Download as pdf or txt
You might also like
- Scope Management Plan: Group 16 Western Sydney AirportDocument11 pagesScope Management Plan: Group 16 Western Sydney AirportZoe TanNo ratings yet
- Step-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairDocument10 pagesStep-By-Step Guide - Minimally Invasive Lumbar Spine Decompression and Dural RepairPankaj Vatsa100% (1)
- Skills Lab Vascular Surgery OneDocument10 pagesSkills Lab Vascular Surgery OneZain A AlrustomNo ratings yet
- Vascular Skills PresentationDocument101 pagesVascular Skills PresentationPatch Adams100% (2)
- Presentation 2Document49 pagesPresentation 2LuigiPavalNo ratings yet
- Catalogo Protesis VascularDocument57 pagesCatalogo Protesis VascularCINDY SHAKIRA CHAVEZ CHAVEZNo ratings yet
- Harvesting SVGDocument26 pagesHarvesting SVGSamuel Hotma Rotua Sinaga100% (1)
- Abdominal AortaDocument41 pagesAbdominal AortaMichael IdowuNo ratings yet
- Peripheral Arterial Disease and AngiographyDocument12 pagesPeripheral Arterial Disease and AngiographyFiza MushtaqNo ratings yet
- Surgery On Vessels and Nerfs 2020Document49 pagesSurgery On Vessels and Nerfs 2020Timbur IgorNo ratings yet
- Thoracic Endovascular Aortic RepairDocument2 pagesThoracic Endovascular Aortic RepairYen NgoNo ratings yet
- ACFrOgBJ11ZY9WD49wZ4mx Nu2QyGvK-qmOsUHKXVRSBkfEbfwWLzfDaE3L9 rejnh0YFVdwEJYzgZnIKRyT1AcSkbIft12Sqr5t7NCHqRd2MZQD7DJSwhSvGVKwQbTUPSaBLuf75yV EO1CV72IDocument8 pagesACFrOgBJ11ZY9WD49wZ4mx Nu2QyGvK-qmOsUHKXVRSBkfEbfwWLzfDaE3L9 rejnh0YFVdwEJYzgZnIKRyT1AcSkbIft12Sqr5t7NCHqRd2MZQD7DJSwhSvGVKwQbTUPSaBLuf75yV EO1CV72Iمحمد سعد طهNo ratings yet
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 pagesReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Saphenousveinharvestingpresentation 150824151458 Lva1 App6892Document43 pagesSaphenousveinharvestingpresentation 150824151458 Lva1 App6892vamshidhNo ratings yet
- Cardiac Catheterization and PCIDocument75 pagesCardiac Catheterization and PCIJobelyn Tunay100% (1)
- Vessel Anastomosis Rev.2Document18 pagesVessel Anastomosis Rev.2okmaronab febrizaNo ratings yet
- Coronary Balloon PresentationDocument42 pagesCoronary Balloon Presentationhbasrawala110No ratings yet
- Basics of Microvascular SurgeryDocument33 pagesBasics of Microvascular SurgeryPratikshya KothiaNo ratings yet
- Arterial CannulaDocument52 pagesArterial CannulaRuchi VatwaniNo ratings yet
- MicrosurgeryDocument20 pagesMicrosurgeryNyein Chan AungNo ratings yet
- Overview of FistulasDocument39 pagesOverview of FistulasWade JacksonNo ratings yet
- Up To Date. GasometryDocument46 pagesUp To Date. GasometryGuardito PequeñoNo ratings yet
- Aneurysm ClipsDocument28 pagesAneurysm ClipsVamsiKrishnaChagalakondaNo ratings yet
- Biofluid Mechanics Chapter 5Document11 pagesBiofluid Mechanics Chapter 5AbcdNo ratings yet
- Surgical Interventions, Monitoring and SupportDocument41 pagesSurgical Interventions, Monitoring and SupportPreciousShaizNo ratings yet
- Surgical Interventions, Monitoring and SupportDocument41 pagesSurgical Interventions, Monitoring and SupportDr. Rabail MalikNo ratings yet
- Group ADocument12 pagesGroup ASalifyanji SimpambaNo ratings yet
- Omar F. Hadidi, MD, Tom C. Nguyen, MD: Chapter 10: Step-By-Step Guide: Transfemoral Sapien S3 TAVRDocument12 pagesOmar F. Hadidi, MD, Tom C. Nguyen, MD: Chapter 10: Step-By-Step Guide: Transfemoral Sapien S3 TAVRlavanyaNo ratings yet
- Approaches To Colloid Cyst (Of 3 Ventricle) : HardikDocument46 pagesApproaches To Colloid Cyst (Of 3 Ventricle) : HardikHardik RajyaguruNo ratings yet
- 10 20515-Otd 97205-190634Document6 pages10 20515-Otd 97205-190634majanga johnNo ratings yet
- Heart Disease and Heart Bypass SurgeryDocument3 pagesHeart Disease and Heart Bypass SurgeryAuladi Lubis ∑No ratings yet
- AmputationDocument52 pagesAmputationShobhit SharmaNo ratings yet
- Surgical Intervention Pseudo AneurysmDocument1 pageSurgical Intervention Pseudo AneurysmTasha_Caballer_379No ratings yet
- Arterial Blood GasesDocument21 pagesArterial Blood GasesJesús Alberto López VenturaNo ratings yet
- Nephrol. Dial. Transplant. 2002 Konner 376 9Document4 pagesNephrol. Dial. Transplant. 2002 Konner 376 9Adriana VickNo ratings yet
- Saphenousveinharvestingpresentation 150824151458 Lva1 App6892Document46 pagesSaphenousveinharvestingpresentation 150824151458 Lva1 App6892Maryasi PanjaitanNo ratings yet
- Arterial Blood Gases - UpToDateDocument20 pagesArterial Blood Gases - UpToDateGuillermo MárquezNo ratings yet
- DR Ranjith MP Senior Resident Department of Cardiology Government Medical College KozhikodeDocument78 pagesDR Ranjith MP Senior Resident Department of Cardiology Government Medical College KozhikodePutu Adi SusantaNo ratings yet
- Blood Collection: Islamic University - Gaza (IUG)Document105 pagesBlood Collection: Islamic University - Gaza (IUG)Razvan ChiricaNo ratings yet
- Thoracodorsal Artery Perforator Flap (TAP Flap)Document1 pageThoracodorsal Artery Perforator Flap (TAP Flap)Consultorio Cirurgia plásticaNo ratings yet
- Thorakales Aortenaneurysma DissertationDocument7 pagesThorakales Aortenaneurysma DissertationCustomWrittenPaperLittleRock100% (1)
- Final Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaDocument44 pagesFinal Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaKing ThiyagaNo ratings yet
- Oral Surgery FlapsDocument13 pagesOral Surgery Flapshaneefmdf100% (1)
- EvarDocument78 pagesEvarAnonymous 14iQy0nwMZNo ratings yet
- CardioDocument8 pagesCardioJewel BabiaNo ratings yet
- Aortic Aneurysm: DR Rahul CDocument79 pagesAortic Aneurysm: DR Rahul CIrwan Meidi LubisNo ratings yet
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDocument9 pagesHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenNo ratings yet
- Vascular Surgical ProceduresDocument10 pagesVascular Surgical Proceduresafeekhan0007No ratings yet
- Presentation By: Dr Saima ( 赛马) N Nakapolo BDS, 4 YearDocument43 pagesPresentation By: Dr Saima ( 赛马) N Nakapolo BDS, 4 YearIsak ShatikaNo ratings yet
- R3 Surgical Technique - IntlDocument27 pagesR3 Surgical Technique - Intlquetecojaunburro100% (1)
- Post PCNL Hemorrhage: Presenter: DR Sumit KabraDocument30 pagesPost PCNL Hemorrhage: Presenter: DR Sumit KabraGaurav GuptaNo ratings yet
- Bss1 - Indonesia - Share2018Document43 pagesBss1 - Indonesia - Share2018Michael RaktionNo ratings yet
- Closing TechniquesDocument14 pagesClosing TechniquesAndrei BulgariuNo ratings yet
- Arterial Blood Gases - UpToDateDocument41 pagesArterial Blood Gases - UpToDateMelanny Perez GonzalesNo ratings yet
- OrchiectomyDocument28 pagesOrchiectomytutorial 18No ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersFrom EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Angioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAngioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- A Short Treatise on the Section of the Prostate Gland in Lithotomy: With an Explanation of a Safe and Easy Method of Conducting the Operation on the Principles of CheseldenFrom EverandA Short Treatise on the Section of the Prostate Gland in Lithotomy: With an Explanation of a Safe and Easy Method of Conducting the Operation on the Principles of CheseldenNo ratings yet
- Diah Mustika HW, SPS, Kic Intensive Care Unit of Emergency Department Naval Hospital DR Ramelan, SurabayaDocument33 pagesDiah Mustika HW, SPS, Kic Intensive Care Unit of Emergency Department Naval Hospital DR Ramelan, SurabayaNabilaNo ratings yet
- FamiliesDocument26 pagesFamiliesChaoukiNo ratings yet
- Transducer Engineering 2 Marks With AnswersDocument13 pagesTransducer Engineering 2 Marks With AnswersSridharan DNo ratings yet
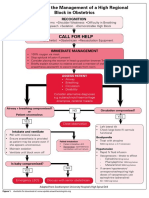
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- 29102015000000B - Boehler DCMS-IG - SWDocument1 page29102015000000B - Boehler DCMS-IG - SWErdinc BayatNo ratings yet
- NIPON STEEL Solution For Offshore Oil and GasDocument21 pagesNIPON STEEL Solution For Offshore Oil and GasCharwin XiaoNo ratings yet
- Pressure Conversion ChartDocument1 pagePressure Conversion Chartamarkore3486No ratings yet
- Condenser Sizing CalculationDocument21 pagesCondenser Sizing CalculationShruti Sharma100% (4)
- Radioactivity UitmDocument25 pagesRadioactivity UitmMoody6861No ratings yet
- (MRCP Study Guides) S. Hughes - Complete Data Interpretation For The MRCP-Churchill Livingstone (2001)Document2 pages(MRCP Study Guides) S. Hughes - Complete Data Interpretation For The MRCP-Churchill Livingstone (2001)basocdovnch0% (1)
- About Drill CasingDocument2 pagesAbout Drill CasingMmadu Vivian ChiamakaNo ratings yet
- Sebi GuidelinesDocument16 pagesSebi GuidelinesJerome P100% (1)
- COVID-19 and Disinfectants and Sanitizers in Food PremisesDocument5 pagesCOVID-19 and Disinfectants and Sanitizers in Food Premisesnur atiqah sobriNo ratings yet
- Susan Sugarman - Freud's Interpretation of Dreams - A Reappraisal-Cambridge University Press (2022)Document195 pagesSusan Sugarman - Freud's Interpretation of Dreams - A Reappraisal-Cambridge University Press (2022)Rodolfo Ferronatto De SouzaNo ratings yet
- (Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFDocument42 pages(Download PDF) The Monstrous Feminine in Contemporary Japanese Popular Culture Raechel Dumas Online Ebook All Chapter PDFdavid.messer693100% (15)
- AA Allen - Deliver MeDocument86 pagesAA Allen - Deliver Mecaren ronoNo ratings yet
- Emax 2222Document85 pagesEmax 2222camNo ratings yet
- Parables of Jesus Net BibleDocument2 pagesParables of Jesus Net Bibleapi-174346096No ratings yet
- G2C & B2C Services: Telecentre Entrepreneur CourseDocument6 pagesG2C & B2C Services: Telecentre Entrepreneur CourseKarthik VanamNo ratings yet
- Optical Processes and Excitons: RamanDocument26 pagesOptical Processes and Excitons: RamanDiana HSNo ratings yet
- Env LawDocument16 pagesEnv LawHeena ShaikhNo ratings yet
- Geography Mock Test PopulationDocument8 pagesGeography Mock Test PopulationMain AccountNo ratings yet
- Internship Report Shamim and CompanyDocument74 pagesInternship Report Shamim and CompanyUsman Niazi100% (1)
- Whitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USEDocument6 pagesWhitesboro Isd - 1995 TEXAS SCHOOL SURVEY OF DRUG AND ALCOHOL USETexas School Survey of Drug and Alcohol UseNo ratings yet
- ToxicologyDocument197 pagesToxicologyRichelle Dianne Ramos-Giang100% (6)
- Clinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseDocument4 pagesClinical Nutrition: Paediatric Nutrition Risk Scores in Clinical Practice: Children With Inflammatory Bowel DiseaseMaggie S HungNo ratings yet
- Waiters and WaitressesDocument2 pagesWaiters and WaitressesJaylord Susas GuitguitNo ratings yet
- Pyara Paneer: IngredientsDocument54 pagesPyara Paneer: IngredientsRashmi PrakashNo ratings yet
- Computerised Wheel Balancer Computerised Wheel BalancerDocument2 pagesComputerised Wheel Balancer Computerised Wheel Balancervivek dongareNo ratings yet