Download as doc, pdf, or txt
You might also like
- SILVA Ultramind Esp System WorkbookDocument75 pagesSILVA Ultramind Esp System WorkbookLingua Star100% (1)
- Self-Learning Module Unit 3 Physical AssessmentDocument57 pagesSelf-Learning Module Unit 3 Physical AssessmentMarlon Glorioso IINo ratings yet
- BDD YBOCS Adult PDFDocument6 pagesBDD YBOCS Adult PDFdruzair007No ratings yet
- Body Posture QuestionnaireDocument4 pagesBody Posture QuestionnaireKhairul Faiz50% (2)
- Non Deliverable ForwardDocument17 pagesNon Deliverable ForwardManish GuptaNo ratings yet
- Johnston (1999) Why We Feel. The Science of Human EmotionsDocument221 pagesJohnston (1999) Why We Feel. The Science of Human EmotionsNavi Setnom ArieugonNo ratings yet
- Physical Residual Functional Capacity ReportDocument7 pagesPhysical Residual Functional Capacity ReportDellComputer99No ratings yet
- RFC 2009 Physical With Onset Four PageDocument4 pagesRFC 2009 Physical With Onset Four PagedrewhobbieNo ratings yet
- Chronic Fatigue Syndrome Mss 1Document5 pagesChronic Fatigue Syndrome Mss 1Anika OkjeNo ratings yet
- Index Disability NeckDocument9 pagesIndex Disability NeckCarolina Bejarano GonzalezNo ratings yet
- RFC Form (Physical)Document2 pagesRFC Form (Physical)dvolmy321No ratings yet
- Department of Education: ExploreDocument4 pagesDepartment of Education: ExploreRuben Rosendal De AsisNo ratings yet
- Stress Management Module 2Document17 pagesStress Management Module 2Jerome Mallari PacsonNo ratings yet
- PE Protocol With Details PDFDocument7 pagesPE Protocol With Details PDFDominic SloanNo ratings yet
- Questionnaire Misab 2Document6 pagesQuestionnaire Misab 2Misab MKNo ratings yet
- Individualized Treatment Plan FW 1Document3 pagesIndividualized Treatment Plan FW 1api-365255082100% (1)
- Personal Development Causes and Effects of Stress: Quarter 1 - Module 9Document14 pagesPersonal Development Causes and Effects of Stress: Quarter 1 - Module 9Elvira DagalangitNo ratings yet
- Module 4: Case Conceptualization and Treatment Planning: ObjectivesDocument6 pagesModule 4: Case Conceptualization and Treatment Planning: ObjectivesMaria BagourdiNo ratings yet
- Residual Functional Capacit Questionnaire: Pati NT Stne ST E Dob: S 565-56-5651Document3 pagesResidual Functional Capacit Questionnaire: Pati NT Stne ST E Dob: S 565-56-5651loginmuraliNo ratings yet
- Checks For Fidelity of Therapy SOP For Each Session in The Integrated Cognitive Control TherapyDocument5 pagesChecks For Fidelity of Therapy SOP For Each Session in The Integrated Cognitive Control Therapymahashweta bhattacharyaNo ratings yet
- HMMM PEDocument11 pagesHMMM PEJessa May SanchezNo ratings yet
- Cns 771 Assignment - Assignment 3Document6 pagesCns 771 Assignment - Assignment 3api-709765074No ratings yet
- Focusing Motivation Course BookletDocument14 pagesFocusing Motivation Course BookletjasonNo ratings yet
- Stress Management PlanDocument12 pagesStress Management PlanDuc DangNo ratings yet
- PSP - FinalDocument4 pagesPSP - Finalapi-242367576No ratings yet
- NCP q4Document1 pageNCP q4Kathleen PabalanNo ratings yet
- Pilar College of Zamboanga City, IncDocument14 pagesPilar College of Zamboanga City, IncIvy VillalobosNo ratings yet
- Lesson 1Document17 pagesLesson 1Solo SegalNo ratings yet
- q3 Shs Hope 2 - Module 1Document13 pagesq3 Shs Hope 2 - Module 1Hope JamestownNo ratings yet
- Pott's Disease NCPDocument30 pagesPott's Disease NCPmrscribd12No ratings yet
- Module 9 UNIT 4Document24 pagesModule 9 UNIT 4bassem djediNo ratings yet
- Bdd-Ybocs-Adult 230629 161624Document7 pagesBdd-Ybocs-Adult 230629 161624Pankhuri MishraNo ratings yet
- Liz Big Assign 2Document5 pagesLiz Big Assign 2api-266278027No ratings yet
- 11 - NCPsDocument6 pages11 - NCPsellian3leiNo ratings yet
- Mental Health RoutineDocument8 pagesMental Health Routinemorella figueraNo ratings yet
- Unit 6Document15 pagesUnit 6RAGHAV DIXITNo ratings yet
- LP RevisedDocument15 pagesLP Revisedjaneth banaagNo ratings yet
- Guided VisualizationDocument4 pagesGuided VisualizationAris Kendell BungabongNo ratings yet
- Warriors Path Systema - Keep Calm and Be Resilient October - 2014aDocument9 pagesWarriors Path Systema - Keep Calm and Be Resilient October - 2014awhitou100% (1)
- Hope - 1 Grade 11: 60 Minutes AerobicDocument9 pagesHope - 1 Grade 11: 60 Minutes AerobicDonajei RicaNo ratings yet
- Part A Unit 2 IT SelfManagement SkillsDocument39 pagesPart A Unit 2 IT SelfManagement SkillsJaifray BalwanNo ratings yet
- NCPDocument3 pagesNCPbjhilario100% (1)
- ACEDS Course Reflection PointsDocument7 pagesACEDS Course Reflection PointsNicole Tamsyn GriloNo ratings yet
- Relaxation Skills For AnxietyDocument15 pagesRelaxation Skills For AnxietyAnamaria Rosca100% (1)
- Relaxation Skills For Anxiety PDFDocument15 pagesRelaxation Skills For Anxiety PDFDomingo de Leon100% (1)
- Stress Management: Session Duration: 1h-1.5hDocument10 pagesStress Management: Session Duration: 1h-1.5hKrishna GavaliNo ratings yet
- Modules in P.E & HealthDocument17 pagesModules in P.E & HealthApryll Anne EdadesNo ratings yet
- PE and Health 12 2nd QTRDocument48 pagesPE and Health 12 2nd QTRXian Guzman100% (1)
- PE101.Module 1.lesson1. Component of HealthDocument9 pagesPE101.Module 1.lesson1. Component of HealthRoen Shane RamonalNo ratings yet
- G10 Q2 PE Module 6 - For Reg - L EditingDocument14 pagesG10 Q2 PE Module 6 - For Reg - L EditingSALGIE SERNALNo ratings yet
- DLP-FinalFinal-StressManagemnt (Week 4)Document5 pagesDLP-FinalFinal-StressManagemnt (Week 4)Sheryl PerezNo ratings yet
- Part A Unit 2 Self Management Skills Unsolved Questions SolvedDocument5 pagesPart A Unit 2 Self Management Skills Unsolved Questions SolvedAnkit MazumdarNo ratings yet
- Growth and Development Lesson 2: Management of Health Concerns During PubertyDocument6 pagesGrowth and Development Lesson 2: Management of Health Concerns During PubertyZannedelle Espina GonzalesNo ratings yet
- Lecture 9 Stress MGTDocument8 pagesLecture 9 Stress MGTsaikukhanNo ratings yet
- H O P E: Ealth Ptimizing Hysical Ducation 3Document23 pagesH O P E: Ealth Ptimizing Hysical Ducation 3Rokcyne Nage RobusNo ratings yet
- P.E and Health: First Quarter - Week 1 Health-Related Fitness ComponentsDocument19 pagesP.E and Health: First Quarter - Week 1 Health-Related Fitness ComponentsNeil John ArmstrongNo ratings yet
- 4cm Final YayDocument12 pages4cm Final Yayapi-518621879No ratings yet
- Nursing Care Plan NCP Group 3 Fatigue ..Document2 pagesNursing Care Plan NCP Group 3 Fatigue ..Aerron Severus Secano ShuldbergNo ratings yet
- 1 - H7GD Ia 12Document2 pages1 - H7GD Ia 12Sarah mae EmbalsadoNo ratings yet
- P S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care PlanDocument1 pageP S Y C H O L O G I C Need Rest and Sleep Independent:: Nursing Care Planunkown userNo ratings yet
- Assessment and Plan of Care: SOAP Notes Writing Patient Centered Functional GoalsDocument5 pagesAssessment and Plan of Care: SOAP Notes Writing Patient Centered Functional GoalsAaron James GrayNo ratings yet
- Event PreApproval Routing ChecklistDocument3 pagesEvent PreApproval Routing ChecklistDellComputer99No ratings yet
- Employer Specail Wage Report Social-Security-Form-SSA-131Document2 pagesEmployer Specail Wage Report Social-Security-Form-SSA-131DellComputer99No ratings yet
- Ss 5Document5 pagesSs 5DellComputer99No ratings yet
- Results That Have Not Been Provided Previously To The Social Security AdministrationDocument6 pagesResults That Have Not Been Provided Previously To The Social Security AdministrationDellComputer99No ratings yet
- Physical Residual Functional Capacity ReportDocument7 pagesPhysical Residual Functional Capacity ReportDellComputer99No ratings yet
- Sleep Disorders Residual Functional Capacity QuestionnaireDocument3 pagesSleep Disorders Residual Functional Capacity QuestionnaireDellComputer99No ratings yet
- Headaches Residual Functional Capacity QuestionnaireDocument3 pagesHeadaches Residual Functional Capacity QuestionnaireDellComputer99No ratings yet
- Presn. On Gen. SWRDDocument60 pagesPresn. On Gen. SWRDbijoy100% (1)
- Every Office Has OneDocument2 pagesEvery Office Has OneVeronicaGelfgrenNo ratings yet
- Software Requirement Engineering - CS708 Power Point Slides Lecture-09Document25 pagesSoftware Requirement Engineering - CS708 Power Point Slides Lecture-09ALTAIRI SALEHNo ratings yet
- 7.3-7.4 Electric Field and Potential Difference TemplateDocument11 pages7.3-7.4 Electric Field and Potential Difference TemplateAyman HalimeNo ratings yet
- Esotropia and ExotropiaDocument49 pagesEsotropia and ExotropiaEdoga Chima EmmanuelNo ratings yet
- 1 Pre-Lab: ELEC2201 Signals & Linear Systems MDocument7 pages1 Pre-Lab: ELEC2201 Signals & Linear Systems MPhilip SalmonyNo ratings yet
- Andon PDFDocument24 pagesAndon PDFFrilya Andarni Saragih SumbayakNo ratings yet
- Damper Valve - Technical Data SheetDocument1 pageDamper Valve - Technical Data SheetPinakin PatelNo ratings yet
- Questions (1-30)Document39 pagesQuestions (1-30)Khánh ToànNo ratings yet
- Recalls 10 - Np2Document6 pagesRecalls 10 - Np2Nova Clea BoquilonNo ratings yet
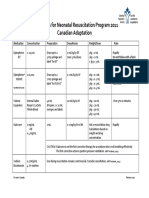
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- 3629 Structtimber1 PDFDocument33 pages3629 Structtimber1 PDFPrithwish2014No ratings yet
- General Definition of Sag and Tension in Electrical Transmission LinesDocument11 pagesGeneral Definition of Sag and Tension in Electrical Transmission Linesdskymaximus67% (3)
- Ethics in Accounting A Decision Making Approach 1St Edition Klein Solutions Manual Full Chapter PDFDocument40 pagesEthics in Accounting A Decision Making Approach 1St Edition Klein Solutions Manual Full Chapter PDFLisaMartinykfz100% (9)
- Perils of PlagiarismDocument3 pagesPerils of Plagiarismapi-306005383No ratings yet
- Psalm 127 - Overview"Document1 pagePsalm 127 - Overview"Malcolm CoxNo ratings yet
- Multiple MyelomaDocument8 pagesMultiple MyelomaFelipeNo ratings yet
- The Concept of Developmental PsychologyDocument16 pagesThe Concept of Developmental PsychologyJulie Anne ÜNo ratings yet
- EN 1993-1-12-2007 Eurocode 3  " Design of Steel Structures  " Part 1-12 Additional Rules For The Extension of EN 1993 Up To Steel Grades S 700Document12 pagesEN 1993-1-12-2007 Eurocode 3  " Design of Steel Structures  " Part 1-12 Additional Rules For The Extension of EN 1993 Up To Steel Grades S 700Gökhan Çiçek100% (1)
- SpaceX Response To DISH Re Mobile Platforms (6!8!22)Document6 pagesSpaceX Response To DISH Re Mobile Platforms (6!8!22)michaelkan1No ratings yet
- MLD 201aDocument13 pagesMLD 201aChaucer19No ratings yet
- PVC Foam Furniture Sheet PDFDocument2 pagesPVC Foam Furniture Sheet PDFAbdul Majid100% (1)
- Solución: R T β T R (T) = 1000 Ω ΩDocument6 pagesSolución: R T β T R (T) = 1000 Ω ΩDuvan BayonaNo ratings yet
- A Meta-Analysis of Motivational Interviewing Twenty-Five Years of Empirical StudiesDocument24 pagesA Meta-Analysis of Motivational Interviewing Twenty-Five Years of Empirical StudiesJavieraRamírezSánchezNo ratings yet
- Full Data AnalysisDocument627 pagesFull Data AnalysisMyMinecrafter97No ratings yet
- The Terror of Pediatric Medicine DR SircusDocument258 pagesThe Terror of Pediatric Medicine DR SircusAngel Francisco100% (1)
- Problems 1Document2 pagesProblems 1Rajiv KumarNo ratings yet
- Case Study 3 Cynar Plastics To Fuel FINALDocument8 pagesCase Study 3 Cynar Plastics To Fuel FINALtalhaNo ratings yet