
NOACs DOACs Coagulation Tests 2018nov16
NOACs DOACs Coagulation Tests 2018nov16
You might also like
- Clinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsDocument8 pagesClinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsdarekshepardNo ratings yet
- MILsgsdgds VDocument4 pagesMILsgsdgds Vgarywall.ukNo ratings yet
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Document55 pagesNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNo ratings yet
- Rivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageRomeo-Remus RaffaiNo ratings yet
- Rivaroxaban PresentationDocument13 pagesRivaroxaban PresentationReem El-HusseinyNo ratings yet
- UPDATED MalDocument52 pagesUPDATED MalABDIRAHIM ADAMNo ratings yet
- Hematologia - Hemostasia - Doacs (Jama 2018)Document2 pagesHematologia - Hemostasia - Doacs (Jama 2018)Matias FlammNo ratings yet
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDocument57 pagesNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNo ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Anticoag 2015november FullDocument14 pagesAnticoag 2015november FullRosanna FiorilloNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- AFib WarfarinVsNOACsDocument2 pagesAFib WarfarinVsNOACsalpha wolfNo ratings yet
- New Oral Anticoagulants Guidelines: Kai YapDocument23 pagesNew Oral Anticoagulants Guidelines: Kai YapMuhammad Reza FirdausNo ratings yet
- Rivaroxaban Sensitivity ThromboplastinDocument5 pagesRivaroxaban Sensitivity ThromboplastinpgdlilleNo ratings yet
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- Guidelines For Hemostasis and ThrombosisDocument4 pagesGuidelines For Hemostasis and Thrombosisjennifer acostaNo ratings yet
- 1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsDocument2 pages1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsPopov VictorNo ratings yet
- Anti CoagulantsDocument37 pagesAnti CoagulantsMaria khurshidNo ratings yet
- PredavanjeDocument54 pagesPredavanjeSnezana MihajlovicNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Angiotensin Receptor BlockersDocument6 pagesAngiotensin Receptor BlockersMohammad Arafat SiddiquiNo ratings yet
- AnticoagulantsDocument3 pagesAnticoagulantsDarNo ratings yet
- TransfusionDocument3 pagesTransfusionjulissand10No ratings yet
- S 011 LBLDocument22 pagesS 011 LBLalexandr zinchenkoNo ratings yet
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDocument23 pagesVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
- ACOS BloodDocument7 pagesACOS Bloodpablin1788No ratings yet
- Acetaminophen (APAP) ToxicityDocument12 pagesAcetaminophen (APAP) ToxicityJessa MaeNo ratings yet
- Laboratory Control of Anticoagulant Therapy - PPTX LectDocument69 pagesLaboratory Control of Anticoagulant Therapy - PPTX LectTusabe FredNo ratings yet
- Switching Between AnticoagulantsDocument2 pagesSwitching Between AnticoagulantsSylvinho46No ratings yet
- Amended Intravenous Unfractionated Heparin Recommended StandardDocument4 pagesAmended Intravenous Unfractionated Heparin Recommended StandardTOJO JOSEPH TOMNo ratings yet
- Anticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDDocument103 pagesAnticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDabhilashreddy45100% (1)
- Comparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionDocument9 pagesComparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionLolita UmarNo ratings yet
- 10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHADocument32 pages10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHAEmdan SengadjiNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- Drug Monograph ExampleDocument6 pagesDrug Monograph ExampleAaltiyaNo ratings yet
- Doac Switch Guidance Oct 2016Document1 pageDoac Switch Guidance Oct 2016RouaNo ratings yet
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Document26 pagesXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNo ratings yet
- Reversing The New AnticoagulantsDocument24 pagesReversing The New AnticoagulantsFurman BorstNo ratings yet
- Anti CoagulationDocument2 pagesAnti Coagulationsundance127No ratings yet
- Anticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectableDocument4 pagesAnticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectablepaulaNo ratings yet
- Saito 2006Document8 pagesSaito 2006cindyNo ratings yet
- EHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationDocument41 pagesEHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationAmelia Maria LasloNo ratings yet
- Anticoagulant DOACDocument39 pagesAnticoagulant DOACSukmawatiNo ratings yet
- Doacs AND LABORATORY1Document12 pagesDoacs AND LABORATORY1pasqualijNo ratings yet
- DRUGS2Document1 pageDRUGS2KaoriMarieSembranoNo ratings yet
- FAQ - DOAC in CKD Update - FinalDocument4 pagesFAQ - DOAC in CKD Update - Finalraea.dobsonNo ratings yet
- Nuevos anticoagulantes-BLOODDocument7 pagesNuevos anticoagulantes-BLOODnakroliNo ratings yet
- Anticoagulantele Si Explorarile Invazive 2021Document33 pagesAnticoagulantele Si Explorarile Invazive 2021GabrielaOaneNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
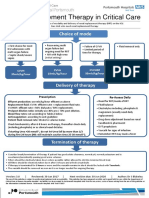
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
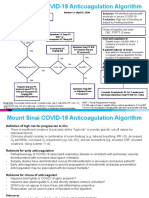
- COVID 19 Anticoagulation Algorithm Version Final 1.1Document2 pagesCOVID 19 Anticoagulation Algorithm Version Final 1.1Emi PuspitasariNo ratings yet
- Rivaroxaban (Xarelto) Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban (Xarelto) Requiring Emergency Surgery or Treatment For HaemorrhageWLC27No ratings yet
- Anticoagulation Related Bleeding - Guideline Summary: Click On The Appropriate Link BelowDocument19 pagesAnticoagulation Related Bleeding - Guideline Summary: Click On The Appropriate Link BelowIreneNo ratings yet
- Pharmacy CarbamazepineDocument21 pagesPharmacy CarbamazepineMargie dulacaNo ratings yet
- Monitoring The Traditional & The New AnticoagulantsDocument53 pagesMonitoring The Traditional & The New Anticoagulantsasclswisconsin100% (1)
- Comparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionDocument9 pagesComparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionAnna ApriyantiNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Awareness, Attitudes, Prevention, and Perceptions of COVID-19 Outbreak Among Nurses in Saudi ArabiaDocument16 pagesAwareness, Attitudes, Prevention, and Perceptions of COVID-19 Outbreak Among Nurses in Saudi ArabiaAlec AnonNo ratings yet
- PSM case-ARI-7Document23 pagesPSM case-ARI-7Amer HussainNo ratings yet
- 135th KSW Transcript EN Draft v4 PDFDocument43 pages135th KSW Transcript EN Draft v4 PDFnew lightNo ratings yet
- CPR ACLS Study GuideDocument18 pagesCPR ACLS Study GuideJohn Phamacy100% (1)
- Nutrition To You: We BringDocument64 pagesNutrition To You: We Bringjose litoNo ratings yet
- Cover Letter For Mayo ClinicDocument7 pagesCover Letter For Mayo Clinicuyyjcvvcf100% (2)
- SuperlongevityDocument3 pagesSuperlongevityVadivelan MNo ratings yet
- Recalls Kaps 2017 April 01Document7 pagesRecalls Kaps 2017 April 01Aymen BekirNo ratings yet
- A Narrative Review of Influenza: A Seasonal and Pandemic DiseaseDocument12 pagesA Narrative Review of Influenza: A Seasonal and Pandemic DiseaseFreddy SueroNo ratings yet
- Discussion Text Vincentius Ivandra 34 12A1Document2 pagesDiscussion Text Vincentius Ivandra 34 12A1Kusuma PutraNo ratings yet
- Analysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolDocument3 pagesAnalysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Emergency MedicineDocument6 pagesEmergency MedicineChaht RojborwonwitayaNo ratings yet
- Revised HS360 ICICI Lombard Health Insurance PlanDocument29 pagesRevised HS360 ICICI Lombard Health Insurance PlanrbitrackerNo ratings yet
- JZWM Jan 2010Document7 pagesJZWM Jan 2010llcoffeeNo ratings yet
- Schizophrenia Spectrum and Other Psychotic DisordersDocument84 pagesSchizophrenia Spectrum and Other Psychotic DisordersJara YumiNo ratings yet
- Module SixDocument8 pagesModule SixEdelwise IgnacioNo ratings yet
- Resisted Isometric TestingDocument15 pagesResisted Isometric TestingDr. Disha Rupareliya BhateNo ratings yet
- Workshop BMW ManagementDocument42 pagesWorkshop BMW ManagementTami SelviNo ratings yet
- Chicken Pox Research PaperDocument5 pagesChicken Pox Research Paperc9rvz6mm100% (1)
- Module 1. Prudence in ChoicesDocument15 pagesModule 1. Prudence in ChoicesJellane Seletaria100% (1)
- Cardiology & Ekgs: Archer Nclex ReviewDocument59 pagesCardiology & Ekgs: Archer Nclex Reviewdaphne farleyNo ratings yet
- Forta Super-Sweep Fine®: Safety Data SheetDocument5 pagesForta Super-Sweep Fine®: Safety Data Sheetnoe tellezNo ratings yet
- Endline Grade 1 2022Document1 pageEndline Grade 1 2022JAIRAH BAUSANo ratings yet
- Article WJPR 1530873619Document5 pagesArticle WJPR 1530873619ammu ajitNo ratings yet
- Musculoskeletal System: Health AssessmentDocument43 pagesMusculoskeletal System: Health AssessmentEliezer Nuenay100% (1)
- Parasitology Babesia SPP CatDocument1 pageParasitology Babesia SPP CatIrina AtudoreiNo ratings yet
- Para-Transes Pre-Final Exam - Unit 4Document11 pagesPara-Transes Pre-Final Exam - Unit 4Aysha AishaNo ratings yet
- Instructions For Users: Drug Preparation Before EctDocument2 pagesInstructions For Users: Drug Preparation Before EctSymbat TileubergenNo ratings yet
- Grade 7 Term 1 Health Education SchemesDocument7 pagesGrade 7 Term 1 Health Education SchemesShanice NyairoNo ratings yet
- ParasiteDocument20 pagesParasiteHemanathan PraemNo ratings yet























































































Download as pdf or txt
You might also like
- Clinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsDocument8 pagesClinical Practice Guide On Antithrombotic Drug Dosing and Management of Antithrombotic Drug-Associated Bleeding Complications in AdultsdarekshepardNo ratings yet
- MILsgsdgds VDocument4 pagesMILsgsdgds Vgarywall.ukNo ratings yet
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Document55 pagesNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNo ratings yet
- Rivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban Xarelto Requiring Emergency Surgery or Treatment For HaemorrhageRomeo-Remus RaffaiNo ratings yet
- Rivaroxaban PresentationDocument13 pagesRivaroxaban PresentationReem El-HusseinyNo ratings yet
- UPDATED MalDocument52 pagesUPDATED MalABDIRAHIM ADAMNo ratings yet
- Hematologia - Hemostasia - Doacs (Jama 2018)Document2 pagesHematologia - Hemostasia - Doacs (Jama 2018)Matias FlammNo ratings yet
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDocument57 pagesNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNo ratings yet
- Newer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugDocument5 pagesNewer Oral Anticoagulants: Dabigatran Etexilate Is An Inactive Pro-DrugLouiseNo ratings yet
- Anticoag 2015november FullDocument14 pagesAnticoag 2015november FullRosanna FiorilloNo ratings yet
- DabigatranDocument25 pagesDabigatranNagesh JadavNo ratings yet
- AFib WarfarinVsNOACsDocument2 pagesAFib WarfarinVsNOACsalpha wolfNo ratings yet
- New Oral Anticoagulants Guidelines: Kai YapDocument23 pagesNew Oral Anticoagulants Guidelines: Kai YapMuhammad Reza FirdausNo ratings yet
- Rivaroxaban Sensitivity ThromboplastinDocument5 pagesRivaroxaban Sensitivity ThromboplastinpgdlilleNo ratings yet
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- Guidelines For Hemostasis and ThrombosisDocument4 pagesGuidelines For Hemostasis and Thrombosisjennifer acostaNo ratings yet
- 1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsDocument2 pages1388 Cardiovascular Drugs: Interactions Units Adverse Effects, Treatment, and PrecautionsPopov VictorNo ratings yet
- Anti CoagulantsDocument37 pagesAnti CoagulantsMaria khurshidNo ratings yet
- PredavanjeDocument54 pagesPredavanjeSnezana MihajlovicNo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Angiotensin Receptor BlockersDocument6 pagesAngiotensin Receptor BlockersMohammad Arafat SiddiquiNo ratings yet
- AnticoagulantsDocument3 pagesAnticoagulantsDarNo ratings yet
- TransfusionDocument3 pagesTransfusionjulissand10No ratings yet
- S 011 LBLDocument22 pagesS 011 LBLalexandr zinchenkoNo ratings yet
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDocument23 pagesVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
- ACOS BloodDocument7 pagesACOS Bloodpablin1788No ratings yet
- Acetaminophen (APAP) ToxicityDocument12 pagesAcetaminophen (APAP) ToxicityJessa MaeNo ratings yet
- Laboratory Control of Anticoagulant Therapy - PPTX LectDocument69 pagesLaboratory Control of Anticoagulant Therapy - PPTX LectTusabe FredNo ratings yet
- Switching Between AnticoagulantsDocument2 pagesSwitching Between AnticoagulantsSylvinho46No ratings yet
- Amended Intravenous Unfractionated Heparin Recommended StandardDocument4 pagesAmended Intravenous Unfractionated Heparin Recommended StandardTOJO JOSEPH TOMNo ratings yet
- Anticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDDocument103 pagesAnticoagulants: Presented By: ABHILASH Moderator: DR CH RAHUL MDabhilashreddy45100% (1)
- Comparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionDocument9 pagesComparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionLolita UmarNo ratings yet
- 10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHADocument32 pages10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHAEmdan SengadjiNo ratings yet
- VTE Form - Surgical & Medical PatientsDocument2 pagesVTE Form - Surgical & Medical PatientsNatasha BhasinNo ratings yet
- Drug Monograph ExampleDocument6 pagesDrug Monograph ExampleAaltiyaNo ratings yet
- Doac Switch Guidance Oct 2016Document1 pageDoac Switch Guidance Oct 2016RouaNo ratings yet
- Xarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Document26 pagesXarelto Tablet Salut Selaput 20 MG - Rivaroksaban - DKI1251602517C1 - 2020Dimas RfNo ratings yet
- Reversing The New AnticoagulantsDocument24 pagesReversing The New AnticoagulantsFurman BorstNo ratings yet
- Anti CoagulationDocument2 pagesAnti Coagulationsundance127No ratings yet
- Anticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectableDocument4 pagesAnticoagulation Guidelines For Neuraxial Procedures: Anticoagulants, InjectablepaulaNo ratings yet
- Saito 2006Document8 pagesSaito 2006cindyNo ratings yet
- EHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationDocument41 pagesEHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationAmelia Maria LasloNo ratings yet
- Anticoagulant DOACDocument39 pagesAnticoagulant DOACSukmawatiNo ratings yet
- Doacs AND LABORATORY1Document12 pagesDoacs AND LABORATORY1pasqualijNo ratings yet
- DRUGS2Document1 pageDRUGS2KaoriMarieSembranoNo ratings yet
- FAQ - DOAC in CKD Update - FinalDocument4 pagesFAQ - DOAC in CKD Update - Finalraea.dobsonNo ratings yet
- Nuevos anticoagulantes-BLOODDocument7 pagesNuevos anticoagulantes-BLOODnakroliNo ratings yet
- Anticoagulantele Si Explorarile Invazive 2021Document33 pagesAnticoagulantele Si Explorarile Invazive 2021GabrielaOaneNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- COVID 19 Anticoagulation Algorithm Version Final 1.1Document2 pagesCOVID 19 Anticoagulation Algorithm Version Final 1.1Emi PuspitasariNo ratings yet
- Rivaroxaban (Xarelto) Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesRivaroxaban (Xarelto) Requiring Emergency Surgery or Treatment For HaemorrhageWLC27No ratings yet
- Anticoagulation Related Bleeding - Guideline Summary: Click On The Appropriate Link BelowDocument19 pagesAnticoagulation Related Bleeding - Guideline Summary: Click On The Appropriate Link BelowIreneNo ratings yet
- Pharmacy CarbamazepineDocument21 pagesPharmacy CarbamazepineMargie dulacaNo ratings yet
- Monitoring The Traditional & The New AnticoagulantsDocument53 pagesMonitoring The Traditional & The New Anticoagulantsasclswisconsin100% (1)
- Comparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionDocument9 pagesComparison of The Efficacy of Morning Versus Evening Administration of Telmisartan in Essential HypertensionAnna ApriyantiNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Awareness, Attitudes, Prevention, and Perceptions of COVID-19 Outbreak Among Nurses in Saudi ArabiaDocument16 pagesAwareness, Attitudes, Prevention, and Perceptions of COVID-19 Outbreak Among Nurses in Saudi ArabiaAlec AnonNo ratings yet
- PSM case-ARI-7Document23 pagesPSM case-ARI-7Amer HussainNo ratings yet
- 135th KSW Transcript EN Draft v4 PDFDocument43 pages135th KSW Transcript EN Draft v4 PDFnew lightNo ratings yet
- CPR ACLS Study GuideDocument18 pagesCPR ACLS Study GuideJohn Phamacy100% (1)
- Nutrition To You: We BringDocument64 pagesNutrition To You: We Bringjose litoNo ratings yet
- Cover Letter For Mayo ClinicDocument7 pagesCover Letter For Mayo Clinicuyyjcvvcf100% (2)
- SuperlongevityDocument3 pagesSuperlongevityVadivelan MNo ratings yet
- Recalls Kaps 2017 April 01Document7 pagesRecalls Kaps 2017 April 01Aymen BekirNo ratings yet
- A Narrative Review of Influenza: A Seasonal and Pandemic DiseaseDocument12 pagesA Narrative Review of Influenza: A Seasonal and Pandemic DiseaseFreddy SueroNo ratings yet
- Discussion Text Vincentius Ivandra 34 12A1Document2 pagesDiscussion Text Vincentius Ivandra 34 12A1Kusuma PutraNo ratings yet
- Analysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolDocument3 pagesAnalysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Emergency MedicineDocument6 pagesEmergency MedicineChaht RojborwonwitayaNo ratings yet
- Revised HS360 ICICI Lombard Health Insurance PlanDocument29 pagesRevised HS360 ICICI Lombard Health Insurance PlanrbitrackerNo ratings yet
- JZWM Jan 2010Document7 pagesJZWM Jan 2010llcoffeeNo ratings yet
- Schizophrenia Spectrum and Other Psychotic DisordersDocument84 pagesSchizophrenia Spectrum and Other Psychotic DisordersJara YumiNo ratings yet
- Module SixDocument8 pagesModule SixEdelwise IgnacioNo ratings yet
- Resisted Isometric TestingDocument15 pagesResisted Isometric TestingDr. Disha Rupareliya BhateNo ratings yet
- Workshop BMW ManagementDocument42 pagesWorkshop BMW ManagementTami SelviNo ratings yet
- Chicken Pox Research PaperDocument5 pagesChicken Pox Research Paperc9rvz6mm100% (1)
- Module 1. Prudence in ChoicesDocument15 pagesModule 1. Prudence in ChoicesJellane Seletaria100% (1)
- Cardiology & Ekgs: Archer Nclex ReviewDocument59 pagesCardiology & Ekgs: Archer Nclex Reviewdaphne farleyNo ratings yet
- Forta Super-Sweep Fine®: Safety Data SheetDocument5 pagesForta Super-Sweep Fine®: Safety Data Sheetnoe tellezNo ratings yet
- Endline Grade 1 2022Document1 pageEndline Grade 1 2022JAIRAH BAUSANo ratings yet
- Article WJPR 1530873619Document5 pagesArticle WJPR 1530873619ammu ajitNo ratings yet
- Musculoskeletal System: Health AssessmentDocument43 pagesMusculoskeletal System: Health AssessmentEliezer Nuenay100% (1)
- Parasitology Babesia SPP CatDocument1 pageParasitology Babesia SPP CatIrina AtudoreiNo ratings yet
- Para-Transes Pre-Final Exam - Unit 4Document11 pagesPara-Transes Pre-Final Exam - Unit 4Aysha AishaNo ratings yet
- Instructions For Users: Drug Preparation Before EctDocument2 pagesInstructions For Users: Drug Preparation Before EctSymbat TileubergenNo ratings yet
- Grade 7 Term 1 Health Education SchemesDocument7 pagesGrade 7 Term 1 Health Education SchemesShanice NyairoNo ratings yet
- ParasiteDocument20 pagesParasiteHemanathan PraemNo ratings yet