Download as pdf or txt
You might also like
- The Perceptions of de La Salle University-Dasmarinas Senior High School Students Regarding The Mandatory ROTC2Document80 pagesThe Perceptions of de La Salle University-Dasmarinas Senior High School Students Regarding The Mandatory ROTC2Kurt ApoleNo ratings yet
- The RBI Policy Challenge 2017Document3 pagesThe RBI Policy Challenge 2017Ani DalalNo ratings yet
- 2014-08-03 09.09.53 6Document9 pages2014-08-03 09.09.53 6Nag Mallesh RaoNo ratings yet
- Watson 2004Document7 pagesWatson 2004Oscar Andrés PinillaNo ratings yet
- Stroke VolumeDocument10 pagesStroke VolumeAnonymous oQtve4oNo ratings yet
- Ischemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesDocument6 pagesIschemic Heart Disease and Diagnostic Coronary Angiographyepidemiological Data and Femoral vs. Radial Approach: A Series of 100 CasesIJAR JOURNALNo ratings yet
- TEE Surgical Decision Making - June2020 PDFDocument43 pagesTEE Surgical Decision Making - June2020 PDFalina100% (1)
- Pi Is 0894731723005333Document62 pagesPi Is 0894731723005333ВалентинаNo ratings yet
- An Analysis of The Geometry of Saccular IntracraniDocument12 pagesAn Analysis of The Geometry of Saccular IntracraniAnnetNo ratings yet
- Ultrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015Document10 pagesUltrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015angelama1783riosNo ratings yet
- HVS 3Document8 pagesHVS 3Teodora EremiaNo ratings yet
- 01 02 03Document8 pages01 02 03alingh98No ratings yet
- Sheikh Et Al 2020 - Meta-Analysis Utility of IVUS in PVIDocument10 pagesSheikh Et Al 2020 - Meta-Analysis Utility of IVUS in PVINobby MonicaNo ratings yet
- Cardiac ValveDocument9 pagesCardiac Valveikbal rambalinoNo ratings yet
- 5550-Article Text-42309-3-10-20220104Document8 pages5550-Article Text-42309-3-10-20220104the OGs. 96No ratings yet
- Postoperative Care in Thoracic SurgeryDocument8 pagesPostoperative Care in Thoracic SurgeryAngélica ContrerasNo ratings yet
- Schizophrenia in CardiacDocument8 pagesSchizophrenia in CardiacValentina RodriguezNo ratings yet
- 2018 Article 1428Document8 pages2018 Article 1428Kh RafikaNo ratings yet
- Standardized Echo Report Rev1Document38 pagesStandardized Echo Report Rev1Arnaldo Santizo SáenzNo ratings yet
- Cavaillols1995 PDFDocument10 pagesCavaillols1995 PDFGad AliNo ratings yet
- Sacks2018 PDFDocument13 pagesSacks2018 PDFJonathan Paucar ArévaloNo ratings yet
- Posters (Third Part) : SciencedirectDocument2 pagesPosters (Third Part) : SciencedirectshewaleakhileshNo ratings yet
- Use of Ultrasonography As A Diagnostic and Therapeutic ToolDocument11 pagesUse of Ultrasonography As A Diagnostic and Therapeutic ToolVojtěch ŠmídNo ratings yet
- Standardized Echo Report Rev1Document38 pagesStandardized Echo Report Rev1dgina8800100% (1)
- Echo 2Document16 pagesEcho 2Indera VyasNo ratings yet
- PIIS0749070413000742Document46 pagesPIIS0749070413000742Juan Carlos MezaNo ratings yet
- 10.1016@S0140 67361931721 0Document7 pages10.1016@S0140 67361931721 0Oana DrăganNo ratings yet
- Cardiac MR Assessment of Right Ventricular Function in Acquired Heart Disease - Factors of Variability Jérôme CaudronDocument12 pagesCardiac MR Assessment of Right Ventricular Function in Acquired Heart Disease - Factors of Variability Jérôme CaudronLY SovantolaNo ratings yet
- Repair of Rotator Cuff Tears in The Elderly: Does It Make Sense?Document10 pagesRepair of Rotator Cuff Tears in The Elderly: Does It Make Sense?Gustavo BECERRA PERDOMONo ratings yet
- EE Pac Con FADocument6 pagesEE Pac Con FAGuillermo CenturionNo ratings yet
- Impaired Left Ventricular Apical Rotation Is Associated With Disease Activity of Psoriatic ArthritisDocument8 pagesImpaired Left Ventricular Apical Rotation Is Associated With Disease Activity of Psoriatic ArthritisEmanuel NavarreteNo ratings yet
- Detrano 1989Document7 pagesDetrano 1989Lilims LilithNo ratings yet
- Jer 206 BBBDocument31 pagesJer 206 BBBVina SalsabilaNo ratings yet
- Jurnal Mba Sari 1Document44 pagesJurnal Mba Sari 1PitoAdhiNo ratings yet
- Accuracy of Imaging Technologies in The DiagnosisDocument7 pagesAccuracy of Imaging Technologies in The DiagnosisAGGREY DUDUNo ratings yet
- Automatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionDocument9 pagesAutomatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionMiguelNo ratings yet
- Jurnal OmiDocument14 pagesJurnal OmiYogie YahuiNo ratings yet
- Impingement Femoroacetabular AsintomaticosDocument6 pagesImpingement Femoroacetabular AsintomaticosMathias TaritolayNo ratings yet
- Management of Acute Limb Ischemia in The Pediatric PopulationDocument5 pagesManagement of Acute Limb Ischemia in The Pediatric PopulationPendidikan Dokter Unsyiah 2015No ratings yet
- MR Angiography and 2-D Phase-Contrast Imaging For EvaluationDocument7 pagesMR Angiography and 2-D Phase-Contrast Imaging For EvaluationSkander GharbiNo ratings yet
- Comparison of Echocardiographic Single-Plane Biplane LADocument7 pagesComparison of Echocardiographic Single-Plane Biplane LAWirawan PrabowoNo ratings yet
- Yejvs - 7376Document14 pagesYejvs - 7376Francisco Álvarez MarcosNo ratings yet
- Electrocardiographic Biosignals To Predict Atrial Fibrillation Are We There YetDocument2 pagesElectrocardiographic Biosignals To Predict Atrial Fibrillation Are We There YetsunhaolanNo ratings yet
- Discordance Between Echocardiography and MRI in The Assessment of Mitral Regurgitation SeverityDocument11 pagesDiscordance Between Echocardiography and MRI in The Assessment of Mitral Regurgitation SeverityPanfilAlinaNo ratings yet
- Han2011 PDFDocument5 pagesHan2011 PDFVinnie Juliana YonatanNo ratings yet
- Cardio EstudantesDocument5 pagesCardio EstudantesNestor Torres MarinaNo ratings yet
- Ehf2 13519Document10 pagesEhf2 13519Defriyan RamziNo ratings yet
- Jurnal CT Cardiac 3Document27 pagesJurnal CT Cardiac 3Kakhfi Gemah PNo ratings yet
- Endarterectomy: Results From The Carotid Artery Revascularization and Clinical Referral Patterns For Carotid Artery Stenting Versus CarotidDocument10 pagesEndarterectomy: Results From The Carotid Artery Revascularization and Clinical Referral Patterns For Carotid Artery Stenting Versus CarotidDidier AdodoNo ratings yet
- Val Normale EchoDocument11 pagesVal Normale EchoAlexandra TofanNo ratings yet
- 1 s2.0 S266666852100063X MainDocument8 pages1 s2.0 S266666852100063X MainDina RyantiNo ratings yet
- ArticolsssaDocument11 pagesArticolsssaCosmin GabrielNo ratings yet
- Application of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationDocument8 pagesApplication of Strain and Other Echocardiographic Parameters in The Evaluation of Early and Long-Term Clinical Outcomes After Cardiac Surgery RevascularizationSondang JasmineNo ratings yet
- J.jacc.2018automated AFDocument8 pagesJ.jacc.2018automated AFdharsandipan86No ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- Pi Is 0300957221001544Document8 pagesPi Is 0300957221001544Peter ThaiNo ratings yet
- Bjs 11398Document9 pagesBjs 11398ratnayanti udinNo ratings yet
- Left Ventricular Global Longitudinal Strain Can ReDocument2 pagesLeft Ventricular Global Longitudinal Strain Can RemihaelamocanNo ratings yet
- Belykh, E., Krutko, A. V., Baykov, E. S., Giers, M. B., Preul, M. C., & Byvaltsev, V. A. (2017). Preoperative estimation of disc herniation recurrence after microdiscectomy predictive value of a multivariate model basedDocument11 pagesBelykh, E., Krutko, A. V., Baykov, E. S., Giers, M. B., Preul, M. C., & Byvaltsev, V. A. (2017). Preoperative estimation of disc herniation recurrence after microdiscectomy predictive value of a multivariate model basedRobert AndreiNo ratings yet
- Real-Time 3D Echo in Patient Selection For Cardiac Resynchronization TherapyDocument11 pagesReal-Time 3D Echo in Patient Selection For Cardiac Resynchronization TherapycesareNo ratings yet
- EchoMonitor2015 PDFDocument17 pagesEchoMonitor2015 PDFmarkleacockNo ratings yet
- Science 1202393Document8 pagesScience 1202393CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Structure and Function of The AAA - 2012 - Biochimica Et Biophysica Acta BBADocument13 pagesStructure and Function of The AAA - 2012 - Biochimica Et Biophysica Acta BBACARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Acid-Base And: Respiratory Properties of A Butrered Bovine Erythrocyte Perfusion MediumDocument6 pagesAcid-Base And: Respiratory Properties of A Butrered Bovine Erythrocyte Perfusion MediumCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Douetal 2014 SpringerDocument19 pagesDouetal 2014 SpringerCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Proteasomal AAA ATPases Struct - 2012 - Biochimica Et Biophysica Acta BBA - MDocument16 pagesProteasomal AAA ATPases Struct - 2012 - Biochimica Et Biophysica Acta BBA - MCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Triple Control Implications Cardiac Disease: of RelaxationDocument7 pagesTriple Control Implications Cardiac Disease: of RelaxationCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 2007-1Document9 pagesDirk L. Brutsaert 2007-1CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- The International Journal of Biochemistry & Cell BiologyDocument11 pagesThe International Journal of Biochemistry & Cell BiologyCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- ISNO Consensus Guidelines For Practical Adaptation of The WHO 2016 Classification of Adult Diffuse GliomasDocument11 pagesISNO Consensus Guidelines For Practical Adaptation of The WHO 2016 Classification of Adult Diffuse GliomasCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 1980Document16 pagesDirk L. Brutsaert 1980CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Multidimensional Scaling of Diffuse Gliomas ApplicDocument15 pagesMultidimensional Scaling of Diffuse Gliomas ApplicCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Chloride and Hydrogen Ion Distribution Between Human Red Cells and PlasmaDocument12 pagesChloride and Hydrogen Ion Distribution Between Human Red Cells and PlasmaCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 1993-1Document8 pagesDirk L. Brutsaert 1993-1CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Dirk L. Brutsaert 2007Document9 pagesDirk L. Brutsaert 2007CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- COP9 Signalosome: Discovery, Conservation, Activity, and FunctionDocument14 pagesCOP9 Signalosome: Discovery, Conservation, Activity, and FunctionCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Biomolecules: The COP9 Signalosome: A Multi-DUB ComplexDocument11 pagesBiomolecules: The COP9 Signalosome: A Multi-DUB ComplexCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Septal FascicleDocument13 pagesSeptal FascicleCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- A Nomogram For The Interpretation of Acid-Base Data: Summary: A Diagnostic Nomogram Based On Log pCODocument4 pagesA Nomogram For The Interpretation of Acid-Base Data: Summary: A Diagnostic Nomogram Based On Log pCOCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Arterial Blood Gas AssessmentsDocument55 pagesArterial Blood Gas AssessmentsCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Elife 12102 v3Document25 pagesElife 12102 v3CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Assessed by Cryo-Electron Microscopy and Structural Mass SpectrometryDocument37 pagesAssessed by Cryo-Electron Microscopy and Structural Mass SpectrometryCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Hexeberg 1993Document4 pagesHexeberg 1993CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- The EMBO Journal - 2021 - Mohamed - The CRL4DCAF1 Cullin RING Ubiquitin Ligase Is Activated Following A Switch inDocument14 pagesThe EMBO Journal - 2021 - Mohamed - The CRL4DCAF1 Cullin RING Ubiquitin Ligase Is Activated Following A Switch inCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- WNT Signaling in Adult Cardiac Hypertrophy and Remodeling: Lessons Learned From Cardiac DevelopmentDocument11 pagesWNT Signaling in Adult Cardiac Hypertrophy and Remodeling: Lessons Learned From Cardiac DevelopmentCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- American Society of Plant Biologists (ASPB)Document10 pagesAmerican Society of Plant Biologists (ASPB)CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- BPH 13922Document14 pagesBPH 13922CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Extended Atrial Conduction System Characterised by The Expression of The HCN4 Channel and Connexin45Document11 pagesExtended Atrial Conduction System Characterised by The Expression of The HCN4 Channel and Connexin45CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- 1059 FullDocument19 pages1059 FullCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Implications of The Hybrid Epithelial/mesenchymal Phenotype in MetastasisDocument19 pagesImplications of The Hybrid Epithelial/mesenchymal Phenotype in MetastasisCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Review ArticleDocument17 pagesReview ArticleCARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- Emg Movimientos de TricepsDocument38 pagesEmg Movimientos de TricepsVictor LopezNo ratings yet
- Types of Negotiation in IndiaDocument49 pagesTypes of Negotiation in IndiaBhavana ChaudhariNo ratings yet
- Integration & Differentiation A3 NotesDocument16 pagesIntegration & Differentiation A3 NotesTshering TashiNo ratings yet
- Chapter 1 MarketingDocument2 pagesChapter 1 MarketingYousef Abdullah GhundulNo ratings yet
- A Review of Artificial Intelligence Technologies To Achieve Machining ObjectivesDocument22 pagesA Review of Artificial Intelligence Technologies To Achieve Machining ObjectivesSaksham SetiaNo ratings yet
- Theory Questions (1-7)Document2 pagesTheory Questions (1-7)sharmadisha0703No ratings yet
- Agency Finals ReviewerDocument61 pagesAgency Finals ReviewerRyan ChristianNo ratings yet
- Worksheet G10 AnalyticalChemistryDocument2 pagesWorksheet G10 AnalyticalChemistrySantanuNo ratings yet
- Pasaka FestivalDocument9 pagesPasaka FestivalBaymaxNo ratings yet
- Burisch Don Dep Rain DancerDocument59 pagesBurisch Don Dep Rain DancersisterrosettaNo ratings yet
- Thesis It Na JudDocument38 pagesThesis It Na JudNepoy Beltran EntendezNo ratings yet
- Community Guidelines - TikTok - March 2023 - Integrity and AuthencityDocument5 pagesCommunity Guidelines - TikTok - March 2023 - Integrity and AuthencityAline IraminaNo ratings yet
- Annual Report 2012-13Document46 pagesAnnual Report 2012-13Ar123No ratings yet
- Mathematical Logic in The Human BrainDocument23 pagesMathematical Logic in The Human BrainEugenia LupuNo ratings yet
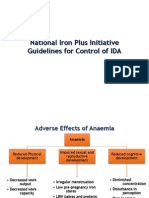
- National Iron Plus Initiative Guidelines For Controlof IDADocument19 pagesNational Iron Plus Initiative Guidelines For Controlof IDAvvirumbi100% (1)
- StarbucksDocument3 pagesStarbucksMonika SharmaNo ratings yet
- Uhlfelder v. DeSantisDocument2 pagesUhlfelder v. DeSantisKyle SNo ratings yet
- Point of View Quiz 2Document3 pagesPoint of View Quiz 2Telle TelleNo ratings yet
- (GUITAR TAB) One Direction - HistoryDocument2 pages(GUITAR TAB) One Direction - HistoryRoy Jonathan Hutajulu100% (1)
- Astrology - Am & RahukalamDocument2 pagesAstrology - Am & Rahukalamusf69No ratings yet
- Mathmatical PhysicsDocument7 pagesMathmatical PhysicsMr. DILLUNo ratings yet
- Finals Children's Program ScriptDocument4 pagesFinals Children's Program ScriptcharmainegloriosoNo ratings yet
- Personal Bible ReflectionsDocument176 pagesPersonal Bible ReflectionsRegino Joel B. Josol100% (1)
- Sociology Ia SampleDocument21 pagesSociology Ia SampleNattala DunkleyNo ratings yet
- Practical Research 2: Quarter 4 - Module 2 Quantitative Data-Collection TechniquesDocument3 pagesPractical Research 2: Quarter 4 - Module 2 Quantitative Data-Collection TechniquesLianne Lagayan100% (1)
- BTech Civil Engineering SyllabusDocument270 pagesBTech Civil Engineering SyllabusCharan KumarNo ratings yet
- Gallstones PD - 9Document18 pagesGallstones PD - 9drelvNo ratings yet
- (MATUTE, RODEL) Module-3-LESSON-1-SPEAR-3-TAKYANDocument4 pages(MATUTE, RODEL) Module-3-LESSON-1-SPEAR-3-TAKYANRodel MatuteNo ratings yet