Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Substance AbuseDocument87 pagesSubstance AbuseJayselle Arvie100% (1)
- JJGR v1 1004Document5 pagesJJGR v1 1004laurencia aliminNo ratings yet
- Gorfinkel 2020 Oi 200521 1596736886.419Document11 pagesGorfinkel 2020 Oi 200521 1596736886.419laurencia aliminNo ratings yet
- Self Isolation A Significant Contributor To Cannabis Use During The COVID 19 PandemicDocument5 pagesSelf Isolation A Significant Contributor To Cannabis Use During The COVID 19 Pandemiclaurencia aliminNo ratings yet
- Impact of Acute and Chronic Cannabis Use On Stress Response Regulation: Challenging The Belief That Cannabis Is An Effective Method For CopingDocument11 pagesImpact of Acute and Chronic Cannabis Use On Stress Response Regulation: Challenging The Belief That Cannabis Is An Effective Method For Copinglaurencia aliminNo ratings yet
- Cannabis and Covid 19 Reason ForDocument6 pagesCannabis and Covid 19 Reason Forlaurencia aliminNo ratings yet
- Enteral Vitamin A For Reducing Severity of Bronchopulmonary Dysplasia: A Randomized TrialDocument12 pagesEnteral Vitamin A For Reducing Severity of Bronchopulmonary Dysplasia: A Randomized Triallaurencia aliminNo ratings yet
- ASG Superconductors Paramed MRI UnitDocument27 pagesASG Superconductors Paramed MRI UnitedelNo ratings yet
- My Research ProposalDocument10 pagesMy Research ProposaloptometrynepalNo ratings yet
- Cology 3 Unit 1Document28 pagesCology 3 Unit 1imrujlaskar111No ratings yet
- Introduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences BangaloreDocument86 pagesIntroduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences Bangaloreprathyoosha baskaran100% (1)
- Early Victims of X-Rays: A Tribute and Current PerceptionDocument3 pagesEarly Victims of X-Rays: A Tribute and Current PerceptionFlávio Augusto SoaresNo ratings yet
- MeningitisDocument34 pagesMeningitispriska maniesNo ratings yet
- Rec Letter From ZhylkybaevaDocument2 pagesRec Letter From ZhylkybaevaГулнара УмурзаковаNo ratings yet
- Commonly Used Drugs in The ERDocument2 pagesCommonly Used Drugs in The ERsberry522No ratings yet
- Breast Surgeon in Pune - Dr. Swati SuradkarDocument8 pagesBreast Surgeon in Pune - Dr. Swati SuradkarSwati SuradkarNo ratings yet
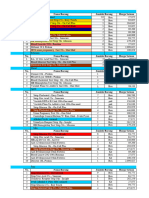
- BELANJA BHP Medis SinarindoDocument183 pagesBELANJA BHP Medis SinarindowerryNo ratings yet
- Goodman and Gilman39s Manual of Pharmacology and Therapeutics Latest EditionDocument3 pagesGoodman and Gilman39s Manual of Pharmacology and Therapeutics Latest EditionLinda0% (1)
- Auras Epilépticas: Clasificación, Fisiopatología, Utilidad Práctica, Diagnóstico Diferencial y ControversiasDocument7 pagesAuras Epilépticas: Clasificación, Fisiopatología, Utilidad Práctica, Diagnóstico Diferencial y ControversiasMartinAnteparraNo ratings yet
- Product Development Pipeline - FebruaryDocument4 pagesProduct Development Pipeline - FebruaryCebin VargheseNo ratings yet
- Postoperative Nursing ManagementDocument12 pagesPostoperative Nursing ManagementAhmed AliNo ratings yet
- Molecular Imaging: Shrikant NagareDocument4 pagesMolecular Imaging: Shrikant NagareAshish Mohan BhattaraiNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearanceChristineAlaNo ratings yet
- Anti Allergic DrugsDocument18 pagesAnti Allergic Drugsaamer niaziNo ratings yet
- Lymphangitis TreatmentDocument2 pagesLymphangitis TreatmentHarista Miranda SalamNo ratings yet
- ExplanationDocument8 pagesExplanationmarisa dwilestariNo ratings yet
- Forms of Nimesulide..ArtDocument5 pagesForms of Nimesulide..ArtKimberly RiceNo ratings yet
- Blunt AbdominalDocument39 pagesBlunt AbdominalIgnatius JesinNo ratings yet
- Cholera and SalmonellaDocument5 pagesCholera and SalmonellaJonas Marvin Anaque100% (1)
- Physical Education 11: Active Lifestyle For WellnessDocument24 pagesPhysical Education 11: Active Lifestyle For Wellnesshatdognamalaki100% (2)
- Analysource Report 20210112012628Document37 pagesAnalysource Report 20210112012628Vijaya AgrawaNo ratings yet
- Concept Map - Colon CancerDocument2 pagesConcept Map - Colon Cancerbea pegadNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2020 Pediatric SurgeryDocument15 pagesInformation MSQ KROK 2 Medicine 2007 2020 Pediatric SurgeryReshma Shaji PnsNo ratings yet
- Lesson Plan Lumbar PunctureDocument19 pagesLesson Plan Lumbar PunctureLoma Waghmare (Jadhav)No ratings yet
- A Basic Overview On Transdermal Drug Delivery SystemDocument9 pagesA Basic Overview On Transdermal Drug Delivery SystemEditor IJTSRDNo ratings yet
- Uji Sensitivitas Bakteri Shigella Sp. Terhadap Antibiotik Golongan Sulfonamida, Beta-Laktam, Dan Makrolida TAHUN 2017Document11 pagesUji Sensitivitas Bakteri Shigella Sp. Terhadap Antibiotik Golongan Sulfonamida, Beta-Laktam, Dan Makrolida TAHUN 2017Alexankim xanNo ratings yet