Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MERCER '09 - Flexible Benefits & Asia's ExperienceDocument34 pagesMERCER '09 - Flexible Benefits & Asia's ExperienceBurn HallNo ratings yet
- Chapter 3Document8 pagesChapter 3larra100% (2)
- Monk Fruit SweetenerDocument45 pagesMonk Fruit SweetenerEunica FadriquelaNo ratings yet
- Coronavirus Disease 2019 - COVID-19: April 2020Document76 pagesCoronavirus Disease 2019 - COVID-19: April 2020ASHWIN BALAJI RNo ratings yet
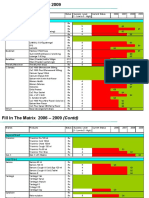
- Fill in The Matrix 2006 - 2009Document4 pagesFill in The Matrix 2006 - 2009Burn HallNo ratings yet
- Mercer 2012 PK TRS Job Matching BookletDocument595 pagesMercer 2012 PK TRS Job Matching BookletBurn Hall100% (1)
- A Man For All Seasons: Actor CharacterDocument2 pagesA Man For All Seasons: Actor CharacterBurn HallNo ratings yet
- Sales Model Applied - South AsiaDocument9 pagesSales Model Applied - South AsiaBurn HallNo ratings yet
- 1ABCosting TemplateDocument1 page1ABCosting TemplateBurn HallNo ratings yet
- IBC of AquaponicsDocument187 pagesIBC of AquaponicsJohnNo ratings yet
- Accenture Health 2017 Internet of Health Things SurveyDocument27 pagesAccenture Health 2017 Internet of Health Things SurveyBurn HallNo ratings yet
- Action Plan GPTWDocument6 pagesAction Plan GPTWBurn HallNo ratings yet
- Proposal 111023 For Novartis Otc Pakistan: Proposed Theme: " Beyond The Summit"Document6 pagesProposal 111023 For Novartis Otc Pakistan: Proposed Theme: " Beyond The Summit"Burn HallNo ratings yet
- Bell Siphon DesignDocument85 pagesBell Siphon DesignBurn HallNo ratings yet
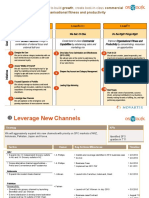
- Leap:: Three Pathways To Build Growth, Create Best-In-Class CommercialDocument2 pagesLeap:: Three Pathways To Build Growth, Create Best-In-Class CommercialBurn HallNo ratings yet
- Best - Energy Licence Agreement: Standard Terms & Conditions of Appointment V1.7 - Created 06th October 2021Document25 pagesBest - Energy Licence Agreement: Standard Terms & Conditions of Appointment V1.7 - Created 06th October 2021Burn HallNo ratings yet
- Digital Health Tech VISION 2018: Intelligent Enterprise UnleashedDocument32 pagesDigital Health Tech VISION 2018: Intelligent Enterprise UnleashedBurn HallNo ratings yet
- New GSK Consumer Healthcare Communications Pack: Monday 2nd MarchDocument51 pagesNew GSK Consumer Healthcare Communications Pack: Monday 2nd MarchBurn HallNo ratings yet
- Field Force IncentiveDocument1 pageField Force IncentiveBurn HallNo ratings yet
- ENDORSEMENT SX DraftDocument3 pagesENDORSEMENT SX DraftRED STATIONNo ratings yet
- IjdaDocument5 pagesIjdaSyed NooraniNo ratings yet
- Lab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainDocument4 pagesLab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainAdn crnNo ratings yet
- Chapter 2Document2 pagesChapter 2Castro RicNo ratings yet
- s11882 018 0806 6 PDFDocument7 pagess11882 018 0806 6 PDFHildreth Rosel SabioNo ratings yet
- Malawi Public Health ActDocument63 pagesMalawi Public Health ActKondwani AndreahNo ratings yet
- Molar Distalization PDFDocument3 pagesMolar Distalization PDFdruzair00775% (4)
- Aportul de Potasiu in Hipertensiunea Arteriala 2024Document9 pagesAportul de Potasiu in Hipertensiunea Arteriala 2024claudiu balabanNo ratings yet
- Overview of CMAMDocument33 pagesOverview of CMAMMd Faruque Ahmad100% (1)
- Angelman Syndrome Rough DraftDocument8 pagesAngelman Syndrome Rough Draftapi-540190838No ratings yet
- AARC Clinical Practice Guideline - Management of Airway EmergenciesDocument7 pagesAARC Clinical Practice Guideline - Management of Airway EmergenciesdoterofthemosthighNo ratings yet
- Pericardial DiseseasDocument38 pagesPericardial Diseseasmameekasim75No ratings yet
- FosfomycinDocument5 pagesFosfomycinThyThyydnNo ratings yet
- ETI-SR AU1.0 eng-USori ReviewDocument30 pagesETI-SR AU1.0 eng-USori ReviewXimena Alicia García AvendañoNo ratings yet
- PsikopatologiDocument25 pagesPsikopatologiShella Thea WibawaNo ratings yet
- EincDocument14 pagesEincmendoza jhamNo ratings yet
- Artikel Rev 1Document19 pagesArtikel Rev 1ChrisnaArdhyaMedikaNo ratings yet
- Resilience in Challenging Times 30min Presentation PDFDocument7 pagesResilience in Challenging Times 30min Presentation PDFRaul Gonzales Bianco EspinosaNo ratings yet
- 2492 AAP RCUK PET Chart-5Document1 page2492 AAP RCUK PET Chart-5Essam HassanNo ratings yet
- TB of Genital TractDocument29 pagesTB of Genital TractKasi Krishna Raja100% (2)
- Vol.13 Human Performance and LimitationsDocument222 pagesVol.13 Human Performance and LimitationsMostafa MohsenNo ratings yet
- Final Paper - Tiktok As A Covid-19 Discussion Platform of Bicol University College of Arts and LettersDocument98 pagesFinal Paper - Tiktok As A Covid-19 Discussion Platform of Bicol University College of Arts and Letterskathy macadat100% (1)
- World Bispecific Summit Brochure v9Document20 pagesWorld Bispecific Summit Brochure v9Nadeem JamalNo ratings yet
- 18 Diseases of Passion Fruit PDFDocument29 pages18 Diseases of Passion Fruit PDFmvbgarciaNo ratings yet
- Faidey Ka Insurance Faidey Ka Insurance: Kotak Proposal FormDocument6 pagesFaidey Ka Insurance Faidey Ka Insurance: Kotak Proposal FormankitrohillaNo ratings yet
- Nami ResourceDocument1 pageNami Resourceapi-578365819No ratings yet
- Thesis Statement Breastfeeding in PublicDocument5 pagesThesis Statement Breastfeeding in Publicafkntwbla100% (2)