
ABCDE Emergency Scenarios - OSCE Revision
ABCDE Emergency Scenarios - OSCE Revision
You might also like
- Confirmation of Satanding PDFDocument3 pagesConfirmation of Satanding PDFDavidForloyoNo ratings yet
- Neurology For MRCP PACESDocument137 pagesNeurology For MRCP PACESOmarAlbeshrei100% (1)
- Latihan ATLSDocument28 pagesLatihan ATLSDesy Faridah100% (6)
- Job DescriptionDocument10 pagesJob Descriptionpioneer92No ratings yet
- Original Research Abstract AFCC ASMIHA 2019Document82 pagesOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- NBME 7 KeyDocument6 pagesNBME 7 KeyQaim ShahNo ratings yet
- Residency: Called - To.See - Patient V1.1Document111 pagesResidency: Called - To.See - Patient V1.1Glen OngNo ratings yet
- OSCE EmergencyDocument26 pagesOSCE EmergencyXu PeihaoNo ratings yet
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Station 2 Scenario PackDocument82 pagesStation 2 Scenario Packsarah premrajNo ratings yet
- MBChB4 5PastPapersDocument172 pagesMBChB4 5PastPapersHariharan NarendranNo ratings yet
- CBT - Emergency Medicine EditedDocument14 pagesCBT - Emergency Medicine Editedchristy INo ratings yet
- Investigations Management Notes For FinalsDocument138 pagesInvestigations Management Notes For FinalsThistell ThistleNo ratings yet
- The Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesDocument112 pagesThe Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesWonjoo LeeNo ratings yet
- JVP - WL GanDocument1 pageJVP - WL GanWeh Loong GanNo ratings yet
- Mark Schemes 1Document27 pagesMark Schemes 1crampuppy100% (2)
- ECG Made Easy - J HamptonDocument78 pagesECG Made Easy - J Hamptonkabal321100% (1)
- PRES MCQsDocument218 pagesPRES MCQsdoctorbilalsNo ratings yet
- Vaginal Swabs OSCE Guide PDFDocument8 pagesVaginal Swabs OSCE Guide PDFParsaant SinghNo ratings yet
- Top Tips For MRCGP CSA Exam P1 PDFDocument3 pagesTop Tips For MRCGP CSA Exam P1 PDFSalah ElbadawyNo ratings yet
- Foundation SJT CourseDocument9 pagesFoundation SJT Courseemedica coursesNo ratings yet
- OSCE Skills 2013 1Document141 pagesOSCE Skills 2013 1Haseeb RayhanNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet
- Heyson Notes IntegratedDocument327 pagesHeyson Notes Integratedproudofsky100% (2)
- PRO III 2012 Long Case (Surgical)Document39 pagesPRO III 2012 Long Case (Surgical)vijayaNo ratings yet
- MRCGPLeafletDocument4 pagesMRCGPLeafletAbubaker Mukhtar El SiddigNo ratings yet
- Abcdefg1983 PDFDocument769 pagesAbcdefg1983 PDFmohNo ratings yet
- Six Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurDocument16 pagesSix Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurNimisha Balakrishnan100% (1)
- How To Pass The MRCS PresentationDocument27 pagesHow To Pass The MRCS PresentationNurhusein KedirNo ratings yet
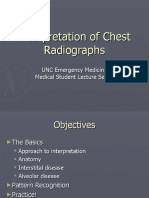
- Interpretation of Chest RadiographsDocument37 pagesInterpretation of Chest RadiographsAnshul JainNo ratings yet
- Basic Chest X-Ray Interpretation: Eliana MuisDocument58 pagesBasic Chest X-Ray Interpretation: Eliana MuiselianaNo ratings yet
- R 5th Year OSCE - Part 2Document230 pagesR 5th Year OSCE - Part 2Leon RajanthiranNo ratings yet
- Paediatrics SbaDocument34 pagesPaediatrics SbaAhmad Syahmi YZ100% (1)
- Lesson Plan Human Reproductive SystemDocument2 pagesLesson Plan Human Reproductive SystemGarnis HakimNo ratings yet
- Amc CourseoverviewDocument10 pagesAmc CourseoverviewRana Saddaqat HayatNo ratings yet
- Khidir DevelopmentDocument72 pagesKhidir DevelopmentMahmoud AbouelsoudNo ratings yet
- MRCP 1.doc 2Document70 pagesMRCP 1.doc 2Rasha Abduldaiem Elmalik100% (1)
- 2 Approach To The Neuro Exam Feb 2011Document35 pages2 Approach To The Neuro Exam Feb 2011suaqaziNo ratings yet
- #Sample Questions SBA - Paed 2011Document1 page#Sample Questions SBA - Paed 2011Asif ZarkNo ratings yet
- Medical InvestigationsDocument7 pagesMedical InvestigationsmedpgnotesNo ratings yet
- ABCDE ManagementDocument26 pagesABCDE ManagementHilmy Haydar El-FauzyNo ratings yet
- Almostadoctor - co.uk-OSCE ChecklistDocument10 pagesAlmostadoctor - co.uk-OSCE ChecklistJonathan YoungNo ratings yet
- Ammar Alani - AMC Clinical - 14.3.2018 Cases - My ApproachDocument6 pagesAmmar Alani - AMC Clinical - 14.3.2018 Cases - My ApproachqurbanNo ratings yet
- Sarishka Singh - ECG For PLAB 1Document5 pagesSarishka Singh - ECG For PLAB 1cnshariff@gmail.comNo ratings yet
- Comment On Dressing or Bandages and Take Them Down, Comment On ScarsDocument4 pagesComment On Dressing or Bandages and Take Them Down, Comment On ScarsGNo ratings yet
- Preparation CCFP Exam PowerpointDocument24 pagesPreparation CCFP Exam PowerpointPeterbb HelmanNo ratings yet
- Course Rules VS20171215 V3.1Document26 pagesCourse Rules VS20171215 V3.1CornelNo ratings yet
- MRCP Paces Chest RedclifffDocument13 pagesMRCP Paces Chest RedclifffIsmail H ANo ratings yet
- Past Paper (No Answer)Document170 pagesPast Paper (No Answer)Hariharan NarendranNo ratings yet
- Emrcs SurgeryDocument145 pagesEmrcs Surgerydanish balochNo ratings yet
- DR Swamy PLAB Courses LTD.: Plab 1 Mock Test: 5 March 2019 Time Allowed: 3HrsDocument31 pagesDR Swamy PLAB Courses LTD.: Plab 1 Mock Test: 5 March 2019 Time Allowed: 3HrsSualeha SohailNo ratings yet
- Cardiothoracic Surgery v1.0Document19 pagesCardiothoracic Surgery v1.0Ko YeKhaeNo ratings yet
- Amc ConversationDocument13 pagesAmc Conversationprofarmah6150No ratings yet
- 2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFDocument1 page2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFms_lezahNo ratings yet
- Suatu Alat Laboratoris Alat Bantu DiagnosisDocument78 pagesSuatu Alat Laboratoris Alat Bantu DiagnosisAnonymous 3LwVkUsdNo ratings yet
- Austin Evidence Based CVDocument2 pagesAustin Evidence Based CVtjelongNo ratings yet
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
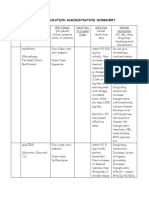
- Medication Administration WorksheetDocument6 pagesMedication Administration WorksheetCheska CarrionNo ratings yet
- Vegetarian Diet, Seventh Day Adventists and Risk of CardiovascularDocument7 pagesVegetarian Diet, Seventh Day Adventists and Risk of CardiovascularJohn SammutNo ratings yet
- Biology 2nd Paper Zoology Suggestion For 1st Year Final Exam EVDocument2 pagesBiology 2nd Paper Zoology Suggestion For 1st Year Final Exam EVkingjordi82No ratings yet
- Literature Review of HypertensionDocument7 pagesLiterature Review of Hypertensionafmzatvuipwdal100% (1)
- Testavan SPCDocument4 pagesTestavan SPCMoussa AmerNo ratings yet
- New Case of Pre-EclampsiaDocument13 pagesNew Case of Pre-EclampsiaKristine AlejandroNo ratings yet
- P-Mid Midterm ExamDocument10 pagesP-Mid Midterm ExamIan Mizzel A. DulfinaNo ratings yet
- Handbook of Obstetric MedicineDocument15 pagesHandbook of Obstetric MedicineSara Zoi Lu50% (2)
- Central Nervous SystemDocument25 pagesCentral Nervous SystemKhairulbariah AhmadNo ratings yet
- Drug Study NotesDocument3 pagesDrug Study NotesCristoper BodionganNo ratings yet
- Aortic DissectionDocument67 pagesAortic DissectionPIYALI BISWASNo ratings yet
- Case-Study-On-Pulmonary EdemaDocument100 pagesCase-Study-On-Pulmonary EdemaLouie MansaNo ratings yet
- Soal Ikfr Unair 2019 - EditDocument5 pagesSoal Ikfr Unair 2019 - EditFusarina MumpuniNo ratings yet
- Case Study3Document13 pagesCase Study3Nadine FormaranNo ratings yet
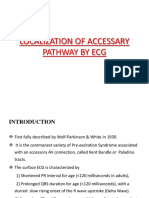
- Localization of Accessary Pathway by EcgDocument63 pagesLocalization of Accessary Pathway by Ecgdini_angginiNo ratings yet
- hemiplegia دكتور عزونيDocument4 pageshemiplegia دكتور عزونيRaed AlhnaityNo ratings yet
- Pancreatic Hormones & Antidiabetic Drugs: Case StudyDocument31 pagesPancreatic Hormones & Antidiabetic Drugs: Case StudyMae Lislie Canonigo - FloresNo ratings yet
- Coronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdDocument99 pagesCoronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdMwanja MosesNo ratings yet
- WRLD HRT DayDocument24 pagesWRLD HRT Daydas_s13No ratings yet
- Exercise ECGDocument85 pagesExercise ECGSUHER ANUNo ratings yet
- Cholesterol Risk ChartDocument2 pagesCholesterol Risk ChartNishantha SenaratneNo ratings yet
- 2016 Jarle Jorveit Sudden Cardiac DeathDocument48 pages2016 Jarle Jorveit Sudden Cardiac DeathArassikaNo ratings yet
- Take One Nursing Final Coaching Ms CriticalDocument29 pagesTake One Nursing Final Coaching Ms Criticalnot your medz duranNo ratings yet
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- Prone Positioning: What'S New in Intensive CareDocument3 pagesProne Positioning: What'S New in Intensive Careamandanbatista10No ratings yet
- Solitaire Company ProfileDocument71 pagesSolitaire Company ProfilesolitairepharmaciaNo ratings yet
- Electric ShockDocument4 pagesElectric ShockTamjid Kabir100% (1)























































































Download as pdf or txt
You might also like
- Confirmation of Satanding PDFDocument3 pagesConfirmation of Satanding PDFDavidForloyoNo ratings yet
- Neurology For MRCP PACESDocument137 pagesNeurology For MRCP PACESOmarAlbeshrei100% (1)
- Latihan ATLSDocument28 pagesLatihan ATLSDesy Faridah100% (6)
- Job DescriptionDocument10 pagesJob Descriptionpioneer92No ratings yet
- Original Research Abstract AFCC ASMIHA 2019Document82 pagesOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- NBME 7 KeyDocument6 pagesNBME 7 KeyQaim ShahNo ratings yet
- Residency: Called - To.See - Patient V1.1Document111 pagesResidency: Called - To.See - Patient V1.1Glen OngNo ratings yet
- OSCE EmergencyDocument26 pagesOSCE EmergencyXu PeihaoNo ratings yet
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Station 2 Scenario PackDocument82 pagesStation 2 Scenario Packsarah premrajNo ratings yet
- MBChB4 5PastPapersDocument172 pagesMBChB4 5PastPapersHariharan NarendranNo ratings yet
- CBT - Emergency Medicine EditedDocument14 pagesCBT - Emergency Medicine Editedchristy INo ratings yet
- Investigations Management Notes For FinalsDocument138 pagesInvestigations Management Notes For FinalsThistell ThistleNo ratings yet
- The Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesDocument112 pagesThe Ukfpo Clinical Assessment Examination Guide by Sarishka Singh Plab ResourcesWonjoo LeeNo ratings yet
- JVP - WL GanDocument1 pageJVP - WL GanWeh Loong GanNo ratings yet
- Mark Schemes 1Document27 pagesMark Schemes 1crampuppy100% (2)
- ECG Made Easy - J HamptonDocument78 pagesECG Made Easy - J Hamptonkabal321100% (1)
- PRES MCQsDocument218 pagesPRES MCQsdoctorbilalsNo ratings yet
- Vaginal Swabs OSCE Guide PDFDocument8 pagesVaginal Swabs OSCE Guide PDFParsaant SinghNo ratings yet
- Top Tips For MRCGP CSA Exam P1 PDFDocument3 pagesTop Tips For MRCGP CSA Exam P1 PDFSalah ElbadawyNo ratings yet
- Foundation SJT CourseDocument9 pagesFoundation SJT Courseemedica coursesNo ratings yet
- OSCE Skills 2013 1Document141 pagesOSCE Skills 2013 1Haseeb RayhanNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet
- Heyson Notes IntegratedDocument327 pagesHeyson Notes Integratedproudofsky100% (2)
- PRO III 2012 Long Case (Surgical)Document39 pagesPRO III 2012 Long Case (Surgical)vijayaNo ratings yet
- MRCGPLeafletDocument4 pagesMRCGPLeafletAbubaker Mukhtar El SiddigNo ratings yet
- Abcdefg1983 PDFDocument769 pagesAbcdefg1983 PDFmohNo ratings yet
- Six Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurDocument16 pagesSix Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurNimisha Balakrishnan100% (1)
- How To Pass The MRCS PresentationDocument27 pagesHow To Pass The MRCS PresentationNurhusein KedirNo ratings yet
- Interpretation of Chest RadiographsDocument37 pagesInterpretation of Chest RadiographsAnshul JainNo ratings yet
- Basic Chest X-Ray Interpretation: Eliana MuisDocument58 pagesBasic Chest X-Ray Interpretation: Eliana MuiselianaNo ratings yet
- R 5th Year OSCE - Part 2Document230 pagesR 5th Year OSCE - Part 2Leon RajanthiranNo ratings yet
- Paediatrics SbaDocument34 pagesPaediatrics SbaAhmad Syahmi YZ100% (1)
- Lesson Plan Human Reproductive SystemDocument2 pagesLesson Plan Human Reproductive SystemGarnis HakimNo ratings yet
- Amc CourseoverviewDocument10 pagesAmc CourseoverviewRana Saddaqat HayatNo ratings yet
- Khidir DevelopmentDocument72 pagesKhidir DevelopmentMahmoud AbouelsoudNo ratings yet
- MRCP 1.doc 2Document70 pagesMRCP 1.doc 2Rasha Abduldaiem Elmalik100% (1)
- 2 Approach To The Neuro Exam Feb 2011Document35 pages2 Approach To The Neuro Exam Feb 2011suaqaziNo ratings yet
- #Sample Questions SBA - Paed 2011Document1 page#Sample Questions SBA - Paed 2011Asif ZarkNo ratings yet
- Medical InvestigationsDocument7 pagesMedical InvestigationsmedpgnotesNo ratings yet
- ABCDE ManagementDocument26 pagesABCDE ManagementHilmy Haydar El-FauzyNo ratings yet
- Almostadoctor - co.uk-OSCE ChecklistDocument10 pagesAlmostadoctor - co.uk-OSCE ChecklistJonathan YoungNo ratings yet
- Ammar Alani - AMC Clinical - 14.3.2018 Cases - My ApproachDocument6 pagesAmmar Alani - AMC Clinical - 14.3.2018 Cases - My ApproachqurbanNo ratings yet
- Sarishka Singh - ECG For PLAB 1Document5 pagesSarishka Singh - ECG For PLAB 1cnshariff@gmail.comNo ratings yet
- Comment On Dressing or Bandages and Take Them Down, Comment On ScarsDocument4 pagesComment On Dressing or Bandages and Take Them Down, Comment On ScarsGNo ratings yet
- Preparation CCFP Exam PowerpointDocument24 pagesPreparation CCFP Exam PowerpointPeterbb HelmanNo ratings yet
- Course Rules VS20171215 V3.1Document26 pagesCourse Rules VS20171215 V3.1CornelNo ratings yet
- MRCP Paces Chest RedclifffDocument13 pagesMRCP Paces Chest RedclifffIsmail H ANo ratings yet
- Past Paper (No Answer)Document170 pagesPast Paper (No Answer)Hariharan NarendranNo ratings yet
- Emrcs SurgeryDocument145 pagesEmrcs Surgerydanish balochNo ratings yet
- DR Swamy PLAB Courses LTD.: Plab 1 Mock Test: 5 March 2019 Time Allowed: 3HrsDocument31 pagesDR Swamy PLAB Courses LTD.: Plab 1 Mock Test: 5 March 2019 Time Allowed: 3HrsSualeha SohailNo ratings yet
- Cardiothoracic Surgery v1.0Document19 pagesCardiothoracic Surgery v1.0Ko YeKhaeNo ratings yet
- Amc ConversationDocument13 pagesAmc Conversationprofarmah6150No ratings yet
- 2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFDocument1 page2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFms_lezahNo ratings yet
- Suatu Alat Laboratoris Alat Bantu DiagnosisDocument78 pagesSuatu Alat Laboratoris Alat Bantu DiagnosisAnonymous 3LwVkUsdNo ratings yet
- Austin Evidence Based CVDocument2 pagesAustin Evidence Based CVtjelongNo ratings yet
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Medication Administration WorksheetDocument6 pagesMedication Administration WorksheetCheska CarrionNo ratings yet
- Vegetarian Diet, Seventh Day Adventists and Risk of CardiovascularDocument7 pagesVegetarian Diet, Seventh Day Adventists and Risk of CardiovascularJohn SammutNo ratings yet
- Biology 2nd Paper Zoology Suggestion For 1st Year Final Exam EVDocument2 pagesBiology 2nd Paper Zoology Suggestion For 1st Year Final Exam EVkingjordi82No ratings yet
- Literature Review of HypertensionDocument7 pagesLiterature Review of Hypertensionafmzatvuipwdal100% (1)
- Testavan SPCDocument4 pagesTestavan SPCMoussa AmerNo ratings yet
- New Case of Pre-EclampsiaDocument13 pagesNew Case of Pre-EclampsiaKristine AlejandroNo ratings yet
- P-Mid Midterm ExamDocument10 pagesP-Mid Midterm ExamIan Mizzel A. DulfinaNo ratings yet
- Handbook of Obstetric MedicineDocument15 pagesHandbook of Obstetric MedicineSara Zoi Lu50% (2)
- Central Nervous SystemDocument25 pagesCentral Nervous SystemKhairulbariah AhmadNo ratings yet
- Drug Study NotesDocument3 pagesDrug Study NotesCristoper BodionganNo ratings yet
- Aortic DissectionDocument67 pagesAortic DissectionPIYALI BISWASNo ratings yet
- Case-Study-On-Pulmonary EdemaDocument100 pagesCase-Study-On-Pulmonary EdemaLouie MansaNo ratings yet
- Soal Ikfr Unair 2019 - EditDocument5 pagesSoal Ikfr Unair 2019 - EditFusarina MumpuniNo ratings yet
- Case Study3Document13 pagesCase Study3Nadine FormaranNo ratings yet
- Localization of Accessary Pathway by EcgDocument63 pagesLocalization of Accessary Pathway by Ecgdini_angginiNo ratings yet
- hemiplegia دكتور عزونيDocument4 pageshemiplegia دكتور عزونيRaed AlhnaityNo ratings yet
- Pancreatic Hormones & Antidiabetic Drugs: Case StudyDocument31 pagesPancreatic Hormones & Antidiabetic Drugs: Case StudyMae Lislie Canonigo - FloresNo ratings yet
- Coronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdDocument99 pagesCoronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdMwanja MosesNo ratings yet
- WRLD HRT DayDocument24 pagesWRLD HRT Daydas_s13No ratings yet
- Exercise ECGDocument85 pagesExercise ECGSUHER ANUNo ratings yet
- Cholesterol Risk ChartDocument2 pagesCholesterol Risk ChartNishantha SenaratneNo ratings yet
- 2016 Jarle Jorveit Sudden Cardiac DeathDocument48 pages2016 Jarle Jorveit Sudden Cardiac DeathArassikaNo ratings yet
- Take One Nursing Final Coaching Ms CriticalDocument29 pagesTake One Nursing Final Coaching Ms Criticalnot your medz duranNo ratings yet
- List of Diseases Imo 2019 Cardio-RespiratoryDocument2 pagesList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraNo ratings yet
- Prone Positioning: What'S New in Intensive CareDocument3 pagesProne Positioning: What'S New in Intensive Careamandanbatista10No ratings yet
- Solitaire Company ProfileDocument71 pagesSolitaire Company ProfilesolitairepharmaciaNo ratings yet
- Electric ShockDocument4 pagesElectric ShockTamjid Kabir100% (1)