Download as pdf or txt
You might also like
- Kenneth E. Bruscia-Defining Music Therapy-Barcelona Pub (2014) PDFDocument422 pagesKenneth E. Bruscia-Defining Music Therapy-Barcelona Pub (2014) PDFCristina Maria Oltean100% (22)
- A Student Will Lead A PrayerDocument11 pagesA Student Will Lead A PrayerEsther Joy Perez100% (3)
- Social AdjustmentDocument29 pagesSocial AdjustmentDrUsha Sharma100% (4)
- Seizures in Adults With Bacterial MeningitisDocument9 pagesSeizures in Adults With Bacterial MeningitiselaNo ratings yet
- Pyogenic Brain Abscess A 15 Year SurveryDocument10 pagesPyogenic Brain Abscess A 15 Year SurverySilvia RoseNo ratings yet
- Ambil PDF JTN 1966Document9 pagesAmbil PDF JTN 1966Naily Nuzulur RohmahNo ratings yet
- Autoimmune Causes of Encephalitis Syndrome in Thailand: Prospective Study of 103 PatientsDocument9 pagesAutoimmune Causes of Encephalitis Syndrome in Thailand: Prospective Study of 103 PatientsLily Dian AgungNo ratings yet
- 1 s2.0 S1876034117301818 Main PDFDocument5 pages1 s2.0 S1876034117301818 Main PDFdiyanNo ratings yet
- Santoso 2020Document10 pagesSantoso 2020Aldo VictoriaNo ratings yet
- Acute Demyelinating Encephalomyelitis (ADEM)Document4 pagesAcute Demyelinating Encephalomyelitis (ADEM)janeth acostaNo ratings yet
- The Causes of Postoperative Meningitis The Comparison of Gram-Negative and Gram-Positive PathogensDocument8 pagesThe Causes of Postoperative Meningitis The Comparison of Gram-Negative and Gram-Positive PathogensPietroRossidisNo ratings yet
- Neurological Sequelae Remain Frequent After Bacterial Meningitis in ChildrenDocument19 pagesNeurological Sequelae Remain Frequent After Bacterial Meningitis in ChildrenAngie WNo ratings yet
- Meningoencephalitis Infectious Etiology in Pediatric Patients at PediTRIC PASTIENTSDocument6 pagesMeningoencephalitis Infectious Etiology in Pediatric Patients at PediTRIC PASTIENTSveraNo ratings yet
- Magnetic Resonance Imaging of The Brain in Patients With Cerebral MalariaDocument10 pagesMagnetic Resonance Imaging of The Brain in Patients With Cerebral MalariaPutri Yoza KesumaNo ratings yet
- Prospective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in A Tertiary Care Pediatric SettingDocument7 pagesProspective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in A Tertiary Care Pediatric SettingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Complicaciones Neurológicas de Las Infecciones Por Rotavirus en Niños Ped Inf Dis 07 2023Document4 pagesComplicaciones Neurológicas de Las Infecciones Por Rotavirus en Niños Ped Inf Dis 07 2023ANNIX FERRERNo ratings yet
- Treatment Outcomes of Tuberculous Meningitis in Adults: A Systematic Review and Meta-AnalysisDocument11 pagesTreatment Outcomes of Tuberculous Meningitis in Adults: A Systematic Review and Meta-AnalysisGiane DavidNo ratings yet
- LiquorDocument8 pagesLiquorFanel PutraNo ratings yet
- Roberg Lars Egil Prediction of Long Term SurvivalDocument10 pagesRoberg Lars Egil Prediction of Long Term SurvivalMahmoud AbouelsoudNo ratings yet
- Incidence and Risk Factors For Seizures in Central Nervous System Infections in ChildhoodDocument6 pagesIncidence and Risk Factors For Seizures in Central Nervous System Infections in ChildhoodLiani Toniaço BellesNo ratings yet
- Diagnostic Approach To Viral Acute Encephalitis Syndrome (AES) in Paediartric Age Group - A Study From New DelhiDocument5 pagesDiagnostic Approach To Viral Acute Encephalitis Syndrome (AES) in Paediartric Age Group - A Study From New DelhiAkila SwaminathanNo ratings yet
- Ophthalmological Findings in Children With EncephalitisDocument8 pagesOphthalmological Findings in Children With EncephalitisSabila TasyakurNo ratings yet
- Infectious Dan Autoantibody Associated EncephalitisDocument13 pagesInfectious Dan Autoantibody Associated EncephalitisAyudiah ParamitaNo ratings yet
- Meningitis BacterialisDocument9 pagesMeningitis BacterialisReza OktaramaNo ratings yet
- Neurologic Cytomegalovirus Complications in Patients With Aids: Retrospective Review of 13 Cases and Review of The LiteratureDocument6 pagesNeurologic Cytomegalovirus Complications in Patients With Aids: Retrospective Review of 13 Cases and Review of The LiteratureriskyNo ratings yet
- Ref 15Document9 pagesRef 15Tiago BaraNo ratings yet
- Encephalites Aigues Infectieuses Chez Lenfant, Experience Du Service Des Maladies Infectieuses de Lhopital Denfant de RabatDocument19 pagesEncephalites Aigues Infectieuses Chez Lenfant, Experience Du Service Des Maladies Infectieuses de Lhopital Denfant de RabatIJAR JOURNALNo ratings yet
- Cryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechDocument6 pagesCryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechIJAR JOURNALNo ratings yet
- Encefalitis 2022Document10 pagesEncefalitis 2022SMIBA MedicinaNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- 149 FullDocument10 pages149 Fullসোমনাথ মহাপাত্রNo ratings yet
- Diagnosis of Cerebral Toxoplasmosis in AIDS Patients in Brazil: Importance of Molecular and Immunological Methods Using Peripheral Blood SamplesDocument4 pagesDiagnosis of Cerebral Toxoplasmosis in AIDS Patients in Brazil: Importance of Molecular and Immunological Methods Using Peripheral Blood SamplesinezlithaNo ratings yet
- FMZ 020Document6 pagesFMZ 020octawyanaNo ratings yet
- Pi Is 1201971213002142Document5 pagesPi Is 1201971213002142melisaberlianNo ratings yet
- 1gorgan BrainAbcessesDocument8 pages1gorgan BrainAbcessesGema Rizki PratamaNo ratings yet
- Presentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalDocument15 pagesPresentation, Etiology, and Outcome of Brain Infections in An Indonesian HospitalANISA RIFKA RIDHONo ratings yet
- 72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientDocument7 pages72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientFaras ArinalNo ratings yet
- International Journal of Infectious DiseasesDocument6 pagesInternational Journal of Infectious DiseasesQuỳnh Nguyễn Thị NhưNo ratings yet
- CE Update: Wegener's Granulomatosis: A Review of The Clinical Implications, Diagnosis, and TreatmentDocument3 pagesCE Update: Wegener's Granulomatosis: A Review of The Clinical Implications, Diagnosis, and TreatmentAfif FaiziNo ratings yet
- ORATORIO Ocrelizumab EMPPDocument12 pagesORATORIO Ocrelizumab EMPPalmarazneurologiaNo ratings yet
- Bacterial Brain Abscess: An Outline For Diagnosis and ManagementDocument10 pagesBacterial Brain Abscess: An Outline For Diagnosis and ManagementWIWI HRNo ratings yet
- Encephalitis: Diagnosis, Management and Recent Advances in The Field of EncephalitidesDocument10 pagesEncephalitis: Diagnosis, Management and Recent Advances in The Field of EncephalitidesPerlaNo ratings yet
- Rapid Detection of Bacterial Meningitis Using A Point-Of-Care GlucometerDocument6 pagesRapid Detection of Bacterial Meningitis Using A Point-Of-Care GlucometerSerque777No ratings yet
- Sun 2012Document6 pagesSun 2012ntnquynhproNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- AygunDocument5 pagesAygunotheasNo ratings yet
- A Thesis Proposal Submitted in Partial Fulfillment For The Requirements of MD inDocument13 pagesA Thesis Proposal Submitted in Partial Fulfillment For The Requirements of MD inMohamed HassanNo ratings yet
- Definite (Microbiologically Confirmed) Tuberculous Meningitis: Predictors and Prognostic ImpactDocument7 pagesDefinite (Microbiologically Confirmed) Tuberculous Meningitis: Predictors and Prognostic ImpactAngelica Maria Rueda SerranoNo ratings yet
- Outcome in Patients With Bacterial Meningitis Presenting With A Minimal Glasgow Coma Scale ScoreDocument24 pagesOutcome in Patients With Bacterial Meningitis Presenting With A Minimal Glasgow Coma Scale ScoreYuki Fitria Ma'atisyaNo ratings yet
- Current Epidemiological Trends of Brain Abscess: A Clinicopathological StudyDocument9 pagesCurrent Epidemiological Trends of Brain Abscess: A Clinicopathological StudyNur Fadhilah KusnadiNo ratings yet
- Acta Med Iran 2013 51 2 113 118 PDFDocument6 pagesActa Med Iran 2013 51 2 113 118 PDFbreNo ratings yet
- Community Acuired Bactarial MeningitisDocument16 pagesCommunity Acuired Bactarial Meningitisidno1008No ratings yet
- Diagnostic Value of Cytological and Microbiological Methods in Cryptococcal MeningitisDocument9 pagesDiagnostic Value of Cytological and Microbiological Methods in Cryptococcal MeningitisAngelica Maria Rueda SerranoNo ratings yet
- Prognostic Factors of Guillain-Barré Syndrome: A 111-Case Retrospective ReviewDocument9 pagesPrognostic Factors of Guillain-Barré Syndrome: A 111-Case Retrospective ReviewdzakiyahNo ratings yet
- Brucellosis DCDocument6 pagesBrucellosis DCbrahim brahimNo ratings yet
- Archneuro 55 199 PDFDocument6 pagesArchneuro 55 199 PDFAdam MochtarNo ratings yet
- Clinical Features, Etiologies, and Outcomes in Adult Patients WithDocument13 pagesClinical Features, Etiologies, and Outcomes in Adult Patients Withagarrido2No ratings yet
- 1 s2.0 S0165587617302975 Main PDFDocument4 pages1 s2.0 S0165587617302975 Main PDFAchmad YunusNo ratings yet
- Case Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of ViewDocument4 pagesCase Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of Viewzefri suhendarNo ratings yet
- Tuberculous Meningitis Review 2010Document16 pagesTuberculous Meningitis Review 2010SERGIO LOBATO FRANÇANo ratings yet
- 12 11 PBDocument168 pages12 11 PBYS NateNo ratings yet
- HHS Public Access: Author ManuscriptDocument22 pagesHHS Public Access: Author ManuscriptNathaly LapoNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Hansen 2019Document19 pagesHansen 2019Prima YosiNo ratings yet
- Clinical Presentation of Childhood Leukaemia: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Presentation of Childhood Leukaemia: A Systematic Review and Meta-AnalysisPrima YosiNo ratings yet
- 10 1016@j Arcmed 2016 11 017Document8 pages10 1016@j Arcmed 2016 11 017Prima YosiNo ratings yet
- G IEE6 Fap HLH S52 VGANBe 1634959083Document34 pagesG IEE6 Fap HLH S52 VGANBe 1634959083Prima YosiNo ratings yet
- 0306s410 PDFDocument2 pages0306s410 PDFPrima YosiNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireSaberAliNo ratings yet
- Analyzing The Curriculum by George J. Posner 25-54Document31 pagesAnalyzing The Curriculum by George J. Posner 25-54ahlamNo ratings yet
- Laboratorios Valores EndocrinoDocument88 pagesLaboratorios Valores EndocrinoS ONo ratings yet
- Aggerholm Et Al (2011) Conceptualising Employer Branding in Sustainable OrganizationsDocument19 pagesAggerholm Et Al (2011) Conceptualising Employer Branding in Sustainable OrganizationsIris LeNo ratings yet
- OSH Roles and Responsibilities ProcedureDocument10 pagesOSH Roles and Responsibilities ProcedureSanjeet SinghNo ratings yet
- Conducting Drop Object Inspection - RA-R9-01-017-01Document1 pageConducting Drop Object Inspection - RA-R9-01-017-01cmrig74No ratings yet
- Operational Guidelines On The Implementation of Face-To-Face Learning Modality Deped-Doh JMC No. 1 S. 2021Document36 pagesOperational Guidelines On The Implementation of Face-To-Face Learning Modality Deped-Doh JMC No. 1 S. 2021Jerlyn BeltranNo ratings yet
- J Cachexia Sarcopenia Muscle - 2022 - Paval - A Systematic Review Examining The Relationship Between Cytokines and CachexiaDocument15 pagesJ Cachexia Sarcopenia Muscle - 2022 - Paval - A Systematic Review Examining The Relationship Between Cytokines and CachexiaYohana Elisabeth GultomNo ratings yet
- ANAPHYSIODocument2 pagesANAPHYSIOEli AyaseNo ratings yet
- Freemrcogpart 2Document3 pagesFreemrcogpart 2Konstantinos Papadakis33% (3)
- 0 Material Safety Data Sheet: Benzene MSDSDocument6 pages0 Material Safety Data Sheet: Benzene MSDSAli RazaNo ratings yet
- USGBC-Health Anthology ReportDocument39 pagesUSGBC-Health Anthology ReportnoveNo ratings yet
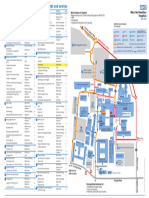
- WGH Site MapDocument1 pageWGH Site MapLuizaNo ratings yet
- Textbook Chitosan Based Biomaterials Volume 1 Fundamentals 1St Edition Jessica Amber Jennings Ebook All Chapter PDFDocument53 pagesTextbook Chitosan Based Biomaterials Volume 1 Fundamentals 1St Edition Jessica Amber Jennings Ebook All Chapter PDFalton.jemison102100% (19)
- What Is VAWC (Violence Against Women and Their Children) ?Document7 pagesWhat Is VAWC (Violence Against Women and Their Children) ?Betson Cajayon100% (1)
- Safety and CareDocument4 pagesSafety and CarePrince K. TaileyNo ratings yet
- A Real Time Case Study - The Training Manager PDFDocument2 pagesA Real Time Case Study - The Training Manager PDFUsha SinghNo ratings yet
- Research ProjectsDocument2 pagesResearch Projectsapi-143464694No ratings yet
- The Impact of Exercise On Stress Levels in Grade 10 Students of Eusebio High SchoolDocument8 pagesThe Impact of Exercise On Stress Levels in Grade 10 Students of Eusebio High SchoolCeejee PaulinNo ratings yet
- Cactus Grandiflorus: 15. MIND - CHEERFUL - Heart Disease With 1Document5 pagesCactus Grandiflorus: 15. MIND - CHEERFUL - Heart Disease With 1ubirajara3fernandes3No ratings yet
- Kes Pencemaran Udara Di DuniaDocument10 pagesKes Pencemaran Udara Di DuniaDannesa ValenciaNo ratings yet
- Health Guard Proposal Form PrintDocument4 pagesHealth Guard Proposal Form Printrock_on_rupz99No ratings yet
- Sex Offender ModuleDocument28 pagesSex Offender ModuleMona Azura IsmailNo ratings yet
- CPSP Dissertation Topics ListDocument6 pagesCPSP Dissertation Topics ListWriteMyPaperCheapBillings100% (1)
- SilosDocument3 pagesSilosapi-548205221100% (1)
- NURSING CARE PLAN RealDocument3 pagesNURSING CARE PLAN RealJorossMabantaMarayanNo ratings yet
- Quali Happy Thursday Final Blando Santos TankimDocument51 pagesQuali Happy Thursday Final Blando Santos TankimMark Blando100% (1)