Download as pdf or txt
You might also like
- Squeezed by Alissa Quart "Why Our Families Can't Afford America"Document6 pagesSqueezed by Alissa Quart "Why Our Families Can't Afford America"Zahra AfikahNo ratings yet
- RS ARI-Common Cold - PPT 93Document57 pagesRS ARI-Common Cold - PPT 93Dr.P.NatarajanNo ratings yet
- MPI Painting CodeDocument28 pagesMPI Painting CodeGhayas JawedNo ratings yet
- MeaslesDocument20 pagesMeaslesTinde KumarNo ratings yet
- Common Pediatric InfectionsDocument26 pagesCommon Pediatric Infectionsfreelancer.am1302No ratings yet
- DDs of Fever With RashDocument18 pagesDDs of Fever With RashEBNo ratings yet
- Fever and RashDocument120 pagesFever and RashsamaNo ratings yet
- Viral Infections Part 1 by Nicolle Ann Pancho (Pediatrics Rotation)Document67 pagesViral Infections Part 1 by Nicolle Ann Pancho (Pediatrics Rotation)Nicolle PanchoNo ratings yet
- Fever and Rash - StudentsDocument117 pagesFever and Rash - StudentsAishath Mizna MOOSA 17-2-00902No ratings yet
- MeaslesDocument33 pagesMeaslesObi EmereuwaNo ratings yet
- Enterovirus & PoliomyelitisDocument17 pagesEnterovirus & PoliomyelitisAbdulsalam HashiNo ratings yet
- DiphtheriaDocument37 pagesDiphtheriaeuniicehahaNo ratings yet
- MeaslesDocument14 pagesMeaslesCHALIE MEQUNo ratings yet
- The Acutely Ill Patient With Fever and Rash Department of Microbiology Micro II-643 Infectious Diseases Victoria Michelen, MDDocument49 pagesThe Acutely Ill Patient With Fever and Rash Department of Microbiology Micro II-643 Infectious Diseases Victoria Michelen, MDFelito SifonteNo ratings yet
- PICORNAVIRUSDocument20 pagesPICORNAVIRUStejasbhukal567No ratings yet
- JURNAL Update Terapy MycosesDocument16 pagesJURNAL Update Terapy MycosesShania EvingelindaNo ratings yet
- Enteroviral InfectionsDocument32 pagesEnteroviral InfectionsTarik PlojovicNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- Viral InfectionDocument36 pagesViral InfectionHani El-asferNo ratings yet
- Measles: Symptoms, Treatment and Prevention: BY: JO1 Harold Jake Arguelles, RN Unit NurseDocument20 pagesMeasles: Symptoms, Treatment and Prevention: BY: JO1 Harold Jake Arguelles, RN Unit NurseTacloban City Jail-MD Health Service UnitNo ratings yet
- Espiratory Infections BitseatDocument90 pagesEspiratory Infections BitseatAhmed KitawNo ratings yet
- Vaccine Preventable DiseaseDocument72 pagesVaccine Preventable Diseasemehdikhalid09No ratings yet
- Disturbances in Inflammatory and ImmunologyDocument89 pagesDisturbances in Inflammatory and ImmunologyAubrey RafadaNo ratings yet
- Acutemeningoencephalitis 170309112245Document41 pagesAcutemeningoencephalitis 170309112245jinsi georgeNo ratings yet
- Infectious DiseaseDocument120 pagesInfectious Diseaseapi-3722655100% (2)
- Measles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanDocument16 pagesMeasles: Rubeola or Morbilli Department of Infectious Disease Wang JingyankatsukagemaruNo ratings yet
- Measles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanDocument16 pagesMeasles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanDhruvil SutharNo ratings yet
- Rubella: Prepared and Presented by Ibrahim Ali Assiri 439106123Document21 pagesRubella: Prepared and Presented by Ibrahim Ali Assiri 439106123عادل حكميNo ratings yet
- 18 DifteriaDocument25 pages18 DifteriaSheryl ElitaNo ratings yet
- Epidemic Typhus: by Dr. Addisu T. (MD, Internist) July, 08,2015Document14 pagesEpidemic Typhus: by Dr. Addisu T. (MD, Internist) July, 08,2015Mebratu DemessNo ratings yet
- Varicella Zoster VirusDocument33 pagesVaricella Zoster VirusJane GreenNo ratings yet
- Measles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanDocument16 pagesMeasles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanVipul MehlaNo ratings yet
- Small Animal MedicineDocument262 pagesSmall Animal Medicinelijyohannesmekonnen7No ratings yet
- Infectious DiseaseDocument9 pagesInfectious DiseaseST AYAN PRO GAMERNo ratings yet
- MeaslesDocument16 pagesMeaslesdepan_dkb32No ratings yet
- Positive Stranded RNA VirusesDocument29 pagesPositive Stranded RNA VirusesNovie Carla GayosaNo ratings yet
- Dengue Fever GuanDocument92 pagesDengue Fever GuanWai Kwong ChiuNo ratings yet
- SGD Case Presentation 8Document34 pagesSGD Case Presentation 8Karen C. Del Rosario100% (1)
- Childhood Tuberculosis: Robert KochDocument46 pagesChildhood Tuberculosis: Robert KochDr.P.NatarajanNo ratings yet
- Communicable Diseases PowerPoint - StudentDocument15 pagesCommunicable Diseases PowerPoint - StudentCruz YrNo ratings yet
- Measles: PGI Nicole Jenne C. TanDocument40 pagesMeasles: PGI Nicole Jenne C. TanNicole Jenne TanNo ratings yet
- Kuliah Respi Bakteri TDK Lazim Revisi TambahanDocument23 pagesKuliah Respi Bakteri TDK Lazim Revisi TambahanIzza Ayudia HakimNo ratings yet
- Herpes, Pox, Rhabdo, Arena VIRUSDocument7 pagesHerpes, Pox, Rhabdo, Arena VIRUSErnie G. Bautista II, RN, MDNo ratings yet
- Paediatric Rashes: Ali Faisal SaleemDocument51 pagesPaediatric Rashes: Ali Faisal Saleemarjumand100% (3)
- MeningitisDocument7 pagesMeningitis47rqmgyt2xNo ratings yet
- Dengue Fever: WHO Dengue: Guidelines For Diagnosis, Treatment, Prevention and ControlDocument16 pagesDengue Fever: WHO Dengue: Guidelines For Diagnosis, Treatment, Prevention and ControlKailash KhatriNo ratings yet
- Infectious DiseasesDocument140 pagesInfectious DiseasesSamah IzzNo ratings yet
- Reckettsia and ChlamediaDocument37 pagesReckettsia and ChlamediaMuqtadir “The Ruler” KuchikiNo ratings yet
- Mumps - Nguyen Thi Ngoc ThamDocument32 pagesMumps - Nguyen Thi Ngoc Thamnguyenthingoctham1208No ratings yet
- Viral Infections - Derma ReportDocument40 pagesViral Infections - Derma ReportgeorgeNo ratings yet
- PI Virus (Enterovirus and Rhinovirus Groups)Document34 pagesPI Virus (Enterovirus and Rhinovirus Groups)Lovryan Tadena AmilingNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- RubellaDocument29 pagesRubellaRose PeranteNo ratings yet
- Otologic Manifestation of Systemic DiseaseDocument57 pagesOtologic Manifestation of Systemic DiseaseHERIZALNo ratings yet
- Measles, Mumps, RubellaDocument25 pagesMeasles, Mumps, RubellaRohit KumarNo ratings yet
- Orthomyxovirus.12&13Document20 pagesOrthomyxovirus.12&13Divya DharshiniNo ratings yet
- This Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Document62 pagesThis Child Has Had A Sore Throat and Fever For 3 Days. The Appearance of The Throat Is Shown. What Do You See?Ivan KurniawanNo ratings yet
- Communicable DiseasesDocument6 pagesCommunicable DiseasesLory LynNo ratings yet
- MEASLESDocument26 pagesMEASLESprasanna lamaNo ratings yet
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDocument28 pages3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaNo ratings yet
- Infectious DiseaseDocument43 pagesInfectious DiseaseHani El-asferNo ratings yet
- Measles: Introduction: - Highly Contagious VirusDocument14 pagesMeasles: Introduction: - Highly Contagious VirusPrabhat RanjanNo ratings yet
- Endocrinology Adreno Genital SyndromeDocument29 pagesEndocrinology Adreno Genital SyndromeDr.P.NatarajanNo ratings yet
- GIT Viral Hepatitis in Children - PPT 93Document22 pagesGIT Viral Hepatitis in Children - PPT 93Dr.P.NatarajanNo ratings yet
- CNS Seizures in ChildhoodDocument42 pagesCNS Seizures in ChildhoodDr.P.NatarajanNo ratings yet
- Cns Neurological ExaminationDocument26 pagesCns Neurological ExaminationDr.P.NatarajanNo ratings yet
- GIT Examination of AbdomenDocument63 pagesGIT Examination of AbdomenDr.P.NatarajanNo ratings yet
- GIT Portal HypertensionDocument24 pagesGIT Portal HypertensionDr.P.NatarajanNo ratings yet
- GIT Cirrhosis Liver in ChildrenDocument37 pagesGIT Cirrhosis Liver in ChildrenDr.P.NatarajanNo ratings yet
- Rs Wheeze in ChildrenDocument44 pagesRs Wheeze in ChildrenDr.P.NatarajanNo ratings yet
- Rs Foreign Body AspirationDocument50 pagesRs Foreign Body AspirationDr.P.NatarajanNo ratings yet
- Rs PleurisyDocument32 pagesRs PleurisyDr.P.NatarajanNo ratings yet
- Wet RisersDocument3 pagesWet RisersNur Amirah Abdul JamilNo ratings yet
- Bio-Organic Chem LecturesDocument205 pagesBio-Organic Chem LecturesРаони Мессиас100% (2)
- Why Aws Is Even Better With CloudcheckrDocument7 pagesWhy Aws Is Even Better With CloudcheckrPardha SaradhiNo ratings yet
- Benzene - It'S Characteristics and Safety in Handling, Storing & TransportationDocument6 pagesBenzene - It'S Characteristics and Safety in Handling, Storing & TransportationEhab SaadNo ratings yet
- ..Document11 pages..Rizka Nur FadhilahNo ratings yet
- Bibliography Primary Sources: Books:: Marie-Curie-Speech - HTMLDocument11 pagesBibliography Primary Sources: Books:: Marie-Curie-Speech - HTMLapi-130099490No ratings yet
- IPC in Family PlanningDocument12 pagesIPC in Family PlanningHari MurtiNo ratings yet
- Bence Bays Resume July 2015Document2 pagesBence Bays Resume July 2015api-292242662No ratings yet
- Group3 Dilemmac pr6031Document8 pagesGroup3 Dilemmac pr6031api-576539858No ratings yet
- Microbiology 101: Laboratory Exercise #22: Carbohydrate MetabolismDocument16 pagesMicrobiology 101: Laboratory Exercise #22: Carbohydrate Metabolismmaraki998No ratings yet
- Exploded View & Parts Listing Air Operated Double Diaphragm PumpDocument3 pagesExploded View & Parts Listing Air Operated Double Diaphragm PumpEdgar NercarNo ratings yet
- India Bulls Housing Finance LimitedDocument67 pagesIndia Bulls Housing Finance LimitedslohariNo ratings yet
- Busbar Protect1Document9 pagesBusbar Protect1syahira87No ratings yet
- OSH SeminarDocument2 pagesOSH SeminarSahar Ulu JeruasNo ratings yet
- Physician'S Order/Progress Notes: 23 S. Avila Male JhonDocument2 pagesPhysician'S Order/Progress Notes: 23 S. Avila Male JhonKrizha Angela Nicolas100% (1)
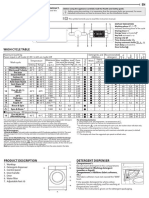
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Ramsay Health Care - BudgetDocument13 pagesRamsay Health Care - BudgetTatiana Garcia MendozaNo ratings yet
- Like Water For Chocolate QuestionsDocument2 pagesLike Water For Chocolate Questionslde918No ratings yet
- Aisyah Fadiyah - SPEECH DRAFTDocument5 pagesAisyah Fadiyah - SPEECH DRAFTAisyah FawNo ratings yet
- PhilRice - Fertilizer CalculationDocument21 pagesPhilRice - Fertilizer CalculationMichelle Ann SoledadNo ratings yet
- 1.1 - Monitor de Aterramento - 8030Document2 pages1.1 - Monitor de Aterramento - 8030Denis MarcosNo ratings yet
- Capinew Account June13Document7 pagesCapinew Account June13ashwinNo ratings yet
- II 2015 4Document283 pagesII 2015 4tuni santeNo ratings yet
- An International Cohort Study of Cancer in Systemic Lupus ErythematosusDocument10 pagesAn International Cohort Study of Cancer in Systemic Lupus ErythematosusCristina TudorNo ratings yet
- Catálogo de Referencias - Power Conversion SystemsDocument60 pagesCatálogo de Referencias - Power Conversion SystemsBENo ratings yet
- 555-Timer AStable and MonostableDocument13 pages555-Timer AStable and MonostableenzuekNo ratings yet
- Implications of Operating Boilers at Lower Pressures Than Design PressureDocument2 pagesImplications of Operating Boilers at Lower Pressures Than Design PressureAu TagolimotNo ratings yet
- Product Manual 26361V1 (Revision F) : 505DE Digital Governor For Steam TurbinesDocument198 pagesProduct Manual 26361V1 (Revision F) : 505DE Digital Governor For Steam TurbinesGuilherme Marquezin100% (1)