Download as pdf or txt
You might also like
- Aortic Stenosis (As)Document20 pagesAortic Stenosis (As)rameshbmc100% (1)
- Dudek 2409 Esc2007 SlidesDocument22 pagesDudek 2409 Esc2007 SlidesNagatzulNo ratings yet
- Risk of Gastrointestinal Bleeding in Patients With End-Stage Renal DiseaseDocument10 pagesRisk of Gastrointestinal Bleeding in Patients With End-Stage Renal DiseaseEuclea MandolangNo ratings yet
- 1 s2.0 S0002914913024521 MainDocument6 pages1 s2.0 S0002914913024521 MainJicko Street HooligansNo ratings yet
- JCM 08 01530Document14 pagesJCM 08 01530Medicina FamiliarNo ratings yet
- ACCP Cardiology PRN JC June 2022Document16 pagesACCP Cardiology PRN JC June 2022topNo ratings yet
- Association of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIADocument9 pagesAssociation of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIAJhonny Churata HuarachiNo ratings yet
- Hamaguchi 2009Document7 pagesHamaguchi 2009Nur Syamsiah MNo ratings yet
- Clinical and Procedural Predictors of No-Reflow Phenomenon After Primary Percutaneous Coronary InterventionsDocument6 pagesClinical and Procedural Predictors of No-Reflow Phenomenon After Primary Percutaneous Coronary InterventionsJose Manuel Ornelas-AguirreNo ratings yet
- JurnalDocument16 pagesJurnalGemmy SistarinaNo ratings yet
- Association of Platelet-to-Lymphocyte Ratio With Severity and Complexity of Coronary Artery Disease in Patients With Acute Coronary SyndromesDocument7 pagesAssociation of Platelet-to-Lymphocyte Ratio With Severity and Complexity of Coronary Artery Disease in Patients With Acute Coronary SyndromesMaferNo ratings yet
- AA - Cochrane 1Document5 pagesAA - Cochrane 1Angga Putra PramanaNo ratings yet
- Bun PDFDocument6 pagesBun PDFNida NurfadhilahNo ratings yet
- Usefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityDocument6 pagesUsefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityJicko Street HooligansNo ratings yet
- Gangguan Kardiovaskular Pada Pasien Dialisis (HD Dan PD)Document47 pagesGangguan Kardiovaskular Pada Pasien Dialisis (HD Dan PD)rivan100% (1)
- Clinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, NonDocument4 pagesClinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, Nonrobert_andrei_68No ratings yet
- Cardiac Risk in ESRD Patient-2Document42 pagesCardiac Risk in ESRD Patient-2mehta100% (1)
- DIABertelt2017 14Document7 pagesDIABertelt2017 14marsim92No ratings yet
- Moulis2018 PDFDocument4 pagesMoulis2018 PDFDwita MargarethNo ratings yet
- Bab II Laporan PBLDocument10 pagesBab II Laporan PBLAnnisa Aulia FitriNo ratings yet
- Association Between Preoperative Ambulatory Heart Rate and Postoperative Myocardial Injury: A Retrospective Cohort StudyDocument8 pagesAssociation Between Preoperative Ambulatory Heart Rate and Postoperative Myocardial Injury: A Retrospective Cohort StudyRicardoNo ratings yet
- Toxins 12 00420 v3Document11 pagesToxins 12 00420 v3Carlos Miguel Mendoza LlamocaNo ratings yet
- Risk Factor For Pressure Sores in Hozpitalized Acute Ischemic Stroke PatientDocument21 pagesRisk Factor For Pressure Sores in Hozpitalized Acute Ischemic Stroke PatientMediana FimedNo ratings yet
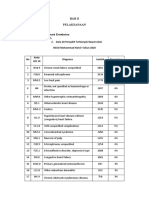
- 10 Penyakit Terbanyak Rawat Inap Pasien BPJS Kesehatan: No Kode ICD 1Document5 pages10 Penyakit Terbanyak Rawat Inap Pasien BPJS Kesehatan: No Kode ICD 1diah ayu kusumawardaniNo ratings yet
- SupplementaryDocument5 pagesSupplementaryResidenPatKlin Juli2022No ratings yet
- Predictive Variables For Mortality After Acute Ischemic StrokeDocument9 pagesPredictive Variables For Mortality After Acute Ischemic StrokeOscar PérezNo ratings yet
- Pubmed Symptom BasedDocument11 pagesPubmed Symptom BasedUyên HoàngNo ratings yet
- Lee Et Al. 2017 Am J Cardiol OA vs. RADocument4 pagesLee Et Al. 2017 Am J Cardiol OA vs. RAPraveenVeeraNo ratings yet
- Zhang 2021Document6 pagesZhang 2021KOBE BRIAN PETEROSNo ratings yet
- Cardiovascular Diseases (CVD) Greatly Threaten Filipinos Today. Atherosclerotic Changes in The BloodDocument5 pagesCardiovascular Diseases (CVD) Greatly Threaten Filipinos Today. Atherosclerotic Changes in The BloodmusikaNo ratings yet
- Clinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, NonDocument4 pagesClinical Study Report: Open-Label, Non-Randomized, National, Multicentric, Prospective, NonMarius AdrianNo ratings yet
- Nternational Ournal of Esearch Cience & AnagementDocument6 pagesNternational Ournal of Esearch Cience & AnagementhafizmahruzzaNo ratings yet
- Silent Intracerebral Hemorrhage in Patients Randomized To Stenting or Endarterectomy For Symptomatic Carotid StenosisDocument4 pagesSilent Intracerebral Hemorrhage in Patients Randomized To Stenting or Endarterectomy For Symptomatic Carotid Stenosisayu lestariNo ratings yet
- Jurnal Kesmas - Neurological Manifestations in COVID-19 Patients at The Covid-19 National Emergency Hospital Wisma Atlet Kemayoran, IndonesiaDocument16 pagesJurnal Kesmas - Neurological Manifestations in COVID-19 Patients at The Covid-19 National Emergency Hospital Wisma Atlet Kemayoran, IndonesianskhldNo ratings yet
- Digoxin Reduces 30-Day All-Cause Hospital Admission in Ambulatory Older Patients With Chronic Heart Failure and Reduced Ejection FractionDocument31 pagesDigoxin Reduces 30-Day All-Cause Hospital Admission in Ambulatory Older Patients With Chronic Heart Failure and Reduced Ejection FractionYanely AlmaguerNo ratings yet
- DR. PAUL REGANIT - Nutrition Lecture March 1Document49 pagesDR. PAUL REGANIT - Nutrition Lecture March 1Sophie RoseNo ratings yet
- TMP 4760Document6 pagesTMP 4760FrontiersNo ratings yet
- Univ A RiataDocument1 pageUniv A RiatasabathNo ratings yet
- Ehf2 7 1125Document5 pagesEhf2 7 1125Pranvera ApostoliNo ratings yet
- Brain Trauma Foundation Guidelines For Intracranial Pressure Monitoring: Compliance and Effect On OutcomeDocument7 pagesBrain Trauma Foundation Guidelines For Intracranial Pressure Monitoring: Compliance and Effect On OutcomeMilzaNo ratings yet
- The Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeDocument6 pagesThe Total Cholesterol To High-Density Lipoprotein Cholesterol As A Predictor of Poor Outcomes in A Chinese Population With Acute Ischaemic StrokeRay HannaNo ratings yet
- Contrast-Induced Acute Kidney Injury After Primary Percutaneous Coronary Intervention: Results From The HORIZONS-AMI SubstudyDocument9 pagesContrast-Induced Acute Kidney Injury After Primary Percutaneous Coronary Intervention: Results From The HORIZONS-AMI SubstudysarahNo ratings yet
- Updated Hypertension GuidelineDocument88 pagesUpdated Hypertension Guidelinekenny631653No ratings yet
- Disease: Colchicine in Patients With Chronic CoronaryDocument8 pagesDisease: Colchicine in Patients With Chronic CoronaryNiki MawraNo ratings yet
- History and Examination at A Glance PDFDocument207 pagesHistory and Examination at A Glance PDFradiocatifea100% (1)
- Liver Transplantation For Urea Cycle DisordersDocument6 pagesLiver Transplantation For Urea Cycle DisordersHamilton CeballosNo ratings yet
- (10920684 - Neurosurgical Focus) Morbidity and Mortality Associated With Hypernatremia in Patients With Severe Traumatic Brain InjuryDocument5 pages(10920684 - Neurosurgical Focus) Morbidity and Mortality Associated With Hypernatremia in Patients With Severe Traumatic Brain InjuryMariam PlataNo ratings yet
- Journal Review2Document7 pagesJournal Review2api-589685298No ratings yet
- Agarwal 2020Document4 pagesAgarwal 2020isabellaNo ratings yet
- Dummy Table FixDocument6 pagesDummy Table FixintansusmitaNo ratings yet
- Audit of RBC TransfusionDocument30 pagesAudit of RBC TransfusionRahul ChaurasiaNo ratings yet
- 01 Ortel BRIDGEDocument24 pages01 Ortel BRIDGEWallnut StreetNo ratings yet
- Nafilyan 2022 LD 220214 1661882440.67582Document5 pagesNafilyan 2022 LD 220214 1661882440.67582isrealvirgin763No ratings yet
- JR PED WebDocument13 pagesJR PED WebDina RyantiNo ratings yet
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaNo ratings yet
- Registro SuecoDocument7 pagesRegistro SuecoCarlos EghiNo ratings yet
- 1 s2.0 S0735109716366992 mmc1Document8 pages1 s2.0 S0735109716366992 mmc1Pangala NitaNo ratings yet
- Supplementary Appendix 2Document8 pagesSupplementary Appendix 2jsjwbrbr9rNo ratings yet
- Textbook The MRCP Paces Handbook Second Edition Blows Ebook All Chapter PDFDocument53 pagesTextbook The MRCP Paces Handbook Second Edition Blows Ebook All Chapter PDFjacob.henry689100% (3)
- Microcirculation: Current Physiologic, Medical, and Surgical ConceptsFrom EverandMicrocirculation: Current Physiologic, Medical, and Surgical ConceptsRichard EffrosNo ratings yet
- RIISPOA (En)Document13 pagesRIISPOA (En)Caio F Gonçalves NNo ratings yet
- Pda Awareness Matters Booklet 2016 Revised Edition Web VersionDocument36 pagesPda Awareness Matters Booklet 2016 Revised Edition Web VersionCristina100% (2)
- Introduction To Microbiology: Ma. Concepcion A. Maico, RN, Man, EddDocument24 pagesIntroduction To Microbiology: Ma. Concepcion A. Maico, RN, Man, EddIconMaicoNo ratings yet
- Research in Biotechnology1Document16 pagesResearch in Biotechnology1Gaurav JoshiNo ratings yet
- WEEK 3 Classification of Nutrients NutritionDocument33 pagesWEEK 3 Classification of Nutrients NutritionLaida PaguitalNo ratings yet
- Health, Stress, and CopingDocument49 pagesHealth, Stress, and CopingMarissa BrionesNo ratings yet
- BrucellosisDocument65 pagesBrucellosisKotha Chaitanya AbhiramNo ratings yet
- Accord StudyDocument169 pagesAccord StudyRobert DinuNo ratings yet
- Historical AntecedentsDocument17 pagesHistorical AntecedentsBench Adrian AvilaNo ratings yet
- Nutritional AssessmentDocument61 pagesNutritional Assessmentshahid9212No ratings yet
- MicroPara ReviewerDocument22 pagesMicroPara ReviewerAina HaravataNo ratings yet
- 3 CFTDocument9 pages3 CFTMunir AhmedNo ratings yet
- Mini Poster - Stevens Johnson SyndromeDocument21 pagesMini Poster - Stevens Johnson SyndromesandykartikaNo ratings yet
- Oncology Drills With Answers and RationalesDocument41 pagesOncology Drills With Answers and RationalesCarol Kayas100% (1)
- Biochemistry and Cell Biology of Ageing: Part III Biomedical ScienceDocument424 pagesBiochemistry and Cell Biology of Ageing: Part III Biomedical ScienceAureliano BuendiaNo ratings yet
- Drug StudyDocument6 pagesDrug StudyGracie S. VergaraNo ratings yet
- 2.4 SURG1 OncoDocument8 pages2.4 SURG1 OncoGeriz Daniella VigoNo ratings yet
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Thesis On Antioxidant Activity of Medicinal Plants PDFDocument6 pagesThesis On Antioxidant Activity of Medicinal Plants PDFafazapfjl100% (2)
- Overview & History of Quantitative GeneticsDocument8 pagesOverview & History of Quantitative GeneticsC'estMoiNo ratings yet
- Amon409 415Document7 pagesAmon409 415MogleNo ratings yet
- Review of Literature On Dairy Farming in IndiaDocument6 pagesReview of Literature On Dairy Farming in Indiac5nc3whz100% (1)
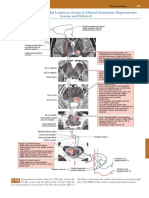
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- Surgeons and AnesthesiaDocument263 pagesSurgeons and AnesthesiaLuis A De la CubaNo ratings yet
- Respondent Memo (Shivam Sharma)Document16 pagesRespondent Memo (Shivam Sharma)Abhimanyu SinghNo ratings yet
- Post Herpetic Neuralgia andDocument63 pagesPost Herpetic Neuralgia andEndahD'LamdaNo ratings yet
- Rainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansDocument3 pagesRainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansTitikshaNo ratings yet
- 11.03.21 COVID-19 Vaccine Information - IDPHDocument5 pages11.03.21 COVID-19 Vaccine Information - IDPHLocal 5 News (WOI-TV)No ratings yet
- Triangular Fibrocartilage Complex Injury in Professional CricketersDocument5 pagesTriangular Fibrocartilage Complex Injury in Professional Cricketersrima rizky nourliaNo ratings yet