
Jurnal Spondylolithesis Dr. Angga 1
Jurnal Spondylolithesis Dr. Angga 1
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- IES Test Prep Answer Explanations For SAT GrammarDocument72 pagesIES Test Prep Answer Explanations For SAT GrammarĐ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘̚ Đ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘75% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- RMU Test ReportDocument3 pagesRMU Test ReportGANESH K75% (4)
- EASA Part-66 Exam Questions of Module 01 - Part IIDocument24 pagesEASA Part-66 Exam Questions of Module 01 - Part IISteven J. Selcuk100% (2)
- J of Obstet and Gynaecol - 2022 - La Verde - Incidence of Gestational Diabetes Mellitus Before and After The Covid 19Document6 pagesJ of Obstet and Gynaecol - 2022 - La Verde - Incidence of Gestational Diabetes Mellitus Before and After The Covid 19the OGs. 96No ratings yet
- Original Article: ObjectiveDocument8 pagesOriginal Article: Objectivethe OGs. 96No ratings yet
- The Effect of ICT Qualification On Selection of Long Term SuppliersDocument9 pagesThe Effect of ICT Qualification On Selection of Long Term Suppliersthe OGs. 96No ratings yet
- Poa 00147Document7 pagesPoa 00147the OGs. 96No ratings yet
- NM 2020 27 4 151Document8 pagesNM 2020 27 4 151the OGs. 96No ratings yet
- 1526-Article Text-5710-2-10-20201126Document13 pages1526-Article Text-5710-2-10-20201126the OGs. 96No ratings yet
- Frequency Analysis of Handwriting For Diagnosis of Parkinson's DiseaseDocument7 pagesFrequency Analysis of Handwriting For Diagnosis of Parkinson's Diseasethe OGs. 96No ratings yet
- Military Hospitals Through The Prism of Sociology of ArchitectureDocument9 pagesMilitary Hospitals Through The Prism of Sociology of Architecturethe OGs. 96No ratings yet
- 5550-Article Text-42309-3-10-20220104Document8 pages5550-Article Text-42309-3-10-20220104the OGs. 96No ratings yet
- Jurnal Spondylolithesis Dr. Angga 4Document9 pagesJurnal Spondylolithesis Dr. Angga 4the OGs. 96No ratings yet
- Jourding Frozen Shoulder Tio Ugantoro 4Document5 pagesJourding Frozen Shoulder Tio Ugantoro 4the OGs. 96No ratings yet
- Post-Traumatic Stress Disorder and Psychological Distress in Chinese Youths Following The COVID-19 EmergencyDocument22 pagesPost-Traumatic Stress Disorder and Psychological Distress in Chinese Youths Following The COVID-19 Emergencythe OGs. 96No ratings yet
- Ciarrochi Fisher and Lane Link Between Values and Well-Being Among People With Cancer 2010 Psycho OncologyDocument9 pagesCiarrochi Fisher and Lane Link Between Values and Well-Being Among People With Cancer 2010 Psycho OncologyJuan C. VargasNo ratings yet
- Petroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityDocument13 pagesPetroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityAli AbubakarNo ratings yet
- W8 Module08 Meaning and Relevance of History Presentation 1Document22 pagesW8 Module08 Meaning and Relevance of History Presentation 1Jessa UdtohanNo ratings yet
- Catalogo ColonneDocument140 pagesCatalogo Colonneapi-18378576No ratings yet
- TapingDocument3 pagesTapingEdeza MatarumNo ratings yet
- Omnivision Man lp06xx Rev0 0611Document18 pagesOmnivision Man lp06xx Rev0 0611ivan ramirezNo ratings yet
- Advanced Landscape DesignDocument10 pagesAdvanced Landscape DesignSomhita DasNo ratings yet
- Mec R2018Document227 pagesMec R2018Kishore Kumar RNo ratings yet
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Geometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALDocument67 pagesGeometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALdrssagrawalNo ratings yet
- Mid Rex 7Document22 pagesMid Rex 7Sudeshna RoyNo ratings yet
- Data Sheet USB5 II 2019 05 ENDocument1 pageData Sheet USB5 II 2019 05 ENJanne LaineNo ratings yet
- BSD-GL-HAL-HMS-100 - (Terms & Definitions)Document42 pagesBSD-GL-HAL-HMS-100 - (Terms & Definitions)Eduard GadzhievNo ratings yet
- 9852 1880 01 Maintenance Instructions ROC L7CR IIDocument102 pages9852 1880 01 Maintenance Instructions ROC L7CR IIphongNo ratings yet
- Tac85 11Document32 pagesTac85 11TateNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- Bata Shoe Company (Bangladesh) Ltd.Document6 pagesBata Shoe Company (Bangladesh) Ltd.Vurdalack666No ratings yet
- (2001) (Sun) (Two-Group Interfacial Area Transport Equation For A Confined Test Section)Document367 pages(2001) (Sun) (Two-Group Interfacial Area Transport Equation For A Confined Test Section)Erol BicerNo ratings yet
- Autonomous University of Baja California: Faculty of Engineering Aerospace EngineeringDocument18 pagesAutonomous University of Baja California: Faculty of Engineering Aerospace EngineeringOscar Oreste Salvador CarlosNo ratings yet
- Problem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0Document17 pagesProblem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0gtech00100% (1)
- Peniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Document3 pagesPeniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Jhocen Grace GanironNo ratings yet
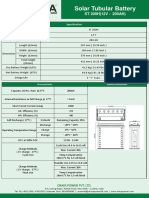
- ST200HDocument2 pagesST200HAnjana DissanayakaNo ratings yet
- Soal PAS K13 Kelas 9 Ganjil Tp. 2019-2020Document5 pagesSoal PAS K13 Kelas 9 Ganjil Tp. 2019-2020Fairuz AbadiNo ratings yet
- SSP 604 - Audi 30l v6 Tdi Biturbo Engine EngDocument23 pagesSSP 604 - Audi 30l v6 Tdi Biturbo Engine Engfrancois.garcia31100% (1)
- Model 621 LR B Data SheetDocument1 pageModel 621 LR B Data SheetMohammed GallowNo ratings yet
- DC Jow Ga Beginner CurriculumDocument2 pagesDC Jow Ga Beginner CurriculumKevinNo ratings yet

















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- IES Test Prep Answer Explanations For SAT GrammarDocument72 pagesIES Test Prep Answer Explanations For SAT GrammarĐ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘̚ Đ̸̢͓͉̣͔̭̜̭͉̰́͌͑͊̇̏̕̚͜͜ͅứ̷̢̛̘̭̤͎̩̣̩̊̆̑̓̽̓͗ͅc̴̟͈̠̤̪͈͍̰̟̤̮̆̄̈́̈̃̏̃̑̊͠͝ä̷̧̰̲̦́̒̐͝ṉ̵̾̀͗̾h̷̥͆͑̍͌͆̋̈́́͒͂̇͘75% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- RMU Test ReportDocument3 pagesRMU Test ReportGANESH K75% (4)
- EASA Part-66 Exam Questions of Module 01 - Part IIDocument24 pagesEASA Part-66 Exam Questions of Module 01 - Part IISteven J. Selcuk100% (2)
- J of Obstet and Gynaecol - 2022 - La Verde - Incidence of Gestational Diabetes Mellitus Before and After The Covid 19Document6 pagesJ of Obstet and Gynaecol - 2022 - La Verde - Incidence of Gestational Diabetes Mellitus Before and After The Covid 19the OGs. 96No ratings yet
- Original Article: ObjectiveDocument8 pagesOriginal Article: Objectivethe OGs. 96No ratings yet
- The Effect of ICT Qualification On Selection of Long Term SuppliersDocument9 pagesThe Effect of ICT Qualification On Selection of Long Term Suppliersthe OGs. 96No ratings yet
- Poa 00147Document7 pagesPoa 00147the OGs. 96No ratings yet
- NM 2020 27 4 151Document8 pagesNM 2020 27 4 151the OGs. 96No ratings yet
- 1526-Article Text-5710-2-10-20201126Document13 pages1526-Article Text-5710-2-10-20201126the OGs. 96No ratings yet
- Frequency Analysis of Handwriting For Diagnosis of Parkinson's DiseaseDocument7 pagesFrequency Analysis of Handwriting For Diagnosis of Parkinson's Diseasethe OGs. 96No ratings yet
- Military Hospitals Through The Prism of Sociology of ArchitectureDocument9 pagesMilitary Hospitals Through The Prism of Sociology of Architecturethe OGs. 96No ratings yet
- 5550-Article Text-42309-3-10-20220104Document8 pages5550-Article Text-42309-3-10-20220104the OGs. 96No ratings yet
- Jurnal Spondylolithesis Dr. Angga 4Document9 pagesJurnal Spondylolithesis Dr. Angga 4the OGs. 96No ratings yet
- Jourding Frozen Shoulder Tio Ugantoro 4Document5 pagesJourding Frozen Shoulder Tio Ugantoro 4the OGs. 96No ratings yet
- Post-Traumatic Stress Disorder and Psychological Distress in Chinese Youths Following The COVID-19 EmergencyDocument22 pagesPost-Traumatic Stress Disorder and Psychological Distress in Chinese Youths Following The COVID-19 Emergencythe OGs. 96No ratings yet
- Ciarrochi Fisher and Lane Link Between Values and Well-Being Among People With Cancer 2010 Psycho OncologyDocument9 pagesCiarrochi Fisher and Lane Link Between Values and Well-Being Among People With Cancer 2010 Psycho OncologyJuan C. VargasNo ratings yet
- Petroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityDocument13 pagesPetroleum Engineering Lab 1 (PGE313) Experiment 2 Determination of PorosityAli AbubakarNo ratings yet
- W8 Module08 Meaning and Relevance of History Presentation 1Document22 pagesW8 Module08 Meaning and Relevance of History Presentation 1Jessa UdtohanNo ratings yet
- Catalogo ColonneDocument140 pagesCatalogo Colonneapi-18378576No ratings yet
- TapingDocument3 pagesTapingEdeza MatarumNo ratings yet
- Omnivision Man lp06xx Rev0 0611Document18 pagesOmnivision Man lp06xx Rev0 0611ivan ramirezNo ratings yet
- Advanced Landscape DesignDocument10 pagesAdvanced Landscape DesignSomhita DasNo ratings yet
- Mec R2018Document227 pagesMec R2018Kishore Kumar RNo ratings yet
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Geometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALDocument67 pagesGeometry - Olympiad Material BY DR SHYAM SUNDAR AGRAWALdrssagrawalNo ratings yet
- Mid Rex 7Document22 pagesMid Rex 7Sudeshna RoyNo ratings yet
- Data Sheet USB5 II 2019 05 ENDocument1 pageData Sheet USB5 II 2019 05 ENJanne LaineNo ratings yet
- BSD-GL-HAL-HMS-100 - (Terms & Definitions)Document42 pagesBSD-GL-HAL-HMS-100 - (Terms & Definitions)Eduard GadzhievNo ratings yet
- 9852 1880 01 Maintenance Instructions ROC L7CR IIDocument102 pages9852 1880 01 Maintenance Instructions ROC L7CR IIphongNo ratings yet
- Tac85 11Document32 pagesTac85 11TateNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- Bata Shoe Company (Bangladesh) Ltd.Document6 pagesBata Shoe Company (Bangladesh) Ltd.Vurdalack666No ratings yet
- (2001) (Sun) (Two-Group Interfacial Area Transport Equation For A Confined Test Section)Document367 pages(2001) (Sun) (Two-Group Interfacial Area Transport Equation For A Confined Test Section)Erol BicerNo ratings yet
- Autonomous University of Baja California: Faculty of Engineering Aerospace EngineeringDocument18 pagesAutonomous University of Baja California: Faculty of Engineering Aerospace EngineeringOscar Oreste Salvador CarlosNo ratings yet
- Problem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0Document17 pagesProblem: Determine The Total Volume of Earth To Be Excavated Up To Elevation 0gtech00100% (1)
- Peniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Document3 pagesPeniel Integrated Christian Academy of Rizal, Inc. Science Weblinks GRADE 4 S.Y. 2020-2021Jhocen Grace GanironNo ratings yet
- ST200HDocument2 pagesST200HAnjana DissanayakaNo ratings yet
- Soal PAS K13 Kelas 9 Ganjil Tp. 2019-2020Document5 pagesSoal PAS K13 Kelas 9 Ganjil Tp. 2019-2020Fairuz AbadiNo ratings yet
- SSP 604 - Audi 30l v6 Tdi Biturbo Engine EngDocument23 pagesSSP 604 - Audi 30l v6 Tdi Biturbo Engine Engfrancois.garcia31100% (1)
- Model 621 LR B Data SheetDocument1 pageModel 621 LR B Data SheetMohammed GallowNo ratings yet
- DC Jow Ga Beginner CurriculumDocument2 pagesDC Jow Ga Beginner CurriculumKevinNo ratings yet