Professional Documents
Culture Documents
Anestesi Blok Mandibula
Anestesi Blok Mandibula
Uploaded by
hafid nugroho0 ratings0% found this document useful (0 votes)
781 views12 pagesThis document provides an overview of the preoperative assessment process. It discusses obtaining a thorough patient history, performing a physical exam including an airway assessment, determining ASA classification, and optimizing any medical conditions prior to surgery. Key monitoring equipment is also outlined, including pulse oximetry to measure oxygen saturation, capnography to monitor exhaled carbon dioxide, ECG to evaluate heart rate and rhythm, blood pressure monitoring, and peripheral nerve stimulation to assess muscle relaxation during procedures. The goal of the preoperative assessment is to identify and address any risk factors in order to reduce complications and optimize the patient's condition for surgery.
Original Description:
Original Title
ANESTESI BLOK MANDIBULA
Copyright
© Attribution Non-Commercial (BY-NC)
Available Formats
DOCX, PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentThis document provides an overview of the preoperative assessment process. It discusses obtaining a thorough patient history, performing a physical exam including an airway assessment, determining ASA classification, and optimizing any medical conditions prior to surgery. Key monitoring equipment is also outlined, including pulse oximetry to measure oxygen saturation, capnography to monitor exhaled carbon dioxide, ECG to evaluate heart rate and rhythm, blood pressure monitoring, and peripheral nerve stimulation to assess muscle relaxation during procedures. The goal of the preoperative assessment is to identify and address any risk factors in order to reduce complications and optimize the patient's condition for surgery.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
0 ratings0% found this document useful (0 votes)
781 views12 pagesAnestesi Blok Mandibula
Anestesi Blok Mandibula
Uploaded by
hafid nugrohoThis document provides an overview of the preoperative assessment process. It discusses obtaining a thorough patient history, performing a physical exam including an airway assessment, determining ASA classification, and optimizing any medical conditions prior to surgery. Key monitoring equipment is also outlined, including pulse oximetry to measure oxygen saturation, capnography to monitor exhaled carbon dioxide, ECG to evaluate heart rate and rhythm, blood pressure monitoring, and peripheral nerve stimulation to assess muscle relaxation during procedures. The goal of the preoperative assessment is to identify and address any risk factors in order to reduce complications and optimize the patient's condition for surgery.
Copyright:
Attribution Non-Commercial (BY-NC)
Available Formats
Download as DOCX, PDF, TXT or read online from Scribd
Download as docx, pdf, or txt
You are on page 1of 12
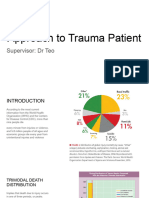
PREOPERATIVE ASSESSMENT • class 2 - able to visualize all of the above, except
❏ abnormal anatomy/physiology/metabolism and/or anterior andposterior tonsillar
concurrent medications can alter response to pillars are hidden by the tongue
anesthetic agents • class 3 - only the soft palate and base of the uvula are
❏ required prior to general and regional anesthesia and visible
conscious sedation • class 4 - only the soft palate can be seen (uvula not
❏ must document that risks and benefits have been visualized)
explained A12 – Anesthesia MCCQE 2002 Review Notes
❏ most regular medications (NB: antihypertensives and ANESTHESIA . . . CONT.
anti-anginals) continued with a few exceptions, Figure 2. Mallampati Classification
e.g. diuretics, oral hypoglycemics, anticoagulants, Drawing by Betty Lee
steroids, monamine oxidase inhibitors (MAOI), and ❏ bony landmarks and suitability of areas for regional
drugs with CNS side effects anesthesia if relevant
❏ optimization of medical treatment preoperatively will ❏ focus on CNS, CVS and respiratory (includes airway)
reduce peri- and postoperative complications systems
• diabetes mellitus (DM) - optimize glycemic control ❏ general e.g. nutritional, hydration, and mental status
• nutritional status - correct malnourished states ❏ pre-existing motor and sensory deficits
• smoking - encourage cessation ❏ sites for IV, central venous pressure (CVP) and
• obesity - encourage weight loss pulmonary artery (PA) catheters, regional anesthesia
• chronic obstructive pulmonary disease (COPD) - Investigations
optimize respiratory status, ❏ change in Public Hospitals Act: Hb and urinalysis no
teach postoperative exercises (e.g. incentive spirometry) longer required as routine in all patients pre-operatively
History ❏ hospital or departmental policies and patient
❏ previous anesthetic experience and complications, characteristics will dictate the necessity and/or
previous intubations, medications drug allergies, indications for tests such as chest x-ray, Hb, etc.
and allergies to topical preparations ❏ ECG often recommended for those > 40 years old
❏ focused review of systems ❏ preoperative pulmonary function tests for patients
• CNS - seizures, transient ischemic attack (TIA), with COPD, heavy smokers with history of persistent
cerebrovascular accident (CVA), cough, chest wall and spinal deformities, morbidly obese,
raised intracranial pressure (ICP), spinal disease, elderly (> 70), and patients for thoracic surgeries
arteriovenous malformation (AVM)/aneurysm, ❏ other investigations as clinically indicated
neuromuscular disease AMERICAN SOCIETY OF ANESTHESIOLOGY
• Resp - smoker, asthma, COPD, upper respiratory tract (ASA) CLASSIFICATION
infection (URTI), dyspnea, stridor ❏ common classification of physical status at time of
• cardiovascular (CVS) - angina/coronary artery disease surgery
(CAD), MI, HTN, congestive heart failure (CHF), ❏ a gross predictor of overall outcome, NOT used as
valvular disease, conditions requiring endocarditis stratification for anesthetic risk (mortality rates)
prophylaxis, arrhythmia, peripheral vascular disease • ASA 1: a healthy, fit patient (0.06-0.08%)
• GI - liver disease, gastroesophogeal reflux disease • ASA 2: a patient with mild systemic disease e.g.
(GERD), vomiting, diarrhea, last meal controlled Type 2 diabetes, controlled essential HTN,
• renal - insufficiency, dialysis obesity (0.27-0.4%), smoker
• hematologic - anemia, coagulation disorders, sickle cell • ASA 3: a patient with severe systemic disease that
• musculoskeletal (MSK) (arthritis - risk of C-spine limits activity, e.g. angina, prior MI,
subluxation during intubation) COPD (1.8-4.3%), DM, obesity
• endocrine - diabetes, thyroid, adrenal • ASA 4: a patient with incapacitating disease that is a
• other - morbid obesity, pregnancy, ethanol and drug use constant threat to life,
❏ family history of malignant hyperthermia, atypical e.g. CHF, renal failure, acute respiratory failure (7.8-
cholinesterase(pseudocholinesterase), 23%)
or other abnormal drug reactions • ASA 5: a moribund patient not expected to survive 24
Physical Examination hours with/without surgery,
❏ OROPHARYNX + AIRWAY assessment to e.g. ruptured abdominal aortic aneurysm (AAA), head
determine the likelihood of difficult intubation trauma with increased ICP (9.4-51%)
• no single test is specific or sensitive - all aid in ❏ for emergency operations, add the letter E after
determination of ease of intubation classification
• degree of mouth opening + TMJ subluxation ❏ from the history, physical exam, and
• jaw size (micro/retrognathia), "thyromental distance" labs/investigations the anesthetist can determine whether
• tongue size or not the
• posterior pharynx, tonsillar pillars, uvula easily visible patient is in OPTIMAL condition for the proposed
• dentition, dental appliances/prosthetics/caps - inform of surgical procedure
possibility of damage ❏ goal is to optimize the non-surgical disease states
• C-spine stability, neck flexion/extension prior to surgery
• tracheal deviation ❏ in emergency cases it is not always possible to
• nasal passage patency (if planning nasotracheal optimize coexistent or chronic disease states; goal is then
intubation) to
❏ Mallampati classification of airways (see Figure 2) accomplish what is possible in the time available
• class 1 - able to visualize soft palate, fauces, uvula, ant POSTOPERATIVE MANAGEMENT
and post tonsillar pillars
❏ usually begins in O.R. with discontinuation of • can show pulse waveforms on suitably equipped
anesthetic drugs and extubation monitors
(exception - if going to intensive care unit (ICU)) • if ventilation is accidentally terminated, the SaO2 may
❏ patient can be transported to post-anesthesia care unit remain normal for several minutes
(PACU) when ABC's stable in a well oxygenated patient due to the high partial
❏ patient can be released from the unit when the PACU pressure of O2 remaining in the lungs
discharge criteria for ventilation, circulation, • inaccurate with hypotension, vasoconstriction, dyes,
consciousness, motor function, and colour have been met (e.g. nailpolish), other Hb, (e.g. CarboxyHb),
❏ potential complications compression of the limb, and movement
CNS • agitation, delirium, somnolence PO2 (mmHg) Hb Sat (%)
Respiratory • aspiration, upper airway obstruction 100 98
• hypoxemia, alveolar hypoventilation 80 96
• upper airway trauma (intubation/extubation) 60 90*
CVS • hypothermia (rewarm patient) 40 75
• shivering (due to hypothermia or postanesthetic effect) 27 50
• hypotension, hypertension, dysrhythmias * Recall Hb-O2 saturation curve (see Respirology
GI • nausea and vomiting Chapter)
I II III IV ❏ capnometer
MCCQE 2002 Review Notes Anesthesia – A13 • measures exhaled CO2, indicates adequacy of
ANESTHESIA . . . CONT. ventilation of lungs and cardiac output,
❏ pain control confirms ETT placement
• goal is to provide pain relief safely with minimal ❏ ECG
disturbance of homeostasis • changes in rate, rhythm, ST elevation/depression
(preoperative visit has been shown to be beneficial) ❏ BP cuff (manual/automatic)
• unrelieved pain can be the cause of many postoperative ❏ stethoscope (precordial, esophageal)
complications ❏ thermometer (surface or core)
• factors influencing the degree of pain include age, ❏ peripheral nerve stimulators (when using
personality, premedication, surgical site, neuromuscular blockade or blocking drugs)
and anesthetic technique • deliver electrical stimulus to elicit muscle responses
• routes - IV, IM, oral, epidural, rectal • indicates degree of muscle relaxation
• preemptive analgesia (controversial) ❏ machine function "monitors" - i.e. volume and
• prevent/reduce noxious stimuli which potentiate pressure alarms and inspired O2 alarms
peripheral and central pain mechanisms ❏ mass spectrometer/gas analyzer
• in postoperative period the dose of analgesic is • identifies and measures inhaled/exhaled gases
decreased and the side effects are less frequent A14 – Anesthesia MCCQE 2002 Review Notes
• use - NSAID's, opioids, local anesthetics, combined ANESTHESIA . . . CONT.
agents LESS FREQUENTLY USED MONITORS
• PCA (patient controlled analgesia) ❏ urinary catheter and urometer
• self-administration of small doses of opiates via pump ❏ central venous line
• bolus dose is preset • rapid fluid infusion, infusion of vasoactive drugs,
• lockout period is set to limit frequency of self- measuring CVP
administration ❏ arterial line
• requirements - oriented patient, IV, SC, or epidural • continuous BP monitoring, easy access allowing for
access frequent ABGs
MONITORING ❏ Swan-Ganz catheter- CVP, PCWP, pulmonary artery
• monitoring provides information that improves the pressures, cardiac output, mixed venous blood gases,
safety of anesthesia and provides a means to core temperature
assess physiological function ❏ ICP monitoring
• appropriate monitors with alarms are intended to ❏ EEG, brain and spinal cord evoked potentials
enhance but not replace the vigilance of ❏ transcutaneous gas measurements
the anesthetist ❏ transesophageal echocardiography (TEE)
• physical examination, observation, assessment, and GENERAL ANESTHETIC AGENTS
diagnosis remain the most important tools DEFINITION OF GENERAL ANESTHESIA (GA)
available to the anesthetist ❏ delivery of anesthetic drugs (inhaled or infused) to
• routine monitors for all cases: BP cuff, ECG, O2 sat produce a level
monitor, stethoscope, temperature probe, of CNS depression with the following goals (the 6 A's of
exposed part of patient visible, capnometer if intubated Anesthesia)
• organ systems monitored and other devices used to 1. ANESTHESIA - hypnosis, loss of consciousness
monitor will vary depending on the nature, 2. ANALGESIA - pain control
length, location, and systems involved in the surgery, and 3. AMNESIA - loss of recall
patient’s pre-existing condition/diseases 4. AREFLEXIA - muscle relaxation (this is not always
COMMONLY USED MONITORING DEVICES required)
❏ pulse oximeter 5. AUTONOMIC AREFLEXIA - decrease sympathetic
• measures SaO2 by red and infrared light absorption by nervous system (SNS) function
Hb; oxygenated and deoxygenated Hb 6. ANXIOLYSIS - pre-op and intra-op
have different absorption characteristics ❏ methods of GA are variable and complex
• non-invasive BALANCED ANESTHESIA
❏ a dynamic process incorporating a multiplicity of to thiopental
agents as no single anesthetic agent has ❏ less residual sedative effect, patient recovers sooner
been developed in which all theseproperties (the 6 A's) (T1/2 = 0.9 hr), thus popular for out patient surgery
are combined in optimal proportions since reduces post-anesthesia recovery time; decreased
PREMEDICATION incidence of nausea and vomiting
❏ medication may be given prior to anesthesia, i.e. ❏ more suited for continuous infusion than STP due to
benzodiazepines, opioids, glycopyrrolate rapid elimination
❏ goals ❏ more expensive
1. provide sedation, amnesia and relief from anxiety and Benzodiazepines (e.g. diazepam, midazolam,
pain lorazepam)
2. to prevent parasympathomimetic effects of the ❏ also known as the minor tranquilizers
anesthetics, i.e. to prevent salivation, ❏ used as a premedication prior to induction or as an
bronchial secretions and dysrhythmias caused by induction agent in combination with other drugs
anesthetic agents and airway instrumentation ❏ oral and injectable formulations available
IV ANESTHETICS (EXCLUDING OPIOIDS) ❏ act on specific brain (GABA) receptors to produce
❏ IV administration provides rapid distribution and selective anti-anxiety and sedative effects;
onset of effects in correct doses, causes only slight depression of CVS
❏ given as a bolus or as a continuous infusion, titrate to and respiratory systems
effect ❏ onset less than 5 minutes if given IV
❏ common agents used for induction are described ❏ duration of action long but variable/somewhat
below unpredictable
Thiopental (Sodium Thiopental, Sodium ❏ benzodiazepine antagonist flumazenil (Anexate)
Thiopentone, STP) • competitive inhibition
❏ ultrashort acting thiobarbiturate • does not affect benzodiazepine metabolism, therefore
❏ most commonly used as an induction agent once effects of reversal wear off,
❏ prepared as a pale yellow 2.5% solution with pH 10.5 sedation may return
(alkaline) Neuroleptics
❏ after IV bolus, rapidly distributes to vessel rich organs ❏ also known as the major tranquilizers, rarely used in
(brain, liver, heart, kidney), thus achieves anesthesia
unconsciousness in brain circulation time (approximately ❏ blockade of dopamine receptors at various locations in
30 seconds) CNS
❏ rapid redistribution from vessel rich tissues to muscle ❏ droperidol used in low dose as antiemetic
and fat causes short lived effect NARCOTICS/OPIOIDS
(approximately 5 minutes) ❏ opium: natural product derived from poppy plant
❏ metabolism and elimination occur at a slower rate extract
(T1/2 =5-12 hrs), resulting in residual effects ❏ opiates: derived from opium (e.g. morphine, codeine)
(usually sedation) during post-anesthesia recovery which ❏ opioids: any drug that binds to morphine receptors
may last hours (also known as opioid receptors);
❏ effects of thiopental include includes natural products, semisynthetic products,
• unconsciousness synthetic drugs, endogenous substances
• decreased cerebral metabolism and O2 requirements Opioid Receptors
• reduction of cerebral blood flow ❏ found in many locations in the body, particularly in
• decrease in CO, BP, reflex tachycardia the brain, brainstem, and spinal cord
• respiratory depression (apnea often occurs with bolus ❏ several classes of receptors, each responsible for
dose) different effects
❏ thiopental has no analgesic properties and at low • mu receptors: analgesia, respiratory depression,
doses actually increases the subjective feeling dependence
of pain (anti-analgesia) • kappa receptors: spinal analgesia, sedation
❏ no muscle relaxant properties • sigma receptors: hallucinations, dysphoria
❏ some contraindications • delta receptors: mood changes
• lack of equipment for intubation and resuscitation Indications
• potential difficult intubation ❏ opioids used for pre-, intra-, postoperative analgesia
• hypersensitivity ❏ also used as an induction agent, alone or as adjuvant
• untreated hypovolemia, hypotension, shock-like states ❏ reduces minimum alveolar concentration (MAC)
• cardiac failure required for volatile anesthetics
• porphyria ❏ can be administered IV, IM, PO
MCCQE 2002 Review Notes Anesthesia – A15 General Effects of Morphine (Prototype Opioid)
GENERAL ANESTHETIC AGENTS . . . CONT. ❏ CNS (depression) - analgesia, mood changes,
Propofol (Diprivan) sedation, respiratory depression, decreased cough reflex
❏ unique agent in its own class (an alkyl phenol) ❏ CNS (excitation) - miosis, nausea and vomiting,
❏ used for induction and/or maintenance of anesthesia hyperreflexia
❏ thick white soybean-based solution ❏ CVS - vasodilatation, orthostatic hypotension
❏ pharmacological effects similar to that of thiopental; ❏ Respiratory - central depression, bronchial
thus similar contraindications but is safe for constriction
porphyria patients ❏ GI - constipation, biliary colic
❏ metabolism and elimination much more rapid due to ❏ GU - urinary retention
increased rate of liver metabolism compared
❏ Other - histamine release, smooth muscle contraction anesthetic agents to respiratory system of patient via
(e.g. biliary and bladder sphincters) anesthetic machine
A16 – Anesthesia MCCQE 2002 Review Notes MAC • 0.75% 1.68% 1.15% • 104%1(weak anesthetic)
GENERAL ANESTHETIC AGENTS . . . CONT. Metabolism2 • 20% 2% 0.2% • 0%
Table 4. Other Opioids Used in Anesthesia Effects • CNS: increase cerebral blood flow, decrease
Agent Potency* Onset Duration Special cerebral O2 • Second gas effect3
Considerations consumption
Morphine 1 Moderate Moderate Histamine release • Resp: respiratory depression (decreased tidal volume
Codeine 1/6-1/10 Moderate Moderate Primarily (TV),
postoperative use, not for IV use increased rate), decreased response to respiratory
Meperidine 1/10 Moderate Moderate Anticholinergic, CO2 reflexes, bronchodilation
hallucination, • CVS: myocardial depression, vasodilatation
less pupillary constriction than morphine • MSK: muscle relaxation, potentiation of other muscle
Fentanyl 100 Rapid Short Transient muscle rigidity in relaxants, uterine relaxation
very high Uses • Maintenance of anesthetic state • Analgesia,
doses, good CVS stability allows for use of lower dose
Sufentanyl 1000 Rapid Short of more potent anesthetic
Alfentanyl 20 Rapid Very short MCCQE 2002 Review Notes Anesthesia – A17
*potency compared to morphine GENERAL ANESTHETIC AGENTS . . . CONT.
Opioid Antagonists (e.g. naloxone, naltrexone) Table 5. Volatile Inhalational Agents (continued)
❏ opioid toxicity manifests primarily at CNS - manage Halothane, Enflurane, Isoflurane, Sevoflurane
ABC's Nitrous Oxide (N2O)
❏ opioid antagonists competitively inhibit opioid Adverse Effects • Halothane rarely implicated in
receptors, predominantly mu receptors postoperative hepatitis • During emergence, N2O can
❏ must observe patient after administration diffuse
• naloxone relatively short acting (T1/2 = 1 hour); effects rapidly from the blood to the alveoli,
of narcotic may return when naloxone wears off resulting in a dilution of O2 in the
• naltrexone (T1/2 = 10 hours) - less likely to see return alveoli ("diffusion hypoxia") it is therefore
of narcotic effects unless narcotic levels very high necessary to provide 100% O2 for several
❏ relative overdose of naloxone may cause agitation, minutes until N2O is eliminated
sweating, tachycardia, hypertension, re-emergence of • Bone marrow depression
pain, • Chronic neuropathy
pulmonary edema, seizures • Toxicity mostly at CNS (decreased autonomic
VOLATILE INHALATIONAL AGENTS functions, hypotension, respiratory arrest) • Tends to
❏ exact mechanism of action unknown: currently diffuse into closed air spaces
thought to be due to anesthetic molecules embedding into causing increased pressure and volume
plasma membranes of cells, causing disruption of ion (important if there is trapped air
channels e.g. air embolus, pneumothorax,
❏ agents are delivered via respiratory system; partial blocked nasal sinuses, etc.)
pressure gradients cause diffusion of inhaled agents Contraindications • Lack of equipment/skill to
from alveoli to blood to brain (target organ) intubate/resuscitate, • Bowel obstruction
❏ for a given anesthetic gas at steady state illness requiring high inspired O2 • Any abdominal
alveolar partial pressure = arterial partial pressure = brain surgery where an increased
partial pressure • Hypersensitivity, malignant hyperthermia, volume of
❏ monitoring the end-tidal alveolar concentration of bowel gas would interfere
inhaled anesthetic agent provides a good estimate (see above) • Pneumothorax
of brain anesthetic tension and anesthetic depth • Airway obstruction, cardiac failure, severe CVS
❏ Minimum Alveolar Concentration (MAC) disease, • Pneumocephalus
• = % concentration of anesthetic agent in alveolar gas at raised ICP • Large alveolar bullae
steady state that will prevent movement in 1. A MAC of 104% is possible in a pressurized chamber
50% of subjects in response to a standard surgical only
stimulus eg. skin incision 2. Oxidative metabolism in liver, remainder is eliminated
• gas concentrations often expressed as multiples of via the respiratory system
MAC, 3. SECOND GAS EFFECT: Even though N2O is poorly
e.g. if an agent has a MAC of 1.5% then 0.5 MAC = soluble in blood, large amounts are taken up from the
0.75% and 2 MAC = 3.0% alveoli during
• MACs are additive, induction because it is administered in such large
e.g. 0.5 MAC of agent A plus 0.5 MAC of agent B will quantities (2-6 L/minute). As a result, the remaining
provide a gas mixture with a MAC of 1.0 gases (eg. isoflurane,
Table 5. Volatile Inhalational Agents enflurane) become more concentrated in the alveoli and
Halothane, Enflurane, Isoflurane, Sevoflurane therefore their uptake is enhanced
Nitrous Oxide (N2O) MUSCLE RELAXANTS + REVERSING DRUGS
Characteristics • Liquid, colorless, non-flammable non- ❏ mild muscle relaxation can be attained by increasing
explosive • Gas, colorless, mild sweet odor the depth
at room temperature of general anesthesia with potent inhalational agents but
• Vaporizer delivers controlled concentration of (stored the
as liquid under pressure)
amount required for useful muscle relaxation is too high twitch twitch
to be Post-tetanic facilitation of twitch height NO post-tetanic
practical, thus specific muscle relaxant drugs preferable facilitation of twitch height
❏ muscle relaxants cause variable degrees of Succinylcholine (SCh)
neuromuscular blockade (paralysis), ❏ SCh = physically resembles two ACh molecules
depending on dose joined end to end
❏ muscle relaxation often desired during surgical ❏ metabolism of SCh by plasma cholinesterase, 1/3,000
procedures for various reasons have atypical plasma cholinesterase
• prevent muscle stretch reflex and suppresses muscle (pseudocholinesterase) resulting in abnormally long
resting tone duration of paralysis
• facilitate intubation ❏ side effects of SCh
• facilitate controlled ventilation 1. SCh also binds to autonomic cholinergic receptors
• allow access to the surgical field (intracavitary surgery) • muscarinic receptors in heart can cause sinus
❏ muscle relaxants classified on the basis of the type of bradycardia
neuromuscular blockade they provide (especially in children or with repeat bolus in less than 10
• Depolarizing Neuromuscular Relaxants minutes)
• Non-depolarizing Neuromuscular Relaxants • muscarinic receptors in salivary glands resulting in
❏ and according to their duration of action increased secretions, especially in children
• short 2. hyperkalemia
• intermediate • potassium release due to persistent depolarization
• long • increase of 0.5 mEq/L with standard bolus
❏ both act at post-synaptic nicotinic acetylcholine • increase of 4.0 to 8.0 mEq/L in severe burns,
(ACh) receptor at the denervated muscles (plegias), major trauma, tetanus;
neuromuscular junction (NMJ) but use of SCh is generally safe in the first 24 hours
❏ actions potentiated by all potent inhalational agents 3. other side effects
❏ nerve stimulator used intraoperatively to assess block • increased ICP/intraocular pressure (IOP)/intragastric
level pressure
A18 – Anesthesia MCCQE 2002 Review Notes • triggers malignant hyperthermia
GENERAL ANESTHETIC AGENTS . . . CONT. • sustained contraction in myotonia
Table 6. Muscle Relaxants • fasciculations
Non-depolarizing (Competitive) Depolarizing (Non- ❏ defasciculation: a small dose of non-depolarizing
competitive) agent given before SCh may reduce some side effects
Agents d-Tubocurarine, pancuronium, Succinylcholine (fasciculations, increased ICP, IOP, myalgia); however,
doxacurium, atracurium, vecuronium, SCh efficacy is decreased, thus SCh has to be given
mivacurium, rocuronium in a 30-50% higher dose
Action at ACh Competitively bind at NMJ without MCCQE 2002 Review Notes Anesthesia – A19
Binds receptor with depolarization GENERAL ANESTHETIC AGENTS . . . CONT.
Receptor causing depolarization causing fasciculations; ❏ contraindications to SCh use
sustained • upper and lower motor neuron lesions (UMN/LMN),
receptor availability to ACh burns, etc.
depolarization prevents action • allergy, hypersensitivity
potential from propagating at junction • malignant hyperthermia
causing temporary paralysis • lack of necessary skill or equipment to intubate
Onset Slower (2-4 minutes) Rapid (30-60 seconds) • suspected difficult intubation (e.g. facial/neck trauma,
Duration Intermediate to long (20-60 minutes) Short (5 unstable cervical spine, etc.)
minutes) • hyperkalemia
Use Muscle relaxation for intubation or Muscle • myotonia congenita, muscular dystrophy
relaxation for intubation • decreased levels/atypical plasma cholinesterase
intraoperatively, facilitation of short procedures, ECT to (pseudocholinesterase)
eliminate muscular • open eye injury
mechanical ventilation in some ICU component of Reversing Agents for Non-depolarizing Blockade (e.g.
convulsions Neostigmine, Pyridostigmine)
patients, reduction of fasciculations ❏ reversible anticholinesterases
and post-op myalgias secondary to SCh ❏ inhibit enzymatic degradation of ACh; increases ACh
Reversibility Yes, with anticholinesterase No at nicotinic receptors, displacing the
pharmacological non-depolarizing muscle relaxant
agents such as Neostigmine reversal available ❏ if non-depolarizing blockade is COMPLETE,
Response to Lower than normal twitch height Lower increasing amount of ACh has little effect; therefore
than normal twitch height anticholinesterase has little effect and should not be
Peripheral Nerve administered until the block is PARTIAL
Stimulation with Gradual fade of twitch height with NO ❏ blockade assessed with nerve stimulator before
fade of twitch height with administration of reversal
Partial Block single twitch stimulus applied as a single (no twitch response = 100% blockade)
twitch stimulus applied as a ❏ with reversal, ACh concentration will increase at
train of four (TOF) and with tetanus train of four (TOF) muscarinic (before nicotinic)
or with tetanus sites causing bradycardia, salivation etc.
normal single TOF tetanus normal single TOF tetanus
❏ therefore simultaneous administration of atropine or B sympathetic blockade
glycopyrrolate is necessary to decrease A-delta and C pain
cholinergic side effects by causing muscarinic receptor A-beta and A-gamma touch
blockade A-alpha motor, proprioception and vibration
REGIONAL ANESTHESIA ❏ since sympathetic blockade (with hypotension,
DEFINITION OF REGIONAL ANESTHESIA bradycardia) occurs early, it is a
❏ local anesthetic applied around a peripheral nerve at potentially dangerous side effect of spinal/epidural
any point along the length of the nerve anesthesia
(from spinal cord up to, but not including, the nerve ❏ titration of LA dosage for differential blockade, e.g.
endings) for the purposes of reducing or can block pain but preserve motor function
preventing impulse transmission EPIDURAL AND SPINAL ANESTHESIA
❏ no CNS depression (unless overdose (OD) of local Anatomy of Spinal/Epidural Area
anesthetic); patient conscious ❏ spinal cord extends to L2, dural sac to S2
❏ regional anesthetic techniques categorized as follows ❏ nerve roots (cauda equina) from L2 to S2
• epidural and spinal anesthesia ❏ needle inserted below L2 should not encounter cord,
• peripheral nerve blockades thus L3-L4, L4-L5 interspace commonly used
• IV regional anesthesia ❏ structures penetrated
PREPARATION FOR REGIONAL ANESTHESIA • skin, subcutaneous fat
Patient Preparation • supraspinous ligament
❏ thorough pre-op evaluation and assessment of patient • interspinous ligament
❏ technique explained to patient • ligamentum flavum (last layer before epidural space)
❏ IV sedation may be indicated before block • dura + arachnoid for spinal anesthesia
❏ monitoring should be as extensive as for general Spinal Anesthesia
anesthesia ❏ relatively small LA dose injected into subarachnoid
Nerve Localization space in the dural sac surrounding the
❏ anatomical landmarks, local anatomy, e.g. line joining spinal cord + nerve roots
iliac crests crosses L3-L4 interspace; ❏ LA solution may be made hyperbaric (of greater
axillary artery as guide to brachial plexus specific gravity (SG) than the cerebrospinal fluid (CSF)
❏ paresthesias and peripheral nerve stimulation used as by mixing with 10% dextrose, thus increasing spread of
a guide to proper needle placement LA to the dependent (low) areas
Relative Indications for Regional Anesthesia of the subarachnoid space
❏ avoidance of some of the dangers of general Epidural Anesthesia
anesthesia (e.g. known difficult intubation, ❏ LA deposited in epidural space (potential space
severe respiratory failure, etc.) between ligamentum flavum and dura)
❏ patient specifically requests regional anesthesia ❏ solutions injected here spread in all directions of the
❏ for high quality post-op pain relief potential space; SG of solution does not affect spread
❏ general anesthesia not available ❏ initial blockade is at the spinal roots followed by some
Contraindications to Regional Anesthesia degree of spinal cord anesthesia as LA diffuses
❏ allergy to local anesthetic into the subarachnoid space through the dura
❏ patient refusal, lack of cooperation ❏ larger dose of LA used
❏ lack of resuscitation equipment Spinal vs. Epidural Anesthesia
❏ lack of IV access ❏ spinal
❏ coagulopathy • easier to perform
❏ certain types of preexisting neurological dysfunction • smaller dose of LA required (usually < toxic IV dose)
❏ local infection at block site • rapid blockade (onset in 2-5 minutes)
Complications of Regional Anesthesia • very effective blockade
❏ failure of technique • hyperbaric LA solution - position of patient important
❏ systemic drug toxicity due to overdose or ❏ epidural
intravascular injection • technically more difficult; greater failure rate
❏ peripheral neuropathy due to intraneural injection • larger volume/doses of LA (usually > toxic IV dose)
❏ pain or hematoma at injection site • significant blockade requires 10-15 minutes
❏ infection • effectiveness of blockade can be variable
A20 – Anesthesia MCCQE 2002 Review Notes • use of catheter allows for continuous infusion or repeat
REGIONAL ANESTHESIA . . . CONT. injections
NERVE FIBRES • slower onset of side effects
❏ different types categorized as follows • position of patient not as important
1. MYELINATED A FIBERS (largest to smallest) • SG of LA solution not as important
• alpha: motor function, proprioception Complications of Spinal/Epidural Anesthesia
• beta: pressure and touch, some motor function ❏ spinal anesthesia
• gamma: muscle spindle tone • failure of technique
• delta: pain and temperature • hypotension, bradycardia if block reaches T2-4
2. THIN MYELINATED B FIBERS (sympathetic nervous system (SNS) block)
• preganglionic axons • post-spinal headache
3. UNMYELINATED C FIBERS • extensive spread of anesthetic ("high spinal")
• pain and temperature • persistent paresthesias (usually transient)
❏ order of blockade with local anesthetic (LA): • epidural or subarachnoid hematoma
FIBRES FUNCTION • spinal cord trauma, infection
MCCQE 2002 Review Notes Anesthesia – A21 ❏ adequate anesthesia of obstetric patients requires a
REGIONAL ANESTHESIA . . . CONT. clear understanding of maternal and fetal physiology
❏ epidural anesthesia ❏ options for pain relief during parturition (labour) are
• failure of technique 1) psychoprophylaxis – Lamaze method
• hypotension - common • patterns of breathing and focused attention of fixed
• bradycardia if cardiac sympathetics blocked (only if object
~T2-4 block) 2) systemic medication
• systemic toxicity of LA (accidental intravenous) • easy to administer but risk of maternal or neonatal
• accidental subarachnoid injection can lead to total depression
spinal anesthesia • common drugs: opioids, tranquilizers, ketamine
• catheter complications (shearing, kinking, vascular or 3) regional anesthesia
subarachnoid placement) • provides excellent analgesia with minimal depressant
• epidural or subarachnoid hematoma effects in mother and fetus
Contraindications to Spinal/Epidural Anesthesia • hypotension as a consequence of sympathectomy is the
❏ absolute contraindications include lack of proper most common complication
equipment or properly trained personnel, patient refusal, • maternal BP monitored q2-5 min for 15-20 min after
lack of IV access, allergy to LA, infection at puncture initiation and regularly thereafter
site or underlying tissues, uncorrected hypovolemia, • techniques used: epidural, combined spinal epidural,
coagulation abnormalities, raised ICP pudendal blocks, spinal,
❏ relative contraindications include bacteremia, paracervical, lumbar sympathetic blocks
preexisting neurological disease, aortic/mitral valve 4) inhalational analgesia
stenosis, • easy to administer, makes uterine contractions more
previous spinal surgery, other back problems, tolerable, but does not relieve pain completely
severe/unstable psychiatric disease or emotional • 50% nitrous oxide
instability ❏ anesthesia for cesarean section
IV REGIONAL ANESTHESIA 1. Regional - spinal or epidural
❏ provides very good anesthesia and muscle relaxation 2. General - used when contraindications to regional or
for operations up to 1.5 hours on the time precludes regional blockade
upper/lower extremity (UE/LE) ❏ potential complications
❏ more commonly used for upper extremity • pulmonary aspiration – due to increased
❏ primary blockade at nerve trunks gastroesophageal reflux
❏ significant secondary blockade at sensory nerve • hypotension and/or fetal distress - caused by occlusion
endings and NMJ of the inferior vena cava (IVC)/aorta by the
❏ risk of systemic LA toxicity (i.e. tourniquet failure) gravid uterus (aortocaval compression) therefore
❏ advantages corrected by turning patient in the left lateral
• reliable decubitus (LLD) position
• relatively simple technique • unintentional total spinal anesthesia
• very few absolute contraindications • LA induced seizures – as a result of intravascularization
❏ contraindications of LA
• patient refusal • postdural puncture headache
• allergy or hypersensitivity to LA • nerve injury - rare
• thrombophlebitis A22 – Anesthesia MCCQE 2002 Review Notes
• conditions where a tourniquet cannot be used (e.g. LOCAL INFILTRATION, HEMATOMA BLOCKS
sickle cell disease) Local Infiltration
❏ technique involves ❏ injection of tissue with LA, producing a lack of
1. cannulation of peripheral vein sensation in the infiltrated area due to LA acting on
2. exsanguination of limb by elevation and bandage nerve endings
application ❏ one of the simplest and safest techniques of providing
3. arterial tourniquet inflated to a pressure of 100 mm Hg anesthesia
above patient’s systolic pressure ❏ suitable for small incisions, suturing, excising small
4. inject low concentration lidocaine (e.g. 0.5%) without lesions
epinephrine via cannula ❏ can use fairly large volumes of dilute LA to infiltrate
Note: pain at site of tourniquet can be avoided by using a a large area (see maximum dose below)
double tourniquet - anesthesia is induced with ❏ low concentrations of epinephrine ( 1:100,000-
proximal tourniquet inflated, then distal cuff inflated and 1:200,000) cause vasoconstriction thus reducing bleeding
proximal cuff deflated and prolonging the effects of LA by reducing systemic
PERIPHERAL NERVE BLOCKS absorption
❏ e.g. brachial plexus block, ankle block, digital ring (contraindicated in fingers, nose, penis, toes and ears)
block Fracture Hematoma Block
❏ relatively safe – avoid intraneural injection and ❏ special type of local infiltration for pain control in the
neurotoxic agents manipulation of certain fractures
❏ provides good operating conditions ❏ hematoma created by fracture is infiltrated with LA to
OBSTETRICAL ANESTHESIA (see Obstetrics anesthetize surrounding tissues
Chapter) ❏ sensory blockade may be only partial
❏ all patients entering the delivery room potentially ❏ no muscle relaxation
require anesthesia, whether planned or as an emergency LOCAL ANESTHETICS (LA)
❏ Local Anesthetics (e.g. lidocaine, bupivicaine, • tinnitus
mepivacaine, chlorprocaine and • visual disturbances
"TAC" - mixture of tetracaine, adrenaline and cocaine) • muscle twitching, tremors
Definition and Mode of Action • convulsions, seizures
❏ LA are drugs that block the generation and • generalized CNS depression, coma, respiratory arrest
propagation of impulses in excitable tissues: nerves, MCCQE 2002 Review Notes Anesthesia – A23
skeletal muscle, cardiac muscle, brain LOCAL ANESTHETICS (LA) . . . CONT.
❏ LA substances bind to a Na+ channel receptor on the ❏ CVS effects
cytosolic side of the Na+ channel • vasodilatation, hypotension
(i.e. must be lipid soluble), inhibiting Na+ flux and thus • decreased myocardial contractility
blocking impulse conduction • dose-dependent delay in cardiac impulse transmission
❏ LA must convert to an ionized form to properly bind • prolonged PR, QRS intervals
to receptor • sinus bradycardia
❏ different types of nerve fibres undergo blockade at • CVS collapse
different rates (see Regional Anesthesia section) ❏ treatment of systemic toxicity
Absorption, Distribution, Metabolism • early recognition of signs
❏ LA readily crosses the blood-brain barrier (BBB) once • 100% O2, manage ABCs
absorbed into the blood stream • diazepam may be used to increase seizure threshold
❏ ester-type LA (procaine, tetracaine) broken down by • if the seizures are not controlled by diazepam, consider
plasma and hepatic esterases; using:
metabolites excreted via kidneys • thiopental (increases seizure threshold)
❏ amide-type LA (lidocaine, bupivicaine) broken down • SCh (stops muscular manifestations of seizures,
by hepatic mixed function oxidases (P450 system); facilitates intubation)
metabolites excreted via kidney SPECIAL CONSIDERATIONS
Selection of LA ATYPICAL PLASMA CHOLINESTERASE
❏ delivery modalities include epidural, spinal, peripheral ❏ plasma cholinesterase also known as
nerve blockades, local injections, topical Pseudocholinesterase
❏ choice of LA depends on ❏ plasma cholinesterase variants decrease SCh
• onset of action –influenced by pKa (lower the pKa, the hydrolysis (metabolism) and thus prolong muscle
higher the concentration of paralysis
the base form of the LA and the faster the onset of ❏ suspect if patient has personal or family history of
action) anesthetic related complications
• duration of desired effects – influenced by protein ❏ treatment
binding • ABCs
(long duration of action when the protein binding of LA • ventilate till normal muscle strength returns as no SCh
is strong) direct antagonist exists
• potency – influenced by lipid solubility (agents with ENDOCRINE DISORDERS
high lipid solubility will penetrate ❏ adrenocortical insufficiency
the nerve membrane more easily) • Addison's, exogenous steroids
• unique needs (e.g. sensory blockade with relative • treatment with steroids pre-, peri-, post-op
preservation of motor function, ❏ diabetes mellitus (DM)
for pain management) • hypo/hyperglycemia due to drugs + stress
• potential for toxicity • hypoglycemia masked by anesthesia
Maximum Doses for LA • treatment: dextrose/insulin, monitor blood glucose
❏ always be aware of the maximum dose for the ❏ pheochromocytoma
particular LA used • adrenergic crisis with surgical manipulation
❏ maximum dose usually expressed as (mg of LA) per • prevention with alpha + beta adrenergic blockade pre-
(kg of lean body weight) op
and as a total maximal dose (adjusted for ❏ "thyroid storm" (rare)
young/elderly/ill) • especially labour/delivery, anesthesia
❏ lidocaine maximum dose: 5 mg/kg (with epinephrine: treatment: beta blockers + pre-op prophylaxis
7mg/kg) MALIGNANT HYPERTHERMIA (MH)
❏ chlorprocaine maximum dose: 11 mg/kg (with ❏ hypermetabolic disorder of skeletal muscle
epinephrine: 14 mg/kg) ❏ autosomal dominant (AD) pattern of genetic
❏ bupivicaine maximum dose: 2.5 mg/kg (with inheritance (possibly)
epinephrine: 3 mg/kg) ❏ incidence of 1-5:100,000, may be associated with
Systemic Toxicity skeletal muscle abnormalities such as ptosis,
❏ occurs by accidental intravascular injection, LA hernia, scoliosis
overdose, or unexpectedly rapid absorption ❏ intracellular hyperCa2+ (due to altered Ca2+
❏ systemic toxicity manifests itself mainly at CNS and sequestration) with resultant hypercatabolism
CVS and decreased ATP
❏ CNS effects first appear to be excitatory due to initial ❏ anesthetic drugs triggering MH crises include
block of inhibitory fibres; • volatile anesthetics: enflurane, halothane, isoflurane
subsequently, block of excitatory fibres and sevoflurane (any drug ending in “ane”)
❏ CNS effects (in approximate order of appearance) • depolarizing relaxants SCh, decamethonium
• numbness of tongue, perioral tingling Signs and Symptoms
• disorientation, drowsiness ❏ immediate or hours after contact with trigger agent
❏ increased end-tidal endotracheal CO2 monitoring on (e.g. volume changes, decreased diffusion, hyperactive
capnograph airways, laryngeal spasm, obesity,
❏ tachycardia/dysrhythmia altered compliance, secretions, etc.)
❏ tachypnea/cyanosis ❏ anticipate + optimize pre-operatively to prevent intra-
❏ increased temperature - may be delayed op and post-op problems
❏ hypertension ASPIRATION SYNDROME
❏ diaphoresis ❏ severity of gastric aspiration related to volume of the
❏ trismus (masseter spasm) common but not specific for aspirate, quality of aspirate
MH (i.e. acidity and presence of contaminated particles) and
(occurs in 1% of children given SCh with halothane the health status of the patient
anesthesia) ❏ avoid inhibiting airway reflexes, reduce gastric
Lab volume and acidity, employ rapid sequence induction
❏ hyper CO2, hypoxia (early) PH
❏ metabolic acidosis BENIGNA PROSTAT HIPERPLASIA (BPH)
❏ respiratory acidosis I. PENGERTIAN
❏ hyperkalemia Istilah hipertrofi sebenarnya kurang tepat karena yang
❏ myoglobinemia/myoglobinuria terjadi adalah hiperplasia kelenjar
❏ increased creatine kinase (CK) periuretra yang mendesak jaringan prostat yang asli ke
A24 – Anesthesia MCCQE 2002 Review Notes perifer dan menjadi kapsul bedah.
SPECIAL CONSIDERATIONS . . . CONT. (Anonim FK UI 1995).
Complications Prostat adalah jaringan fibromuskuler dan jaringan
❏ death/coma kelenjar yang terlihat persis di inferior dari
❏ disseminated intravascular coagulation (DIC) kandung kencing. Prostat normal beratnya + 20 gr,
❏ muscle necrosis/weakness didalamnya berjalan uretra posterior + 2,5
❏ myoglobinuric renal failure cm.
❏ electrolyte abnormalities (i.e. iatrogenic hypokalemia) Pada bagian anterior difiksasi oleh ligamentum
Prevention puboprostatikum dan sebelah inferior oleh
❏ suspect possible MH in patients presenting with a diafragma urogenitale. Pada prostat bagian posterior
family history of problems/death with anesthetic bermuara duktus ejakulatoris yang
❏ dantrolene prophylaxis no longer routine berjalan miring dan berakhir pada verumontanum pada
❏ avoid all triggers dasar uretra prostatika tepat proksimal
❏ central body temp and ET CO2 monitoring dari spingter uretra eksterna.
❏ use regional anesthesia if possible II. PATOFISIOLOGI
❏ use equipment “clean” of trigger agents Proses pembesaran prostat terjadi secara perlahan-lahan
Management sehingga perubahan pada saluran
❏ discontinue inhaled anesthetic and SCh, terminate 1 / 19
procedure BPH
❏ hyperventilate with 100% O2 kemih juga terjadi secara perlahan-lahan. Pada tahap
❏ Dantrolene 1 mg/kg, repeating until stable or 10 awal setelah terjadinya pembesaran
mg/kg maximum reached prostat, resistensi pada leher buli-buli dan daerah prostat
(Dantrolene interferes with calcium release into meningkat, serta otot destrusor
myoplasm from sarcoplasmic reticulum) menebal dan merenggang sehingga timbul sakulasi atau
❏ treat metabolic/physiologic derangements accordingly divertikel. Fase penebalan destrusor
❏ control body temperature ini disebut fase kompensasi. Apabila keadaan berlanjut,
❏ diligent monitoring (especially CVS, lytes, ABGs, maka destrusor menjadi lelah dan
urine output) akhirnya mengalami dekompensasi dan tidak mampu lagi
MYOCARDIAL INFARCTION (MI) untuk berkontraksi sehingga terjadi
❏ ELECTIVE surgery should not be carried out within 6 retensio urin yang selanjutnya dapat menyebabkan
months of an MI: hidronefrosis dan disfungsi saluran kemih
this period carries increased risk of reinfarction/death atas.
❏ classic reinfarction risk is quoted as: III. ETIOLOGI
• < 3 months after MI - 37% patients may reinfarct Penyebab secara pasti belum diketahui, namun terdapat
• 3-6 months after MI - 15% faktor resiko umur dan hormon
• > 6 months after MI - risk remains constant at 5% androgen (Anonim,FK UI,1995). Pada umur diatas 50
• reinfarction carries a 50% mortality rate tahun, pada orang laki-laki akan timbul
❏ if operative procedure is essential and cannot be mikronodule dari kelenjar prostatnya.
delayed, 1V. GAMBARAN KLINIS
the risk may be lessened by invasive monitoring + post- Gejala-gejala pembesaran prostat jinak dikenal sebagai
op ICU Lower Urinary Tract Symptoms
monitoring to 6%, 3% and 1% respectively for the above (LUTS),yang dibedakan menjadi:
time periods 1. Gejala iritatif, yaitu sering miksi (frekuensi),
❏ mortality wth perioperative MI is 20-50% terbangun pada malam hari untuk miksi
❏ infarct rate in absence of prior MI is 0.13% ( nokturia),perasaan ingin miksi yang sangat mendesak
RESPIRATORY DISEASES (urgensi),dan nyeri pada saat
❏ ventilation and delivery of volatile anesthetics can be miksi ( disuria).
complicated by pulmonary disease states 2. Gejala obstruktif adalah pancaran melemah, rasa tidak
puas setelah miksi, kalau
mau miksi harus menunggu lama , harus insiden syok lebih rendah, serta ideal bagi pasien dengan
mengedan,kencing terputus-putus,dan waktu prostat yang besar, resiko bedah
miksi memanjang yang akhirnya menjadi retensi urin dan buruk bagi pasien sangat tua dan ringkih. Pada pasca
inkontinen karena operasi luka bedah mudah
overflow. terkontaminasi karena insisi dilakukan dekat dengan
(Anonim,FK UI,1995). rektal. Lebih jauh lagi inkontinensia,
2 / 19 impotensi, atau cedera rectal dapat mungkin terjadi dari
BPH cara ini. Kerugian lain adalah
V.PEMERIKSAAN PENUNJANG kemungkinan kerusakan pada rectum dan spingter
1.Pemeriksaan colok dubur eksternal serta bidang operatif terbatas.
Pemeriksaan colok dubur dapat memberikan kesan c. Prostatektomi retropubik.
keadaan tonus sfingter anus, mukosa Adalah suatu teknik yang lebih umum dibanding
rektum, kelainan lain seperti benjolan dalam rektum dan pendekatan suprapubik dimana insisi
prostat. Pada perabaan melalui colok abdomen lebih rendah mendekati kelenjar prostat, yaitu
dubur dapat diperhatikan konsistensi prostat, adakah antara arkus pubis dan kandung kemih
asimetri, adakah nodul pada prostat, tanpa tanpa memasuki kandung kemih. Prosedur ini
apakah batas atas dapat diraba. Derajat berat obstruksi cocok untuk kelenjar besar yang terletak
dapat diukur dengan menentukan tinggi dalam pubis. Meskipun darah yang keluar dapat
jumlah sisa urine setelah miksi spontan. Sisa miksi dikontrol dengan baik dan letak bedah
ditentukan engan mengukur urine yang labih mudah untuk dilihat, infeksi dapat cepat terjadi
masih dapat keluar dengan kateterisasi. Sisa urine dapat dalam ruang retropubis. Kelemahan
pula diketahui dengan melakukan lainnya adalah tidak dapat mengobati penyakit kandung
ultrasonografi kandung kemih setelah miksi. kemih yang berkaitan serta insiden
2.Pemeriksaan laboratorium hemorargi akibat pleksus venosa
a.Analisis urin dan pemeriksaan mikroskopik urin, prostat meningkat juga osteitis pubis. Keuntungan yang
elektrolit, kadar ureum kreatinin. lain adalah periode pemulihan lebih
b.Bila perlu Prostate Spesific Antigen (PSA), untuk dasar singkat serta kerusakan spingter kandung kemih lebih
penentuan biopsi. sedikit.
3.Pemeriksaan radiologi : 2. Insisi Prostat Transuretral ( TUIP ).
a.Foto polos abdomen Yaitu suatu prosedur menangani BPH dengan cara
b.BNO-IVP memasukkan instrumen melalui
3 / 19 uretra. Satu atau dua buah insisi dibuat pada prostat dan
BPH kapsul prostat untuk mengurangi
c.Systocopy tekanan prostat pada uretra dan mengurangi kontriksi
d.Cystografi uretra. Cara ini diindikasikan ketika
4.USG kelenjar prostat berukuran kecil ( 30 gram/kurang ) dan
VI. PENATALAKSANAAN efektif dalam mengobati banyak kasus
1. Terapi medikamentosa BPH. Cara ini dapat dilakukan di klinik rawat jalan dan
2. Terapi bedah : Waktu penanganan untuk tiap pasien mempunyai angka komplikasi lebih
bervariasi tergantung beratnya gejala rendah di banding cara lainnya.
dan komplikasi. Indikasi terapi bedah yaitu : 3. TURP ( TransUretral Reseksi Prostat )
a. Retensio urin berulang TURP adalah suatu operasi pengangkatan jaringan
b. Hematuria prostat lewat uretra menggunakan
c. Tanda penurunan fungsi ginjal resektroskop.
d. Infeksi saluran kencing berulang TURP merupakan operasi tertutup tanpa insisi serta tidak
e. Tanda-tanda obstruksi berat yaitu mempunyai efek merugikan
divertikel,hidroureter, dan hidronefrosis. 6 / 19
4 / 19 BPH
BPH terhadap potensi kesembuhan. Operasi ini dilakukan pada
f. Ada batu saluran kemih. prostat yang mengalami
Macam-macam tindakan pada klien BPH : pembesaran antara 30-60 gram, kemudian dilakukan
1. PROSTATEKTOMI reseksi. Cairan irigasi digunakan secara
a. Prostatektomi Supra pubis. terus-menerus dengan cairan isotonis selama prosedur.
Adalah salah satu metode mengangkat kelenjar melalui Setelah dilakukan reseksi,
insisi abdomen. Yaitu suatu insisi yang penyembuhan terjadi dengan granulasi dan reepitelisasi
dibuat kedalam kandung kemih dan kelenjar prostat uretra pars prostatika (Anonim,FK
diangkat dari atas. UI,1995).
b. Prostatektomi Perineal. Setelah dilakukan TURP, dipasang kateter Foley tiga
Adalah mengangkat kelenjar melalui suatu insisi dalam saluran no. 24 yang dilengkapi
perineum. Cara ini lebih praktis balon 30 ml, untuk memperlancar pembuangan gumpalan
dibanding cara yang lain, dan sangat berguna untuk darah dari kandung kemih. Irigasi
biopsi terbuka. Keuntungan yang lain kanding kemih yang konstan dilakukan setelah 24 jam
memberikan pendekatan anatomis langsung, drainage bila tidak keluar bekuan darah lagi.
oleh bantuan gravitasi, efektif untuk Kemudian kateter dibilas tiap 4 jam sampai cairan jernih.
terapi kanker radikal, hemostatik di bawah penglihatan Kateter dingkat setelah 3-5 hari
langsung,angka mortalitas rendah, setelah operasi dan pasien harus sudah dapat berkemih
dengan lancar.
TURP masih merupakan standar emas. Indikasi TURP - Gunakan teknik komunikasi terapeutik untuk
ialah gejala-gejala dari sedang mengetahui - Berikan lingkungan yang tenang
sampai berat, volume prostat kurang dari 60 gram dan - Kurangi faktor presipitasi nyeri.
pasien cukup sehat untuk menjalani - Ajarkan teknik non farmakologis (relaksasi, distraksi
operasi. Komplikasi TURP jangka pendek adalah dll) -Kolaborasi pemberian analgetik untuk mengurangi
perdarahan, infeksi, hiponatremia atau nyeri.
retensio oleh karena bekuan darah. Sedangkan - Evaluasi tindakan pengurang nyeri/kontrol nyeri.
komplikasi jangka panjang adalah striktura Kolaborasi dengan dokter bila ada komplain tentang
uretra, ejakulasi retrograd (50-90%), impotensi (4-40%). pemberian analgetik tidak berhasil.
Karena pembedahan tidak mengobati - Monitor penerimaan klien tentang manajemen nyeri.
penyebab BPH, maka biasanya penyakit ini akan timbul 10 / 19
kembali 8-10 tahun kemudian. BPH
VII. KOMPLIKASI Administrasi analgetik : .
1. Perdarahan. - Cek program pemberian analogetik; jenis, dosis, dan
2. Pembentukan bekuan frekuensi.
3. Obstruksi kateter - Cek riwayat alergi.
4. Disfungsi seksual tergantung dari jenis pembedahan. - Tentukan analgetik pilihan, rute pemberian dan dosis
7 / 19 optimal.
BPH - Monitor V/S
5. Komplikasi yang lain yaitu perubahan anatomis pada - Berikan analgetik tepat waktu terutama saat nyeri
uretra posterior menyebabkan ejakulasi muncul.
retrogard yaitu setelah ejakulasi cairan seminal mengalir - Evaluasi efektifitas analgetik, tanda dan gejala efek
kedalam kandung kemih dan samping.
diekskresikan bersama urin. Selain itu vasektomi 2
mungkin dilakukan untuk mencegah Resiko infeksi b/d pertahanan tubuh primer yang tidak
penyebaran infeksi dari uretra prostatik melalui vas adekuat, prosedur invasif, luka pembedahan.
deference dan ke dalam epidedemis. 11 / 19
Setelah prostatektomi total ( biasanya untuk kanker ) BPH
hampir selalu terjadi impotensi. Bagi - Bebas dari tanda dan gejala infeksi
pasien yang tak mau kehilangan aktifitas seksualnya, - Angka lekosit normal (4-11.000)
implant prostetik penis mungkin - V/S dbn
digunakan untuk membuat penis menjadi kaku guna Kontrol infeksi :
keperluan hubungan seksual. - Bersihkan lingkungan setelah dipakai pasien lain.
6. Infeksi - Batasi pengunjung bila perlu.
VIII. DIAGNOSA KEPERAWATAN YANG - Anjurkan keluarga untuk cuci tangan sebelum dan
MUNGKIN MUNCUL setelah - Gunakan sabun anti microba untuk mencuci
1.Nyeri akut berhubungan dengan Agen injuri fisik, tangan.
pembedahan - Lakukan cuci tangan sebelum dan sesudah tindakan
2. Resiko infeksi berhubungan dengan pertahanan primer keperawatan.
yang tidak adekuat, prosedur invasif. - Gunakan baju, masker dan sarung tangan sebagai alat
3. Kurang pengetahuan tentang penyakit, perawatan dan 12 / 19
pengobatannya berhubungan dengan BPH
kurang familier terhadap informasi, kognitif. - Pertahankan lingkungan yang aseptik selama
4. Syndrom defisit self care berhubungan dengan pemasangan - Lakukan perawatan luka dan dresing
kelemahan, penyakitnya infus,DC sesuai - Tingkatkan intake nutrisi dan cairan
5. Potential Komplikasi ( PK ) : Perdarahan yang adekuat
8 / 19 - Berikan antibiotik sesuai program.
BPH Proteksi terhadap infeksi
RENPRA BPH - Monitor tanda dan gejala infeksi sistemik dan lokal.
No - Monitor hitung granulosit dan WBC.
Diagnosa - Monitor kerentanan terhadap infeksi.
Tujuan 13 / 19
Intervensi BPH
1 Pertahankan teknik aseptik untuk setiap tindakan.
Nyeri Akut berhubungan dengan Agen injuri fisik - Inspeksi kulit dan mebran mukosa terhadap kemerahan,
(pembedahan) Inspeksi keadaan luka dan sekitarnya
meningkat, nyeri terkontrol dengan KH: Ambil kultur jika perlu
- Klien melaporkan nyeri berkurang, skala nyeri 2-3 - Dorong klien untuk intake nutrisi dan cairan yang
- Ekspresi wajah tenang & dapat istirahat, tidur. adekuat.
9 / 19 - Anjurkan istirahat yang cukup
BPH - Ajari dan ajarkan klien untuk meningkatkan mobilitas
- v/s dbn (TD 120/80 mmHg, N: 60-100 x/mnt, RR: 16- dan - Instruksikan klien untuk minum antibiotik sesuai
20x/mnt). program.
Manajemen nyeri : - Ajarkan keluarga/klien tentang tanda dan gejala infeksi.
- Kaji nyeri secara komprehensif termasuk lokasi, - Laporkan kecurigaan infeksi.
karakteristik, - Observasi reaksi nonverbal dari ketidak 3
nyamanan. 14 / 19
BPH
Kurang pengetahuan ttng penyakit, perawata,pengobatan
Nya d/g kurang familier terhadap informasi, terbatasnya
kognitif.
Setelah dilakukan
- Klien/klg mampu menjelaskan kembali apa yang
dijelaskan
- Klien /klg kooperative saat dilakukan tindakan
Teaching : Dissease Process
- Kaji tingkat pengetahuan klien dan keluarga tentang
proses - Jelaskan tentang patofisiologi penyakit, tanda
dan gejala - Sediakan informasi tentang kondisi klien
- Berikan informasi tentang perkembangan klien
- Diskusikan perubahan gaya hidup yang mungkin
diperlukan - Diskusikan tentang pilihan tentang terapi
atau pengobatan
- Jelaskan alasan dilaksanakannya tindakan atau terapi
- Dorong klien untuk menggali pilihan-pilihan atau
memperoleh - Jelaskan kemungkinan komplikasi yang
mungkin terjadi
- Anjurkan klien untuk mencegah efek samping dari
penyakit
- Gali sumber-sumber atau dukungan yang ada
- Anjurkan klien untuk melaporkan tanda dan gejala yang
4
Sindrom defisit self care b/d kelemahan dan nyeri,
penyakitnya
Setelah dilakukanm aasmuhpaun P keerpaewraawtaanta
dni r…i . jam klien
Dg KH:
- Pasien dapat melakukan aktivitas sehari-hari (makan,
berpakaian, kebersihan, toileting, - Kebersihan diri
pasien terpenuhi
Bantuan perawatan diri makan, kebersihan,
berpakaian, toileting dan ambulasi)
- Monitor kemampuan pasien terhadap perawatan diri
- Monitor kebutuhan akan personal hygiene, berpakaian,
- Beri bantuan sampai klien mempunyai kemapuan untuk
- Bantu klien dalam memenuhi kebutuhan sehari-hari.
- Anjurkan & ajarkan klien untuk melakukan aktivitas
sehari-
- Pertahankan aktivitas perawatan diri secara rutin
- Evaluasi kemampuan klien dalam memenuhi kebutuhan
- Berikan reinforcement positip atas usaha yang
dilakukan 5
PK: Perdarahan
Setelah dilakukan askep …. jam perawat akan menangani
atau mengurangi komplikasi dari pada perdarahan
-Pantau tanda dan gejala perdarahan post operasi
(drainage, drip spool, urine)
- Monitor V/S
- Pantau laborat Hb, HMT. AT
- kolaborasi untuk tranfusi bila terjadi perdarahan (hb < -
Kolaborasi dengan dokter untuk terapinya
- Pantau perdarahan pada daerah yang dilakukan operasi
You might also like
- Simon Bricker Short Answer QuestionsDocument280 pagesSimon Bricker Short Answer Questionskaran270100% (4)
- Patient Medication ProfileDocument14 pagesPatient Medication ProfileJean Ganub100% (3)
- 3 - Toronto Notes 2011 - Anesthesia - and - Peri-Operative - MedicineDocument28 pages3 - Toronto Notes 2011 - Anesthesia - and - Peri-Operative - MedicineHisham Qassrawi100% (1)
- The 42 Negative ConfessionsDocument2 pagesThe 42 Negative ConfessionsBenne James100% (1)
- Teyber Process CommentsDocument8 pagesTeyber Process Commentstomdolak100% (1)
- Con Law II ChecklistDocument12 pagesCon Law II Checklistjclavet39No ratings yet
- CPPT in The IcuDocument39 pagesCPPT in The Icueyob kaseyeNo ratings yet
- 1095 Preoperative Risk Stratification and OptimizationDocument99 pages1095 Preoperative Risk Stratification and OptimizationHening Tirta KusumawardaniNo ratings yet
- Essentials of Anesthesia For Medical Students FinalDocument82 pagesEssentials of Anesthesia For Medical Students FinalEs LamNo ratings yet
- Model Answer -I & II سبتمبر 2015تحريريDocument12 pagesModel Answer -I & II سبتمبر 2015تحريريAmr El TaherNo ratings yet
- Abdominal Trauma From Nursing Perspective: JunaediDocument50 pagesAbdominal Trauma From Nursing Perspective: JunaediDana KhoirulNo ratings yet
- Pre Operative AssessmentDocument33 pagesPre Operative AssessmentShimmering MoonNo ratings yet
- Persiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007Document22 pagesPersiapan Pra Operasi: Bagian/ SMF Anestesiologi Rs Islam Sultan Agung/ Fakultas Kedokteran Unissula 2007ariahenkusNo ratings yet
- Medical Emergency Oral Q.docx26.docx8Document44 pagesMedical Emergency Oral Q.docx26.docx8Simina ÎntunericNo ratings yet
- Basics of AnesthesiaDocument34 pagesBasics of Anesthesianicolinna2000yahoo.comNo ratings yet
- Saq 1Document68 pagesSaq 1joe kayongoNo ratings yet
- Care of Critical Ill PatientDocument53 pagesCare of Critical Ill PatientindraNo ratings yet
- 1 PreoperativeDocument67 pages1 PreoperativeMoayad NawaflehNo ratings yet
- General Anesthesia: Dr. Rasha S BondokDocument38 pagesGeneral Anesthesia: Dr. Rasha S BondokRadwa ShokryNo ratings yet
- Anesthesia CasesDocument19 pagesAnesthesia Casesالدعوه الحسنهNo ratings yet
- Ncm106 Week 15 IcuDocument15 pagesNcm106 Week 15 IcuMichelle MallareNo ratings yet
- Anesthetic AssesmentDocument65 pagesAnesthetic AssesmentDR BUYINZA TITUSNo ratings yet
- 1-Anesthetic Assesment & PremedicationDocument77 pages1-Anesthetic Assesment & PremedicationAnanth SusruthNo ratings yet
- Preoperative Evaluation and Considerations in ChildrenDocument24 pagesPreoperative Evaluation and Considerations in ChildrenArshan AliNo ratings yet
- PDF 2Document46 pagesPDF 2kevandmwnNo ratings yet
- 0-306-48407-2 - 35 - 2023-02-23T214346.871Document13 pages0-306-48407-2 - 35 - 2023-02-23T214346.871drsubramanianNo ratings yet
- Aneurisma Aorta AbdominalisDocument36 pagesAneurisma Aorta AbdominalisMutivanya Inez MaharaniNo ratings yet
- Basics of AnaesthesiaDocument34 pagesBasics of Anaesthesiadremad1974No ratings yet
- Anestesi Abdominal ApproachDocument14 pagesAnestesi Abdominal ApproachabdulkadirmunsyNo ratings yet
- Perawatan Pasca AnestesiDocument27 pagesPerawatan Pasca AnestesiMeyNo ratings yet
- Care of The Patient in The Perioperative PeriodDocument20 pagesCare of The Patient in The Perioperative PeriodMohammed FaragNo ratings yet
- Preoperative Assessment and Premedication - PACUDocument60 pagesPreoperative Assessment and Premedication - PACUTraceNo ratings yet
- A Case Presentation On Polytrauma New2Document34 pagesA Case Presentation On Polytrauma New2FERDINAND ATSERNo ratings yet
- Preoperative Assessment - Doctor'sDocument15 pagesPreoperative Assessment - Doctor'sbz6dgr4gsvNo ratings yet
- Emergency MedicineDocument46 pagesEmergency MedicinekararobeedNo ratings yet
- Cabg 130102113345 Phpapp01Document29 pagesCabg 130102113345 Phpapp01md.dascalescu2486No ratings yet
- Angina OutlineDocument4 pagesAngina OutlineJerick Michael FrancoNo ratings yet
- Pre OpDocument104 pagesPre OpRobelNo ratings yet
- Pre-Anesthetic Care and Patients Optimization: Presenter: Dr. Mwasapi P. PDocument96 pagesPre-Anesthetic Care and Patients Optimization: Presenter: Dr. Mwasapi P. PfadhiliNo ratings yet
- 01. 麻醉前評估 - 陳坤堡Document58 pages01. 麻醉前評估 - 陳坤堡kenny631653No ratings yet
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterNo ratings yet
- Preop Assess in AnesthesiaDocument32 pagesPreop Assess in AnesthesiaEva PerdanaNo ratings yet
- IKA Jack Lala 28 MeiDocument19 pagesIKA Jack Lala 28 MeijamalNo ratings yet
- Cont Cardiac D SesDocument58 pagesCont Cardiac D SesChristian Allen SibalaNo ratings yet
- Kunjungan Pre AnestesiDocument22 pagesKunjungan Pre AnestesiAlisya NadhilahNo ratings yet
- Cardiovascular InvestigationDocument51 pagesCardiovascular InvestigationSarahafattahNo ratings yet
- ATLSDocument116 pagesATLSadindaNo ratings yet
- Approach To TruamaDocument29 pagesApproach To TruamaIbsa ShumaNo ratings yet
- Anesthetic Assesment & PremedicationDocument82 pagesAnesthetic Assesment & PremedicationahmedNo ratings yet
- Pre AnestesiDocument64 pagesPre AnestesiKevin YonathanNo ratings yet
- Preanaesthetic Evaluation: DR - Gunupuru BharatDocument89 pagesPreanaesthetic Evaluation: DR - Gunupuru Bharatbharat singhNo ratings yet
- 7 Preop and Postoperative CareDocument71 pages7 Preop and Postoperative CareHailemariam MebratuNo ratings yet
- Anesthesiology PrimerDocument10 pagesAnesthesiology PrimerJamesNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- Persiapan Pra OperasiDocument22 pagesPersiapan Pra Operasiyanayas28No ratings yet
- Principles of Gynecological Surgeries 1Document127 pagesPrinciples of Gynecological Surgeries 1Mohammad AlrefaiNo ratings yet
- Approach To Trauma PatientDocument36 pagesApproach To Trauma PatientTitusNo ratings yet
- Principles in Trauma ManagementDocument34 pagesPrinciples in Trauma Managementvirz23No ratings yet
- Chapter 20 Nursing Management Postoperative CareDocument7 pagesChapter 20 Nursing Management Postoperative Caredcrisostomo8010No ratings yet
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- HYSTERECTOMY Tuazon SapanDocument58 pagesHYSTERECTOMY Tuazon SapanMonette Abalos MendovaNo ratings yet
- Trauma KepalaDocument31 pagesTrauma KepalaMuhammad ArifNo ratings yet
- IPX On VistaDocument3 pagesIPX On Vistahafid nugrohoNo ratings yet
- 77c Abstract BookDocument196 pages77c Abstract BookRunde P PutraNo ratings yet
- SdarticleDocument8 pagesSdarticlehafid nugrohoNo ratings yet
- An Integrative Model of Adolescent Health Risk Behavior: Heidi J. Keeler RN, BSN, Margaret M. Kaiser PHD, Aprn-CnsDocument12 pagesAn Integrative Model of Adolescent Health Risk Behavior: Heidi J. Keeler RN, BSN, Margaret M. Kaiser PHD, Aprn-Cnshafid nugrohoNo ratings yet
- SdarticleDocument8 pagesSdarticlehafid nugrohoNo ratings yet
- Heat Matrass, Warm BlanketDocument14 pagesHeat Matrass, Warm Blankethafid nugrohoNo ratings yet
- Calcium and Dairy Intakes of Adolescents Are Associated With Their Home Environment, Taste Preferences, Personal Health Beliefs, and Meal PatternsDocument9 pagesCalcium and Dairy Intakes of Adolescents Are Associated With Their Home Environment, Taste Preferences, Personal Health Beliefs, and Meal Patternshafid nugrohoNo ratings yet
- Perioperative Hypothermia: The New England Journal of MedicineDocument36 pagesPerioperative Hypothermia: The New England Journal of Medicinehafid nugrohoNo ratings yet
- Peran & Perilaku KesehatanDocument49 pagesPeran & Perilaku Kesehatanhafid nugroho100% (1)
- Pencegahan Hi Perter Mi Dan Hipotermi Imbalance Body TemperatureDocument9 pagesPencegahan Hi Perter Mi Dan Hipotermi Imbalance Body Temperaturehafid nugrohoNo ratings yet
- Risk Factor For Latex AllergyDocument34 pagesRisk Factor For Latex Allergyhafid nugrohoNo ratings yet
- Dressing Luka BakarDocument44 pagesDressing Luka Bakarhafid nugrohoNo ratings yet
- Kebutuhan Fisiologis: Sensori, Persepsi, KognitifDocument43 pagesKebutuhan Fisiologis: Sensori, Persepsi, Kognitifhafid nugrohoNo ratings yet
- (1994) The Stationary Bootstrap - Politis and RomanoDocument12 pages(1994) The Stationary Bootstrap - Politis and RomanoGabe LinNo ratings yet
- PREVIEW Cognos SDK Guide by BI CentreDocument12 pagesPREVIEW Cognos SDK Guide by BI CentreHadi AamirNo ratings yet
- This World Is YoursDocument2 pagesThis World Is YoursAngelo SuguitanNo ratings yet
- 10 8 FrenchenlightenmentDocument10 pages10 8 FrenchenlightenmentNicholas ColemanNo ratings yet
- 7 Types of English Adjectives That Every ESL Student Must Know - FluentU English PDFDocument16 pages7 Types of English Adjectives That Every ESL Student Must Know - FluentU English PDFSuvashreePradhanNo ratings yet
- 1 - Table4 PRAFORMA KPD60204 Model-Model PengajaranDocument4 pages1 - Table4 PRAFORMA KPD60204 Model-Model PengajaranTan Jun YouNo ratings yet
- Taguig City UniversityDocument48 pagesTaguig City UniversityJayson CalbanNo ratings yet
- Valenzuela City Polytechnic College: Electrical Installation & MaintenanceDocument2 pagesValenzuela City Polytechnic College: Electrical Installation & MaintenanceMonnalou FarrellyNo ratings yet
- Diane Richardson's AppDocument9 pagesDiane Richardson's Apptopher_sandersNo ratings yet
- Electromagnetism Laws and Equations: Andrew Mchutchon Michaelmas 2013Document13 pagesElectromagnetism Laws and Equations: Andrew Mchutchon Michaelmas 2013Burhan AliNo ratings yet
- I Wonder PoemDocument9 pagesI Wonder PoemPaakkialetchumi NarainasamyNo ratings yet
- 1921 ADirectory of CeremonialDocument96 pages1921 ADirectory of CeremonialWade SperryNo ratings yet
- Urban RenewalDocument6 pagesUrban RenewalashimaNo ratings yet
- Crim Law II ReviewerDocument157 pagesCrim Law II ReviewerJierah ManahanNo ratings yet
- CivilsyllDocument131 pagesCivilsyllYashwanth YashuNo ratings yet
- Agri Crop Production Lo1 Lo3Document40 pagesAgri Crop Production Lo1 Lo3AV Montes100% (14)
- Doi:10 3934/dcds 2022096Document26 pagesDoi:10 3934/dcds 2022096Mehtar YNo ratings yet
- Self-Assessment 9.8: For Each Learning Objective, Tick ( ) The Box That Best Matches Your AbilityDocument1 pageSelf-Assessment 9.8: For Each Learning Objective, Tick ( ) The Box That Best Matches Your AbilityКатерина КравченкоNo ratings yet
- Employee Data (Application) FormDocument2 pagesEmployee Data (Application) FormGlaneisia MitchellNo ratings yet
- ResearchDocument21 pagesResearchmirrorsanNo ratings yet
- Criminal Complaint Us 500 & 506 RW Sec. 34 of The Indian Penal Code-Drafting-Criminal Template-1098Document3 pagesCriminal Complaint Us 500 & 506 RW Sec. 34 of The Indian Penal Code-Drafting-Criminal Template-1098Sky78% (18)
- 028-Golden Donuts, Inc. v. NLRC G.R. Nos. 113666-68 January 19, 2000Document6 pages028-Golden Donuts, Inc. v. NLRC G.R. Nos. 113666-68 January 19, 2000Jopan SJNo ratings yet
- Meniscal Repair Rehab 2012 PDFDocument13 pagesMeniscal Repair Rehab 2012 PDFrdkelsallNo ratings yet
- Business CommunicationDocument3 pagesBusiness Communicationmalikatif42100% (1)
- Saint Patapios of Thebes and His Monastery in Loutraki PDFDocument5 pagesSaint Patapios of Thebes and His Monastery in Loutraki PDFgandalfthereader2130No ratings yet
- Chapter 2-National Income AccountingDocument78 pagesChapter 2-National Income AccountingOrn PhatthayaphanNo ratings yet