
Spatiotemporal Pattern of COVID-19 Spread in Brazil: Coronavirus
Spatiotemporal Pattern of COVID-19 Spread in Brazil: Coronavirus
You might also like
- Defect Catalogue - Galva .Document45 pagesDefect Catalogue - Galva .Suvro ChakrabortyNo ratings yet
- Increases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesDocument4 pagesIncreases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesKyle Becker95% (19)
- EbooksHouse Super Earth Encyclopedia - DKDocument210 pagesEbooksHouse Super Earth Encyclopedia - DKRaj100% (6)
- ADocument15 pagesAmarianeNo ratings yet
- 1732-Article Text-5228-1-10-20210407Document3 pages1732-Article Text-5228-1-10-20210407NimraNo ratings yet
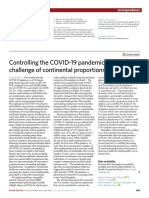
- Controlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsDocument2 pagesControlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsJoebson MaurilioNo ratings yet
- 3721-Article Text-11527-1-10-20210316Document9 pages3721-Article Text-11527-1-10-20210316sergio pecanNo ratings yet
- An Analysis of COVID-19 Mortality Underreporting BDocument14 pagesAn Analysis of COVID-19 Mortality Underreporting BFernando BorgesNo ratings yet
- Covid 19 Updatemarch 92021Document87 pagesCovid 19 Updatemarch 92021carb0ne14rNo ratings yet
- Sars-Cov-2: A Preliminary Comparative Epidemiological Analysis Between Brazil and The WorldDocument8 pagesSars-Cov-2: A Preliminary Comparative Epidemiological Analysis Between Brazil and The WorldRaphaelDaSilvaSeghetoNo ratings yet
- The COVID-19 Pandemic in Brazil: Some Aspects and ToolsDocument13 pagesThe COVID-19 Pandemic in Brazil: Some Aspects and ToolsnidhishpatelNo ratings yet
- DELATORRE, Et Al. (Memorias IOC, 2020) Rastramento Do COVID19Document13 pagesDELATORRE, Et Al. (Memorias IOC, 2020) Rastramento Do COVID19Antonio OscarNo ratings yet
- Risk Clusters of Covid 19 Transmission in Northeastern Brazil Prospective Space Time ModellingDocument8 pagesRisk Clusters of Covid 19 Transmission in Northeastern Brazil Prospective Space Time ModellingLucas AlmeidaNo ratings yet
- What To Expect From The 2017 Yellow Fever Outbreak in Brazil?Document4 pagesWhat To Expect From The 2017 Yellow Fever Outbreak in Brazil?Johnny Saavedra CamachoNo ratings yet
- NOGUEIRA Et Al (2022) - COVID-19's Intra-Urban Inequalities and Social Vulnerability in A Medium-Sized CityDocument10 pagesNOGUEIRA Et Al (2022) - COVID-19's Intra-Urban Inequalities and Social Vulnerability in A Medium-Sized CityJoão Pedro CaetanoNo ratings yet
- Covid 19 Death Analysis in ColombiaDocument14 pagesCovid 19 Death Analysis in ColombiaElsa FloresNo ratings yet
- Geographies of The COVID-19 Pandemic: Reuben Rose-RedwoodDocument10 pagesGeographies of The COVID-19 Pandemic: Reuben Rose-Redwoodcarol_israelNo ratings yet
- Covid-19: From Outbreak To Pandemic: GSJ: Volume 8, Issue 4, April 2020, Online: ISSN 2320-9186Document9 pagesCovid-19: From Outbreak To Pandemic: GSJ: Volume 8, Issue 4, April 2020, Online: ISSN 2320-9186Sri Andini WidyaningrumNo ratings yet
- Differential Effects of Intervention Timing OnDocument10 pagesDifferential Effects of Intervention Timing OnfaizahmedNo ratings yet
- 1395-Manuscrito (Texto Do Artigo) - 644-1-10-20210802Document9 pages1395-Manuscrito (Texto Do Artigo) - 644-1-10-20210802gabriel-ortolaneNo ratings yet
- Infectious Disease Modelling: Marcio Luis Ferreira Nascimento PH.DDocument11 pagesInfectious Disease Modelling: Marcio Luis Ferreira Nascimento PH.DMarcio Luis Ferreira NascimentoNo ratings yet
- 1 s2.0 S0168170222001125 MainDocument4 pages1 s2.0 S0168170222001125 MainStephaneNo ratings yet
- ArtigosDocument7 pagesArtigosLeoberto TorresNo ratings yet
- Research in Social and Administrative PharmacyDocument4 pagesResearch in Social and Administrative PharmacyAndrea MendozaNo ratings yet
- Assessing The Potential Impacts of COVID-19 in BraDocument14 pagesAssessing The Potential Impacts of COVID-19 in BraLeonardo MartinsNo ratings yet
- CLN 71 08 455Document9 pagesCLN 71 08 455Ranny Yovita MaharaniNo ratings yet
- C. Tropis Auler2020Document10 pagesC. Tropis Auler2020Mastifa HanasitaNo ratings yet
- The Pandemic Threatens Aged Rural Regions Most: Ilya Kashnitsky, José Manuel AburtoDocument2 pagesThe Pandemic Threatens Aged Rural Regions Most: Ilya Kashnitsky, José Manuel AburtoalexanderNo ratings yet
- Report 46: Factors Driving Extensive Spatial and Temporal Fluctuations in COVID 19 Fatality Rates in Brazilian HospitalsDocument20 pagesReport 46: Factors Driving Extensive Spatial and Temporal Fluctuations in COVID 19 Fatality Rates in Brazilian Hospitalswill1329No ratings yet
- Bayesian Spatial Modeling of COVID-19 Case-Fatality Rate InequalitiesDocument9 pagesBayesian Spatial Modeling of COVID-19 Case-Fatality Rate InequalitiesCarlos MeraNo ratings yet
- PAHO - WHO Data - Annual Arbovirus Bulletin 2020Document16 pagesPAHO - WHO Data - Annual Arbovirus Bulletin 2020Analia UrueñaNo ratings yet
- COVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilDocument2 pagesCOVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilRaíssa Barbosa LuccheseNo ratings yet
- Impact of Lockdown - BrazilDocument4 pagesImpact of Lockdown - Brazilbismillah skripsiNo ratings yet
- Epidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruDocument12 pagesEpidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruyanettNo ratings yet
- Epidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruDocument12 pagesEpidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruyanettNo ratings yet
- 1 s2.0 S2211335522000596 MainDocument10 pages1 s2.0 S2211335522000596 MainSamuel AraújoNo ratings yet
- Spatial and Epidemiological Analyses of COVID-19 in The Older Population of The Brazilian Amazon RegionDuring 2020Document6 pagesSpatial and Epidemiological Analyses of COVID-19 in The Older Population of The Brazilian Amazon RegionDuring 2020marcusjabaNo ratings yet
- Summer Flu TropicsDocument9 pagesSummer Flu TropicskaznatsNo ratings yet
- 2023 March 28 PheepiupdatedengueenDocument13 pages2023 March 28 Pheepiupdatedengueenlast warriorsNo ratings yet
- Chronic Non Communicable DiseaseDocument13 pagesChronic Non Communicable DiseaseGabryelNo ratings yet
- Common Pitfalls in The Interpretation of COVID-19 Data and StatisticsDocument5 pagesCommon Pitfalls in The Interpretation of COVID-19 Data and StatisticsMargareth CarvalhoNo ratings yet
- Lol 2Document7 pagesLol 2welton.dionisioNo ratings yet
- DownloadDocument9 pagesDownloadcesar8319No ratings yet
- 1 s2.0 S120197122030285X PDFDocument3 pages1 s2.0 S120197122030285X PDFnaira9valentina9pareNo ratings yet
- Brazilian Modeling CovidDocument41 pagesBrazilian Modeling CovidAbdelkaderNo ratings yet
- Groumpos-Apostolopoulos2021 Article ModelingTheSpreadOfDangerousPaDocument16 pagesGroumpos-Apostolopoulos2021 Article ModelingTheSpreadOfDangerousPaasdNo ratings yet
- Detection of Outlier Prefectures On The MortalityDocument3 pagesDetection of Outlier Prefectures On The MortalityEllen Dian Permata Soffa EridineNo ratings yet
- COVID-19 in Brazil - Advantages of A Socialized Unified Health System and Preparation To Contain CasesDocument6 pagesCOVID-19 in Brazil - Advantages of A Socialized Unified Health System and Preparation To Contain CasesFernando FernandesNo ratings yet
- Sorci ETAL2020Document11 pagesSorci ETAL2020ee210002004No ratings yet
- 16IJAERS 1020205 Logistic PDFDocument11 pages16IJAERS 1020205 Logistic PDFIJAERS JOURNALNo ratings yet
- DownloadDocument8 pagesDownloadbiomed.jaquelineNo ratings yet
- Exploring The Nexus Between Medical Geography and Covid-19 Control in NigeriaDocument16 pagesExploring The Nexus Between Medical Geography and Covid-19 Control in NigeriaHabib IbrahimNo ratings yet
- PIIS0140673619325243Document2 pagesPIIS0140673619325243blue diamondNo ratings yet
- 10.1016@s2214 109x2030285 0 PDFDocument9 pages10.1016@s2214 109x2030285 0 PDFNathalia CecchetNo ratings yet
- Jeronimus PersonalityandtheCoronavirusPandemicDocument107 pagesJeronimus PersonalityandtheCoronavirusPandemicEmmaCorovicNo ratings yet
- 10.1038@s41562 020 0928 4 PDFDocument21 pages10.1038@s41562 020 0928 4 PDFNathalia CecchetNo ratings yet
- Preprint Not Peer ReviewedDocument15 pagesPreprint Not Peer ReviewedAndré BarbosaNo ratings yet
- Compartmentalized Mathematical Model To Predict Future NumberDocument14 pagesCompartmentalized Mathematical Model To Predict Future Numberchristian david anturi ospinaNo ratings yet
- 6 Interpretable Machine Learning For Mortality Modeling On Patients With Chronic Diseases Considering The COVID 19 Pandemic in A Region of Chile ADocument9 pages6 Interpretable Machine Learning For Mortality Modeling On Patients With Chronic Diseases Considering The COVID 19 Pandemic in A Region of Chile AClaudia Paz Barria SandovalNo ratings yet
- The Impact of a Deadly Pandemic on Individual, Society, Economy and the WorldFrom EverandThe Impact of a Deadly Pandemic on Individual, Society, Economy and the WorldNo ratings yet
- Projeto GibbonsDocument34 pagesProjeto GibbonsJoebson MaurilioNo ratings yet
- Paper Violência Contra Jovens MulheresDocument5 pagesPaper Violência Contra Jovens MulheresJoebson MaurilioNo ratings yet
- Artigo EconomiADocument11 pagesArtigo EconomiAJoebson MaurilioNo ratings yet
- Paper MotorcycleDocument9 pagesPaper MotorcycleJoebson MaurilioNo ratings yet
- Controlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsDocument2 pagesControlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsJoebson MaurilioNo ratings yet
- Araneda 2021Document8 pagesAraneda 2021Joebson MaurilioNo ratings yet
- ENV & MAP FileDocument43 pagesENV & MAP FileJit MukherheeNo ratings yet
- John F. Butterworth, David C. Mackey, John D. Wasnick - Morgan & Mikhail's Clinical Anesthesiology-McGraw-Hill Education - Medical (2018)Document21 pagesJohn F. Butterworth, David C. Mackey, John D. Wasnick - Morgan & Mikhail's Clinical Anesthesiology-McGraw-Hill Education - Medical (2018)fad02fadNo ratings yet
- Modül 17 Pervane Ders Notu (Sezai Turpçu) : PropellersDocument4 pagesModül 17 Pervane Ders Notu (Sezai Turpçu) : Propellersmevlüt said çalgınNo ratings yet
- Reverse Unloader Valve Rev0Document1 pageReverse Unloader Valve Rev0JasonNo ratings yet
- House Riddles (1) - EasyDocument3 pagesHouse Riddles (1) - EasyMiyasar AzatbaevaNo ratings yet
- A320 Normal ProceduresDocument43 pagesA320 Normal ProceduresSzymon GawrysiukNo ratings yet
- Lit50 48CDocument2 pagesLit50 48CcamiloNo ratings yet
- Chemostat Recycle (Autosaved)Document36 pagesChemostat Recycle (Autosaved)Zeny Naranjo0% (1)
- Motion in 1 D Jee Main LevelDocument7 pagesMotion in 1 D Jee Main LevelShashwat KhuranaNo ratings yet
- Tutorial 8 QuestionsDocument3 pagesTutorial 8 QuestionsEvan DuhNo ratings yet
- Optimizing HPLC Methods 1684601740Document46 pagesOptimizing HPLC Methods 1684601740AlexandreLuizdeSouzaNo ratings yet
- Symmetry: Multinode M2150 Intelligent ControllerDocument6 pagesSymmetry: Multinode M2150 Intelligent Controlleradela sampayoNo ratings yet
- Factores de Virulencia Del Streptococcus PneumoniaeDocument7 pagesFactores de Virulencia Del Streptococcus PneumoniaeFranklin ArandaNo ratings yet
- Dust CleanDocument2 pagesDust CleanArdino Putra PerbawaNo ratings yet
- XII - ECONOMICS - Indian Economy On The Eve of Independence - Assignment 3Document1 pageXII - ECONOMICS - Indian Economy On The Eve of Independence - Assignment 3tanisha bailwalNo ratings yet
- Chapter-3 - Pie ChartsDocument6 pagesChapter-3 - Pie Chartsvishesh bhatiaNo ratings yet
- 4.0 Environmental Impacts and Mitigation Measures Potential Environmental ImpactsDocument7 pages4.0 Environmental Impacts and Mitigation Measures Potential Environmental ImpactsCirilo Jr. LagnasonNo ratings yet
- Dispersion PollutantsDocument18 pagesDispersion PollutantsAmira GogoantaNo ratings yet
- The Wheel and The BobsleighDocument2 pagesThe Wheel and The BobsleighHarisNo ratings yet
- ASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiaDocument23 pagesASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiarahulgangalNo ratings yet
- Oh I Want To See Him, Ill Fly Away, Blessed Be Your Name, Everlasting GodDocument47 pagesOh I Want To See Him, Ill Fly Away, Blessed Be Your Name, Everlasting GodRenato PatunganNo ratings yet
- Hilti Hit Hy 200 With Hit VDocument18 pagesHilti Hit Hy 200 With Hit VRobinReyndersNo ratings yet
- FibromaDocument3 pagesFibromaAsiyath HNo ratings yet
- Pollution ProjectDocument17 pagesPollution Projectdenis becheruNo ratings yet
- RT 200 Midterm Ist TopicDocument34 pagesRT 200 Midterm Ist TopicYola RazoNo ratings yet
- Position, Leverage and Opportunity: A Typology of Strategic Logics Linking Resources With Competitive AdvantageDocument16 pagesPosition, Leverage and Opportunity: A Typology of Strategic Logics Linking Resources With Competitive AdvantageEdgar LL.CNo ratings yet
- Lab 5 - Ring AC DistributorDocument6 pagesLab 5 - Ring AC DistributorMuhammad AnasNo ratings yet
- Brain Computer InterfacesDocument4 pagesBrain Computer InterfacesDavidNo ratings yet




























































































Download as pdf or txt
You might also like
- Defect Catalogue - Galva .Document45 pagesDefect Catalogue - Galva .Suvro ChakrabortyNo ratings yet
- Increases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesDocument4 pagesIncreases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesKyle Becker95% (19)
- EbooksHouse Super Earth Encyclopedia - DKDocument210 pagesEbooksHouse Super Earth Encyclopedia - DKRaj100% (6)
- ADocument15 pagesAmarianeNo ratings yet
- 1732-Article Text-5228-1-10-20210407Document3 pages1732-Article Text-5228-1-10-20210407NimraNo ratings yet
- Controlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsDocument2 pagesControlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsJoebson MaurilioNo ratings yet
- 3721-Article Text-11527-1-10-20210316Document9 pages3721-Article Text-11527-1-10-20210316sergio pecanNo ratings yet
- An Analysis of COVID-19 Mortality Underreporting BDocument14 pagesAn Analysis of COVID-19 Mortality Underreporting BFernando BorgesNo ratings yet
- Covid 19 Updatemarch 92021Document87 pagesCovid 19 Updatemarch 92021carb0ne14rNo ratings yet
- Sars-Cov-2: A Preliminary Comparative Epidemiological Analysis Between Brazil and The WorldDocument8 pagesSars-Cov-2: A Preliminary Comparative Epidemiological Analysis Between Brazil and The WorldRaphaelDaSilvaSeghetoNo ratings yet
- The COVID-19 Pandemic in Brazil: Some Aspects and ToolsDocument13 pagesThe COVID-19 Pandemic in Brazil: Some Aspects and ToolsnidhishpatelNo ratings yet
- DELATORRE, Et Al. (Memorias IOC, 2020) Rastramento Do COVID19Document13 pagesDELATORRE, Et Al. (Memorias IOC, 2020) Rastramento Do COVID19Antonio OscarNo ratings yet
- Risk Clusters of Covid 19 Transmission in Northeastern Brazil Prospective Space Time ModellingDocument8 pagesRisk Clusters of Covid 19 Transmission in Northeastern Brazil Prospective Space Time ModellingLucas AlmeidaNo ratings yet
- What To Expect From The 2017 Yellow Fever Outbreak in Brazil?Document4 pagesWhat To Expect From The 2017 Yellow Fever Outbreak in Brazil?Johnny Saavedra CamachoNo ratings yet
- NOGUEIRA Et Al (2022) - COVID-19's Intra-Urban Inequalities and Social Vulnerability in A Medium-Sized CityDocument10 pagesNOGUEIRA Et Al (2022) - COVID-19's Intra-Urban Inequalities and Social Vulnerability in A Medium-Sized CityJoão Pedro CaetanoNo ratings yet
- Covid 19 Death Analysis in ColombiaDocument14 pagesCovid 19 Death Analysis in ColombiaElsa FloresNo ratings yet
- Geographies of The COVID-19 Pandemic: Reuben Rose-RedwoodDocument10 pagesGeographies of The COVID-19 Pandemic: Reuben Rose-Redwoodcarol_israelNo ratings yet
- Covid-19: From Outbreak To Pandemic: GSJ: Volume 8, Issue 4, April 2020, Online: ISSN 2320-9186Document9 pagesCovid-19: From Outbreak To Pandemic: GSJ: Volume 8, Issue 4, April 2020, Online: ISSN 2320-9186Sri Andini WidyaningrumNo ratings yet
- Differential Effects of Intervention Timing OnDocument10 pagesDifferential Effects of Intervention Timing OnfaizahmedNo ratings yet
- 1395-Manuscrito (Texto Do Artigo) - 644-1-10-20210802Document9 pages1395-Manuscrito (Texto Do Artigo) - 644-1-10-20210802gabriel-ortolaneNo ratings yet
- Infectious Disease Modelling: Marcio Luis Ferreira Nascimento PH.DDocument11 pagesInfectious Disease Modelling: Marcio Luis Ferreira Nascimento PH.DMarcio Luis Ferreira NascimentoNo ratings yet
- 1 s2.0 S0168170222001125 MainDocument4 pages1 s2.0 S0168170222001125 MainStephaneNo ratings yet
- ArtigosDocument7 pagesArtigosLeoberto TorresNo ratings yet
- Research in Social and Administrative PharmacyDocument4 pagesResearch in Social and Administrative PharmacyAndrea MendozaNo ratings yet
- Assessing The Potential Impacts of COVID-19 in BraDocument14 pagesAssessing The Potential Impacts of COVID-19 in BraLeonardo MartinsNo ratings yet
- CLN 71 08 455Document9 pagesCLN 71 08 455Ranny Yovita MaharaniNo ratings yet
- C. Tropis Auler2020Document10 pagesC. Tropis Auler2020Mastifa HanasitaNo ratings yet
- The Pandemic Threatens Aged Rural Regions Most: Ilya Kashnitsky, José Manuel AburtoDocument2 pagesThe Pandemic Threatens Aged Rural Regions Most: Ilya Kashnitsky, José Manuel AburtoalexanderNo ratings yet
- Report 46: Factors Driving Extensive Spatial and Temporal Fluctuations in COVID 19 Fatality Rates in Brazilian HospitalsDocument20 pagesReport 46: Factors Driving Extensive Spatial and Temporal Fluctuations in COVID 19 Fatality Rates in Brazilian Hospitalswill1329No ratings yet
- Bayesian Spatial Modeling of COVID-19 Case-Fatality Rate InequalitiesDocument9 pagesBayesian Spatial Modeling of COVID-19 Case-Fatality Rate InequalitiesCarlos MeraNo ratings yet
- PAHO - WHO Data - Annual Arbovirus Bulletin 2020Document16 pagesPAHO - WHO Data - Annual Arbovirus Bulletin 2020Analia UrueñaNo ratings yet
- COVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilDocument2 pagesCOVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilRaíssa Barbosa LuccheseNo ratings yet
- Impact of Lockdown - BrazilDocument4 pagesImpact of Lockdown - Brazilbismillah skripsiNo ratings yet
- Epidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruDocument12 pagesEpidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruyanettNo ratings yet
- Epidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruDocument12 pagesEpidemiological Analysis of COVID-19 Cases in Native Amazonian Communities From PeruyanettNo ratings yet
- 1 s2.0 S2211335522000596 MainDocument10 pages1 s2.0 S2211335522000596 MainSamuel AraújoNo ratings yet
- Spatial and Epidemiological Analyses of COVID-19 in The Older Population of The Brazilian Amazon RegionDuring 2020Document6 pagesSpatial and Epidemiological Analyses of COVID-19 in The Older Population of The Brazilian Amazon RegionDuring 2020marcusjabaNo ratings yet
- Summer Flu TropicsDocument9 pagesSummer Flu TropicskaznatsNo ratings yet
- 2023 March 28 PheepiupdatedengueenDocument13 pages2023 March 28 Pheepiupdatedengueenlast warriorsNo ratings yet
- Chronic Non Communicable DiseaseDocument13 pagesChronic Non Communicable DiseaseGabryelNo ratings yet
- Common Pitfalls in The Interpretation of COVID-19 Data and StatisticsDocument5 pagesCommon Pitfalls in The Interpretation of COVID-19 Data and StatisticsMargareth CarvalhoNo ratings yet
- Lol 2Document7 pagesLol 2welton.dionisioNo ratings yet
- DownloadDocument9 pagesDownloadcesar8319No ratings yet
- 1 s2.0 S120197122030285X PDFDocument3 pages1 s2.0 S120197122030285X PDFnaira9valentina9pareNo ratings yet
- Brazilian Modeling CovidDocument41 pagesBrazilian Modeling CovidAbdelkaderNo ratings yet
- Groumpos-Apostolopoulos2021 Article ModelingTheSpreadOfDangerousPaDocument16 pagesGroumpos-Apostolopoulos2021 Article ModelingTheSpreadOfDangerousPaasdNo ratings yet
- Detection of Outlier Prefectures On The MortalityDocument3 pagesDetection of Outlier Prefectures On The MortalityEllen Dian Permata Soffa EridineNo ratings yet
- COVID-19 in Brazil - Advantages of A Socialized Unified Health System and Preparation To Contain CasesDocument6 pagesCOVID-19 in Brazil - Advantages of A Socialized Unified Health System and Preparation To Contain CasesFernando FernandesNo ratings yet
- Sorci ETAL2020Document11 pagesSorci ETAL2020ee210002004No ratings yet
- 16IJAERS 1020205 Logistic PDFDocument11 pages16IJAERS 1020205 Logistic PDFIJAERS JOURNALNo ratings yet
- DownloadDocument8 pagesDownloadbiomed.jaquelineNo ratings yet
- Exploring The Nexus Between Medical Geography and Covid-19 Control in NigeriaDocument16 pagesExploring The Nexus Between Medical Geography and Covid-19 Control in NigeriaHabib IbrahimNo ratings yet
- PIIS0140673619325243Document2 pagesPIIS0140673619325243blue diamondNo ratings yet
- 10.1016@s2214 109x2030285 0 PDFDocument9 pages10.1016@s2214 109x2030285 0 PDFNathalia CecchetNo ratings yet
- Jeronimus PersonalityandtheCoronavirusPandemicDocument107 pagesJeronimus PersonalityandtheCoronavirusPandemicEmmaCorovicNo ratings yet
- 10.1038@s41562 020 0928 4 PDFDocument21 pages10.1038@s41562 020 0928 4 PDFNathalia CecchetNo ratings yet
- Preprint Not Peer ReviewedDocument15 pagesPreprint Not Peer ReviewedAndré BarbosaNo ratings yet
- Compartmentalized Mathematical Model To Predict Future NumberDocument14 pagesCompartmentalized Mathematical Model To Predict Future Numberchristian david anturi ospinaNo ratings yet
- 6 Interpretable Machine Learning For Mortality Modeling On Patients With Chronic Diseases Considering The COVID 19 Pandemic in A Region of Chile ADocument9 pages6 Interpretable Machine Learning For Mortality Modeling On Patients With Chronic Diseases Considering The COVID 19 Pandemic in A Region of Chile AClaudia Paz Barria SandovalNo ratings yet
- The Impact of a Deadly Pandemic on Individual, Society, Economy and the WorldFrom EverandThe Impact of a Deadly Pandemic on Individual, Society, Economy and the WorldNo ratings yet
- Projeto GibbonsDocument34 pagesProjeto GibbonsJoebson MaurilioNo ratings yet
- Paper Violência Contra Jovens MulheresDocument5 pagesPaper Violência Contra Jovens MulheresJoebson MaurilioNo ratings yet
- Artigo EconomiADocument11 pagesArtigo EconomiAJoebson MaurilioNo ratings yet
- Paper MotorcycleDocument9 pagesPaper MotorcycleJoebson MaurilioNo ratings yet
- Controlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsDocument2 pagesControlling The COVID-19 Pandemic in Brazil: A Challenge of Continental ProportionsJoebson MaurilioNo ratings yet
- Araneda 2021Document8 pagesAraneda 2021Joebson MaurilioNo ratings yet
- ENV & MAP FileDocument43 pagesENV & MAP FileJit MukherheeNo ratings yet
- John F. Butterworth, David C. Mackey, John D. Wasnick - Morgan & Mikhail's Clinical Anesthesiology-McGraw-Hill Education - Medical (2018)Document21 pagesJohn F. Butterworth, David C. Mackey, John D. Wasnick - Morgan & Mikhail's Clinical Anesthesiology-McGraw-Hill Education - Medical (2018)fad02fadNo ratings yet
- Modül 17 Pervane Ders Notu (Sezai Turpçu) : PropellersDocument4 pagesModül 17 Pervane Ders Notu (Sezai Turpçu) : Propellersmevlüt said çalgınNo ratings yet
- Reverse Unloader Valve Rev0Document1 pageReverse Unloader Valve Rev0JasonNo ratings yet
- House Riddles (1) - EasyDocument3 pagesHouse Riddles (1) - EasyMiyasar AzatbaevaNo ratings yet
- A320 Normal ProceduresDocument43 pagesA320 Normal ProceduresSzymon GawrysiukNo ratings yet
- Lit50 48CDocument2 pagesLit50 48CcamiloNo ratings yet
- Chemostat Recycle (Autosaved)Document36 pagesChemostat Recycle (Autosaved)Zeny Naranjo0% (1)
- Motion in 1 D Jee Main LevelDocument7 pagesMotion in 1 D Jee Main LevelShashwat KhuranaNo ratings yet
- Tutorial 8 QuestionsDocument3 pagesTutorial 8 QuestionsEvan DuhNo ratings yet
- Optimizing HPLC Methods 1684601740Document46 pagesOptimizing HPLC Methods 1684601740AlexandreLuizdeSouzaNo ratings yet
- Symmetry: Multinode M2150 Intelligent ControllerDocument6 pagesSymmetry: Multinode M2150 Intelligent Controlleradela sampayoNo ratings yet
- Factores de Virulencia Del Streptococcus PneumoniaeDocument7 pagesFactores de Virulencia Del Streptococcus PneumoniaeFranklin ArandaNo ratings yet
- Dust CleanDocument2 pagesDust CleanArdino Putra PerbawaNo ratings yet
- XII - ECONOMICS - Indian Economy On The Eve of Independence - Assignment 3Document1 pageXII - ECONOMICS - Indian Economy On The Eve of Independence - Assignment 3tanisha bailwalNo ratings yet
- Chapter-3 - Pie ChartsDocument6 pagesChapter-3 - Pie Chartsvishesh bhatiaNo ratings yet
- 4.0 Environmental Impacts and Mitigation Measures Potential Environmental ImpactsDocument7 pages4.0 Environmental Impacts and Mitigation Measures Potential Environmental ImpactsCirilo Jr. LagnasonNo ratings yet
- Dispersion PollutantsDocument18 pagesDispersion PollutantsAmira GogoantaNo ratings yet
- The Wheel and The BobsleighDocument2 pagesThe Wheel and The BobsleighHarisNo ratings yet
- ASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiaDocument23 pagesASSOCHAM Aviotech Study On Aerospace and Defence Manufacturing in IndiarahulgangalNo ratings yet
- Oh I Want To See Him, Ill Fly Away, Blessed Be Your Name, Everlasting GodDocument47 pagesOh I Want To See Him, Ill Fly Away, Blessed Be Your Name, Everlasting GodRenato PatunganNo ratings yet
- Hilti Hit Hy 200 With Hit VDocument18 pagesHilti Hit Hy 200 With Hit VRobinReyndersNo ratings yet
- FibromaDocument3 pagesFibromaAsiyath HNo ratings yet
- Pollution ProjectDocument17 pagesPollution Projectdenis becheruNo ratings yet
- RT 200 Midterm Ist TopicDocument34 pagesRT 200 Midterm Ist TopicYola RazoNo ratings yet
- Position, Leverage and Opportunity: A Typology of Strategic Logics Linking Resources With Competitive AdvantageDocument16 pagesPosition, Leverage and Opportunity: A Typology of Strategic Logics Linking Resources With Competitive AdvantageEdgar LL.CNo ratings yet
- Lab 5 - Ring AC DistributorDocument6 pagesLab 5 - Ring AC DistributorMuhammad AnasNo ratings yet
- Brain Computer InterfacesDocument4 pagesBrain Computer InterfacesDavidNo ratings yet