 2009Intan Kartika NursyahbaniNo ratings yet
- The Evaluation of Head and Craniocervical PostureDocument4 pagesThe Evaluation of Head and Craniocervical PostureDr. Zardasht N. BradostyNo ratings yet
- 026 Prof-2033Document4 pages026 Prof-2033dgina8800No ratings yet
- Repeatability and Validity of An Upper Limb and Neck Discomfort Questionnaire: The Utility of The Standardized Nordic QuestionnaireDocument6 pagesRepeatability and Validity of An Upper Limb and Neck Discomfort Questionnaire: The Utility of The Standardized Nordic QuestionnaireMuhammad SaleemNo ratings yet
- NIH Public Access: Author ManuscriptDocument23 pagesNIH Public Access: Author ManuscriptIntan Kartika NursyahbaniNo ratings yet
- JCM 12 07189Document11 pagesJCM 12 07189lehueanh.umpNo ratings yet
- Lam 2001 Espacio Subar.Document5 pagesLam 2001 Espacio Subar.Jimmy Pino CoricazaNo ratings yet
- Descriptive Study of The Differences in The Level of The Conus Medullaris in Four Different Age GroupsDocument7 pagesDescriptive Study of The Differences in The Level of The Conus Medullaris in Four Different Age GroupsregarskidNo ratings yet
- Endoscopic Endonasal Approach For Craniovertebral Junction Pathology A Review of The Literature, 2015Document5 pagesEndoscopic Endonasal Approach For Craniovertebral Junction Pathology A Review of The Literature, 2015CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Academic Emergency Medicine - 2011 - Adhikari - Pilot Study To Determine The Utility of Point of Care Ultrasound in TheDocument7 pagesAcademic Emergency Medicine - 2011 - Adhikari - Pilot Study To Determine The Utility of Point of Care Ultrasound in TheIndhu SubbuNo ratings yet
- Risk Factors For and The Role of Dental Extractions in Osteoradionecrosis of The Jaws: A National-Based Cohort StudyDocument9 pagesRisk Factors For and The Role of Dental Extractions in Osteoradionecrosis of The Jaws: A National-Based Cohort Studyita mustainahNo ratings yet
- Otolaryngol - Head Neck Surg - 2023 - Patel - Elective Neck Dissection For cT1 4 N0M0 Head and Neck Verrucous CarcinomaDocument13 pagesOtolaryngol - Head Neck Surg - 2023 - Patel - Elective Neck Dissection For cT1 4 N0M0 Head and Neck Verrucous CarcinomadrsubhajitfaciomaxsurgeonNo ratings yet
- The Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassesDocument10 pagesThe Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassestaufikolingNo ratings yet
- Factors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid NodulesDocument10 pagesFactors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid Nodulesmiguel saba sabaNo ratings yet
- Tto Crup NatureDocument7 pagesTto Crup NatureCarolina Mora RuedaNo ratings yet
- Puccinelli 2019Document8 pagesPuccinelli 2019RathavishwarajNo ratings yet
- Relationship Between Increased Intracranial Pressure and Mastoid EffusionDocument9 pagesRelationship Between Increased Intracranial Pressure and Mastoid EffusionFebrian Parlangga MuisNo ratings yet
- Craniopharyngioma 2 PDFDocument9 pagesCraniopharyngioma 2 PDFBea NufuarNo ratings yet
- Aksha Poster AbstractDocument14 pagesAksha Poster Abstractडॉ यश तलेराNo ratings yet
- Perilongo 1997Document7 pagesPerilongo 1997Gustav RSRNo ratings yet
- HNC Mdasi-HnDocument7 pagesHNC Mdasi-HnSinem GürçayNo ratings yet
- Case Study Intramedullary Spinal Cord TumorDocument13 pagesCase Study Intramedullary Spinal Cord TumorCitra KristiNo ratings yet
- Dorsal RhizotomyDocument13 pagesDorsal RhizotomyAiman MaidanNo ratings yet
- Medip, IJRMS-7729 ODocument7 pagesMedip, IJRMS-7729 ORagupathi MNo ratings yet
- Long Term (10 Year) Outcomes and Prognostic FactorDocument8 pagesLong Term (10 Year) Outcomes and Prognostic FactorNICOLÁS DANIEL SANCHEZ HERNANDEZNo ratings yet
- Microvascular Doppler Ultrasound in Children With Acute PyelonephritisDocument7 pagesMicrovascular Doppler Ultrasound in Children With Acute PyelonephritisAinunnisa MansurNo ratings yet
- 1 s2.0 S2214751921003911 Main - CompressedDocument9 pages1 s2.0 S2214751921003911 Main - Compressedinggrit thalasaviaNo ratings yet
- Original ContributionDocument9 pagesOriginal Contributiondesy 102017135No ratings yet
- Prognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based StudyDocument15 pagesPrognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based Studymahmud.meftahNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and Researchrhegi isdiara FairuzNo ratings yet
- Ca Hard PalateDocument8 pagesCa Hard Palatearif sudiantoNo ratings yet
- Operative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-AnalysisDocument9 pagesOperative Versus Nonoperative Treatments For Legg-Calve - Perthes Disease: A Meta-Analysisyarianna2No ratings yet
- Bacciu 2013Document10 pagesBacciu 2013AshokNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- Awake Craniotomy To Maximize Glioma Resection: Methods and Technical Nuances Over A 27-Year PeriodDocument15 pagesAwake Craniotomy To Maximize Glioma Resection: Methods and Technical Nuances Over A 27-Year Periodchenth3r3No ratings yet
- Cancer - 2003 - Greenberg - Extent of Extracapsular SpreadDocument7 pagesCancer - 2003 - Greenberg - Extent of Extracapsular SpreadVaredis T.No ratings yet
- 2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDocument4 pages2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDimitris RodriguezNo ratings yet
- 55.wilson1989pharyngoesophageal DysmotilityDocument5 pages55.wilson1989pharyngoesophageal DysmotilityWahyu JuliandaNo ratings yet
- Adenoids: What Are They & How Do They Affect My Child's Hearing?Document2 pagesAdenoids: What Are They & How Do They Affect My Child's Hearing?Wahyu JuliandaNo ratings yet
- 38.park2006 Diagnosis of Laryngopharyngeal Reflux AmongDocument5 pages38.park2006 Diagnosis of Laryngopharyngeal Reflux AmongWahyu JuliandaNo ratings yet
- Long-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyDocument5 pagesLong-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyWahyu JuliandaNo ratings yet
- Reconstruction of The EarDocument19 pagesReconstruction of The EarWahyu JuliandaNo ratings yet
- Mucosal Melanoma of The Head and Neck 32-Year ExperienceDocument5 pagesMucosal Melanoma of The Head and Neck 32-Year ExperienceWahyu JuliandaNo ratings yet
- Sep To RhinoplastyDocument27 pagesSep To RhinoplastyWahyu JuliandaNo ratings yet
- Nasal & Naso-Orbital-Ethmoid FractureDocument17 pagesNasal & Naso-Orbital-Ethmoid FractureWahyu JuliandaNo ratings yet
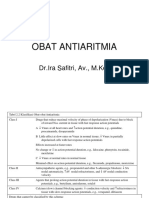
- Obat AntiaritmiaDocument18 pagesObat AntiaritmiaWahyu JuliandaNo ratings yet
- Wound Healing: Faculty of Medicine - Andalas University Dr. M. Djamil Hospital, Padang 2014Document23 pagesWound Healing: Faculty of Medicine - Andalas University Dr. M. Djamil Hospital, Padang 2014Wahyu JuliandaNo ratings yet
- Jurnal JiwaDocument10 pagesJurnal JiwaWahyu Julianda100% (1)
- Pathophysiology of Ischemic Heart DiseaseDocument28 pagesPathophysiology of Ischemic Heart DiseaseWahyu JuliandaNo ratings yet
- Documentation Testing: Using Active VoiceDocument3 pagesDocumentation Testing: Using Active VoiceWahyu JuliandaNo ratings yet
- Nurpr: Shipped To Shipment Info Payment InfoDocument1 pageNurpr: Shipped To Shipment Info Payment InfoWahyu JuliandaNo ratings yet
- Comparison With IOTF Cut-Offs (Boys)Document2 pagesComparison With IOTF Cut-Offs (Boys)Wahyu JuliandaNo ratings yet
- 02/27/09 - The Stanford Daily (PDF)Document8 pages02/27/09 - The Stanford Daily (PDF)The Stanford DailyNo ratings yet
- Blood BankDocument10 pagesBlood BankMarie LlanesNo ratings yet
- Who HCV 2018Document108 pagesWho HCV 2018hendrawanNo ratings yet
- Msds of HCLDocument9 pagesMsds of HCLMohd FirozNo ratings yet
- 1.1 Chromosomal Abnormalities: Hi H I Ef e FDocument26 pages1.1 Chromosomal Abnormalities: Hi H I Ef e FGlupiaSprawaNo ratings yet
- Underground Clinical Vignettes BiochemistryDocument128 pagesUnderground Clinical Vignettes Biochemistrymartha2112No ratings yet
- Talaroc Vs ArpaphilDocument2 pagesTalaroc Vs ArpaphilChe Ann Mae FloresNo ratings yet
- "Pharmaceutical Care": (Asuhan Kefarmasian)Document37 pages"Pharmaceutical Care": (Asuhan Kefarmasian)Ririn sefrianiNo ratings yet
- CBD DR Saugi IrfanDocument88 pagesCBD DR Saugi IrfanFebri BimayanaNo ratings yet
- Tai Chi - New Energy Ways, Energy Body Manipulation, Development - Robert BruceDocument61 pagesTai Chi - New Energy Ways, Energy Body Manipulation, Development - Robert BrucemuyelectricoNo ratings yet
- Chronic Spontaneous UrticariaDocument28 pagesChronic Spontaneous UrticariamaryNo ratings yet
- Yoga Eye Exercise - Eye Correction - Sun Gazing - Eye AccommodationDocument3 pagesYoga Eye Exercise - Eye Correction - Sun Gazing - Eye AccommodationZioAngelNo ratings yet
- Best Practice Workbook - Bipolar Disorder-Yong Xiang YiDocument45 pagesBest Practice Workbook - Bipolar Disorder-Yong Xiang YiJuraidahMohdNooh100% (1)
- Chrysonilia Sitophila Growth On Different CultureDocument7 pagesChrysonilia Sitophila Growth On Different CultureDemetriaNo ratings yet
- Veterinary Medical Terminology: Dr.H.HoseinzadehDocument16 pagesVeterinary Medical Terminology: Dr.H.HoseinzadehJuk CondeNo ratings yet
- Final Study Guide 2020 - Nursing 1119Document5 pagesFinal Study Guide 2020 - Nursing 1119KashaNo ratings yet
- Trinity United Church of Christ BulletinDocument28 pagesTrinity United Church of Christ BulletinWorlee GloverNo ratings yet
- Induction Update2Document30 pagesInduction Update2yusepNo ratings yet
- Unit 3 AtherosclerosisDocument29 pagesUnit 3 AtherosclerosisJack TomarNo ratings yet
- MNT Case StudyDocument13 pagesMNT Case Studyapi-384503305No ratings yet
- Hydrogen Peroxide Magic - Thacker.bDocument209 pagesHydrogen Peroxide Magic - Thacker.bMathieu ChautardNo ratings yet
- Bacterial Genetics 2020Document67 pagesBacterial Genetics 2020Ntobi ThomasNo ratings yet
- Jurnal SkizofreniaDocument9 pagesJurnal SkizofreniaAbdul HamidNo ratings yet
- Section - 037 - Denture Occlusion - Non-BalancedDocument14 pagesSection - 037 - Denture Occlusion - Non-BalancedWafa AbdurahmanNo ratings yet
- Latihan Soal Literasi Bahasa Inggris 1Document9 pagesLatihan Soal Literasi Bahasa Inggris 1Daffa AryaputraNo ratings yet
- Scan 09-Dec-2018Document7 pagesScan 09-Dec-2018Rahul SinhaNo ratings yet
- Gene Transfer Questions-2021Document4 pagesGene Transfer Questions-2021Kaif AliNo ratings yet
- PlasmodiumDocument46 pagesPlasmodiumMuna MaranNo ratings yet