Download as pdf or txt
You might also like
- AWHONN High-Risk & Critical Care Obstetrics (2012)Document440 pagesAWHONN High-Risk & Critical Care Obstetrics (2012)Rima Hajjar100% (2)
- Chemistry: 1.tietz Textbook of Clinical Chemistry and Molecular Diagnostics, Fourth Edition, Page 861Document1 pageChemistry: 1.tietz Textbook of Clinical Chemistry and Molecular Diagnostics, Fourth Edition, Page 861Tauqeer AbbasNo ratings yet
- Breast CancerDocument1 pageBreast CancerDhruva PatelNo ratings yet
- G GDMDocument46 pagesG GDMtimworkmakesthedreamworkNo ratings yet
- Gestational Hypertension and Preeclampsia ACOG.46Document24 pagesGestational Hypertension and Preeclampsia ACOG.46UWIMANA Jean ClaudeNo ratings yet
- Pil 8098Document2 pagesPil 8098NE LandlordNo ratings yet
- GalactosemiaDocument13 pagesGalactosemiaCezaraDianaNo ratings yet
- Management of Diabetes Mellitus: Principles and Practice : Review ArticleDocument12 pagesManagement of Diabetes Mellitus: Principles and Practice : Review ArticlefaustoNo ratings yet
- Name of The Drug 1Document2 pagesName of The Drug 1Jhyrha Camille FelixNo ratings yet
- Name of The Drug Mechanism of Action Indications Contraindications Side Effects Adverse Reaction Nursing Considerations Generic NameDocument2 pagesName of The Drug Mechanism of Action Indications Contraindications Side Effects Adverse Reaction Nursing Considerations Generic NameJhyrha Camille FelixNo ratings yet
- Clinical Course and Management of Acute and Chronic Viral Hepatitis During PregnancyDocument9 pagesClinical Course and Management of Acute and Chronic Viral Hepatitis During PregnancyalexandresarradeyNo ratings yet
- Diabetes GestacionalDocument1 pageDiabetes GestacionalAna ApolinárioNo ratings yet
- Gestational Diabetes Mellitus: Maternity and Neonatal Clinical GuidelineDocument38 pagesGestational Diabetes Mellitus: Maternity and Neonatal Clinical GuidelineRetno SumaraNo ratings yet
- Polyethylene Glycol For Constipation in Children Younger Than Eighteen Months OldDocument3 pagesPolyethylene Glycol For Constipation in Children Younger Than Eighteen Months OldJose SalazarNo ratings yet
- Article - 1527759232 2Document5 pagesArticle - 1527759232 2Raghu Teja M VNo ratings yet
- Professionals DM Module1Document2 pagesProfessionals DM Module1Ching Tsz ShanNo ratings yet
- DM Pada KehamilanDocument20 pagesDM Pada KehamilanasumaacocoNo ratings yet
- Diabetes in PregnancyDocument13 pagesDiabetes in Pregnancyahmad ridzuanNo ratings yet
- Acceptance and Commitment Therapy ACT For Adult TyDocument8 pagesAcceptance and Commitment Therapy ACT For Adult TyVeronicaNo ratings yet
- TestDocument1 pageTestnurul wahyuniNo ratings yet
- PDF Surgical Prophylaxis Poster Dec 2021Document1 pagePDF Surgical Prophylaxis Poster Dec 2021Midhun KishorNo ratings yet
- MetforminDocument2 pagesMetforminEdem LeeNo ratings yet
- R2-Vo3No6Document6 pagesR2-Vo3No6LusianaTasyaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyinjilbalazoNo ratings yet
- DM in PregnancyDocument3 pagesDM in PregnancyherbsdoktaNo ratings yet
- Hunt2018Global CareDocument9 pagesHunt2018Global CareDwi RahmawatiNo ratings yet
- Usfda (2019 - 07 - 17 07 - 17 - 12 UTC)Document175 pagesUsfda (2019 - 07 - 17 07 - 17 - 12 UTC)pavanNo ratings yet
- 11092022119226070042Document9 pages11092022119226070042Alya BarrotNo ratings yet
- Midwifery Pharmacology-4Document1 pageMidwifery Pharmacology-4georgeloto12No ratings yet
- Drug Study Misoprostol PDFDocument5 pagesDrug Study Misoprostol PDFSteffiNo ratings yet
- Articulo 3Document12 pagesArticulo 3Emma PrietoNo ratings yet
- Targocid PDFDocument2 pagesTargocid PDFwahyu agung yuwonoNo ratings yet
- Note 26 Oct 2023Document4 pagesNote 26 Oct 2023Muna HassanNo ratings yet
- Nutrition in Pregnancy A Comparative Review Of.19Document11 pagesNutrition in Pregnancy A Comparative Review Of.19mehrdadrahi258miNo ratings yet
- Basalog One PiDocument2 pagesBasalog One Pipratibha.turitoNo ratings yet
- Kangaroo Mother Program An Alternative Way of Caring For Low Birth Weight InfantsDocument9 pagesKangaroo Mother Program An Alternative Way of Caring For Low Birth Weight InfantsFerroNo ratings yet
- Cues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationDocument3 pagesCues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationLouwella RamosNo ratings yet
- Prevention & Early Outpatient Treatment Protocol For Covid-19Document4 pagesPrevention & Early Outpatient Treatment Protocol For Covid-19jack mehiffNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Does Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialDocument6 pagesDoes Exercise Training During Pregnancy Affect Gestational Age? A Randomised Controlled TrialTrnidad Moder GarvizoNo ratings yet
- ParacetamolDocument3 pagesParacetamolgersalia.christiennikkiNo ratings yet
- Drug Study: Phinma - University of Iloilo College of Allied Health SciencesDocument3 pagesDrug Study: Phinma - University of Iloilo College of Allied Health Scienceslhie cabanlitNo ratings yet
- First Trimester Screening For Preeclampsia An.6Document8 pagesFirst Trimester Screening For Preeclampsia An.6ronaNo ratings yet
- Once-Weekly Semaglutide in Adolescents With Obesity: Original ArticleDocument13 pagesOnce-Weekly Semaglutide in Adolescents With Obesity: Original ArticleAndrés HerrónNo ratings yet
- Diabetes in PregnancyDocument3 pagesDiabetes in Pregnancyspatel15072002No ratings yet
- Aminoglycoside Guideline For Children-2Document7 pagesAminoglycoside Guideline For Children-2Alina CaraciobanuNo ratings yet
- CMC - GDM TransDocument13 pagesCMC - GDM TransRalph AlbertoNo ratings yet
- Gastrointestinal Decontamination of Poisoned PatientDocument14 pagesGastrointestinal Decontamination of Poisoned Patientadm kdmyNo ratings yet
- Award 1Document9 pagesAward 1andreiafernandesmeciaNo ratings yet
- Red Book 9th Edition Lifecycle Charts v2Document2 pagesRed Book 9th Edition Lifecycle Charts v2Shahriar Kabir DaneNo ratings yet
- Gestational Diabetes Education and Diabetes Prevention StrategiesDocument5 pagesGestational Diabetes Education and Diabetes Prevention StrategiesEsha KuttiNo ratings yet
- Diabetes in Pregnancy My Notes(PDF)Document5 pagesDiabetes in Pregnancy My Notes(PDF)001mahwishNo ratings yet
- Drug Study 2Document2 pagesDrug Study 2HeavenNo ratings yet
- Endometrin Corvera Drug-StudyDocument3 pagesEndometrin Corvera Drug-Studykkd nyleNo ratings yet
- A Guide To Sudoscan NewDocument7 pagesA Guide To Sudoscan NewLaura B. BautistaNo ratings yet
- Drug StudyDocument7 pagesDrug Studychandria0026No ratings yet
- Metformin Vs Insulin in Gestational DiabetesDocument17 pagesMetformin Vs Insulin in Gestational Diabetesmiguel alejandro zapata olayaNo ratings yet
- A Review of Current Trends With Type 2 Diabetes Epidemiology, Aetiology, Pathogenesis, Treatments and Future PerspectivesDocument36 pagesA Review of Current Trends With Type 2 Diabetes Epidemiology, Aetiology, Pathogenesis, Treatments and Future PerspectivescastillojessNo ratings yet
- Exposys Data Labs: Internship Report On Data Science ProjectDocument23 pagesExposys Data Labs: Internship Report On Data Science ProjectDhyeayaNo ratings yet
- Gentamicin in NeonatusDocument9 pagesGentamicin in NeonatusSalsabila RaniahNo ratings yet
- STIDocument53 pagesSTIRima HajjarNo ratings yet
- Preterm Labour (PTL) : Antenatal CareDocument10 pagesPreterm Labour (PTL) : Antenatal CareRima HajjarNo ratings yet
- IncontinenceDocument34 pagesIncontinenceRima HajjarNo ratings yet
- Breast MassesDocument25 pagesBreast MassesRima HajjarNo ratings yet
- CREOG2Document1 pageCREOG2Rima HajjarNo ratings yet
- Obstetric Cholestasis (OC) : MaternalDocument3 pagesObstetric Cholestasis (OC) : MaternalRima HajjarNo ratings yet
- Pre-Eclampsia PET and EclampsiaDocument7 pagesPre-Eclampsia PET and EclampsiaRima HajjarNo ratings yet
- Abnormal Uterine BleedingDocument18 pagesAbnormal Uterine BleedingRima HajjarNo ratings yet
- Antenatal CareDocument7 pagesAntenatal CareRima HajjarNo ratings yet
- Case DISCUSSIONDocument2 pagesCase DISCUSSIONRima HajjarNo ratings yet
- Different Prostaglandin FunctionsDocument1 pageDifferent Prostaglandin FunctionsRima HajjarNo ratings yet
- CREOGGYNREVIEW PP PDFDocument98 pagesCREOGGYNREVIEW PP PDFRima HajjarNo ratings yet
- Step 1 REVIEWDocument140 pagesStep 1 REVIEWRima HajjarNo ratings yet
- Pachychoroid PDFDocument9 pagesPachychoroid PDFRima HajjarNo ratings yet
- Alternate Dosing Protocol For Magnesium Sulfate In.18 PDFDocument5 pagesAlternate Dosing Protocol For Magnesium Sulfate In.18 PDFRima HajjarNo ratings yet
- Early Pregnancy LossDocument20 pagesEarly Pregnancy LossRima HajjarNo ratings yet
- 2015 Oncology CREOG Review PDFDocument76 pages2015 Oncology CREOG Review PDFRima HajjarNo ratings yet
- The Autonomic Nervous System (ANS) : K, S & J, CH 47 HandoutDocument27 pagesThe Autonomic Nervous System (ANS) : K, S & J, CH 47 HandoutRima HajjarNo ratings yet
- Bleeding Dr. Sally Temraz - March 2, 2015Document1 pageBleeding Dr. Sally Temraz - March 2, 2015Rima HajjarNo ratings yet
- Premature Rupture of Membranes PromDocument15 pagesPremature Rupture of Membranes PromRima HajjarNo ratings yet
- Pathway DMDocument2 pagesPathway DMBang KiraNo ratings yet
- Diabetic ComaDocument15 pagesDiabetic ComaNader Smadi100% (1)
- HipothyroidDocument48 pagesHipothyroidCakraEkkyNo ratings yet
- Asterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriDocument5 pagesAsterisa Retno Putri-Comprehensive Management of Young Children With Severe Diabetic Ketoacidosis (DKA) - PPT - Asterisa PutriAdrian KhomanNo ratings yet
- Nisha DeviDocument2 pagesNisha DeviSantan Lal DasNo ratings yet
- Insulin Pump ManagementDocument18 pagesInsulin Pump ManagementFelipe Scipiao MouraNo ratings yet
- Lesson Plan ON Diabetes Mellitus: Presented by Swatilekha DasDocument6 pagesLesson Plan ON Diabetes Mellitus: Presented by Swatilekha Dasramzan aliNo ratings yet
- Insulin ShockDocument9 pagesInsulin ShockMarina CiburciuNo ratings yet
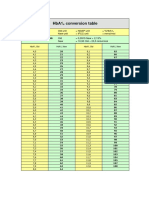
- HbA1cConversionTable PDFDocument1 pageHbA1cConversionTable PDFDarkoMaxNo ratings yet
- SUPP. ENDOCRINE QuestionsDocument3 pagesSUPP. ENDOCRINE QuestionsronaronixstheboyNo ratings yet
- Standards of Medical Care in Diabetes - 2022: 9. Pharmacologic Approaches To Glycemic TreatmentDocument19 pagesStandards of Medical Care in Diabetes - 2022: 9. Pharmacologic Approaches To Glycemic TreatmentAdina SimionNo ratings yet
- References WBCDocument2 pagesReferences WBCMiguelito Galagar GultianoNo ratings yet
- Practical Clinical Endocrinology 2021Document523 pagesPractical Clinical Endocrinology 2021Morozovschi VitalieNo ratings yet
- SN Erra Fazira Jururawat Terlatih U29 Jabatan Kecemasan, HAT Wilayah Kota KinabaluDocument14 pagesSN Erra Fazira Jururawat Terlatih U29 Jabatan Kecemasan, HAT Wilayah Kota Kinabaluyein yenNo ratings yet
- HYPOTHYROIDISMDocument11 pagesHYPOTHYROIDISMVarun SinghNo ratings yet
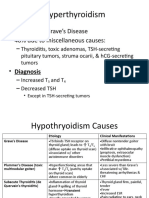
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet
- MCQDocument20 pagesMCQanuj sharma100% (3)
- Flayer 27 Mei Deep Surabaya 3 - 1Document2 pagesFlayer 27 Mei Deep Surabaya 3 - 1Dian SafitrianaNo ratings yet
- Diabetes Mellitus DescritionDocument5 pagesDiabetes Mellitus DescritionTinke WinkeNo ratings yet
- Addison+conn+cush+feo+adr IncidentalomaDocument65 pagesAddison+conn+cush+feo+adr IncidentalomaMjn BausatNo ratings yet
- Thyroid Testing Using RaiDocument8 pagesThyroid Testing Using RaideblackaNo ratings yet
- Indications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)Document8 pagesIndications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)IJAR JOURNALNo ratings yet
- Glycemic Targets: American Diabetes AssociationDocument8 pagesGlycemic Targets: American Diabetes AssociationHelenaNo ratings yet
- Diabetes: Dr. Hermawan Susanto SPPDDocument66 pagesDiabetes: Dr. Hermawan Susanto SPPDAbdur RohmanNo ratings yet
- Preethi Mukundan Pitch 081816Document4 pagesPreethi Mukundan Pitch 081816api-336055432No ratings yet
- Thyroid Function TestsDocument9 pagesThyroid Function Testsmdowl90No ratings yet
- Shaharyar Ansari: Report Status: FinalDocument3 pagesShaharyar Ansari: Report Status: FinalAutonomous Alfa100% (1)
- JURNAL VINKA - RemovedDocument8 pagesJURNAL VINKA - Removeduda photocopy PerintisNo ratings yet
- Diabetes Viva QuestionsDocument2 pagesDiabetes Viva QuestionsSara RezaNo ratings yet