
10849-Article Text-19904-1-10-20181107
10849-Article Text-19904-1-10-20181107
You might also like
- ECM3701 Electronic Communcation Technology: Minor Test No: 01 Year ModuleDocument4 pagesECM3701 Electronic Communcation Technology: Minor Test No: 01 Year ModuleTale Banks0% (1)
- QuantecDocument6 pagesQuantecapi-282901112No ratings yet
- Introduction To Spectroscopy Pavia 4th Solutions ManualDocument5 pagesIntroduction To Spectroscopy Pavia 4th Solutions Manualسیاہ پوش100% (1)
- Creating Custom SU01 Transaction Code With Display and Password Reset Buttons PDFDocument7 pagesCreating Custom SU01 Transaction Code With Display and Password Reset Buttons PDFSanjay DesaiNo ratings yet
- VM EnginesDocument7 pagesVM EnginesraulNo ratings yet
- Live ProjectDocument53 pagesLive Projectritesh chauhanNo ratings yet
- Sadki Xie Chauvin 2011Document26 pagesSadki Xie Chauvin 2011NadiaNadiaNo ratings yet
- 170 Arun KumarDocument6 pages170 Arun KumarRiyazkhan MpNo ratings yet
- Intensive Care Unit NursingDocument10 pagesIntensive Care Unit NursingCute Clothing Store0% (1)
- Evidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsDocument11 pagesEvidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsSarahi Rodriguez GalindoNo ratings yet
- 1 s2.0 S0168851019301563 MainDocument8 pages1 s2.0 S0168851019301563 MainAprillianRizkyaNo ratings yet
- Assessment of KnowledgeDocument17 pagesAssessment of KnowledgeNiningNo ratings yet
- Machine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating TheatreDocument24 pagesMachine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating Theatreayed latifaNo ratings yet
- Anthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFDocument6 pagesAnthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFAiya Auri GumantiNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- Intensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Document48 pagesIntensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Indhu JayavelNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- Critical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesDocument6 pagesCritical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesAngela SaoNo ratings yet
- Quality and Safety in AnaesthesiaDocument10 pagesQuality and Safety in Anaesthesiaanna67890No ratings yet
- The International Journal of Humanities & Social StudiesDocument12 pagesThe International Journal of Humanities & Social StudiesmarcosdabataNo ratings yet
- Turning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewDocument12 pagesTurning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewfajaqaNo ratings yet
- LJMU Research Online: Intend To Cite From This Work)Document18 pagesLJMU Research Online: Intend To Cite From This Work)AbeerNo ratings yet
- An Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CareDocument18 pagesAn Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CarePATRICK OTIATONo ratings yet
- The Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsDocument12 pagesThe Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsKanameMizumiNo ratings yet
- Diagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical TechnologyDocument11 pagesDiagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical Technologycarmen rosa secce pedrazaNo ratings yet
- Integrative Review of The LiteratureDocument25 pagesIntegrative Review of The Literatureapi-540011183No ratings yet
- SBRT PDFDocument14 pagesSBRT PDFrubenNo ratings yet
- Real ProposalDocument16 pagesReal ProposalAlamgir Khan YousafzaiNo ratings yet
- Validation of A Tool To Assess Patient Satisfaction Waiting Times Healthcare Utilization and CostDocument8 pagesValidation of A Tool To Assess Patient Satisfaction Waiting Times Healthcare Utilization and Costokta sariNo ratings yet
- Laparoscopic Versus Open Pediatric Inguinal Hernia RepairDocument15 pagesLaparoscopic Versus Open Pediatric Inguinal Hernia Repairmelon segerNo ratings yet
- Costs of Hospital MalnutritionDocument6 pagesCosts of Hospital MalnutritionAmalia SarsolNo ratings yet
- Comunikasi Dengan Pasien Sadar Venti Sist ReviewDocument14 pagesComunikasi Dengan Pasien Sadar Venti Sist Reviewemil kemenkesNo ratings yet
- Intensive Care Unit (ICU) Readmission: A Mixed-Method Systematic ReviewDocument7 pagesIntensive Care Unit (ICU) Readmission: A Mixed-Method Systematic ReviewSupitchaya WiNo ratings yet
- 10.1186@s13017 018 0185 2Document13 pages10.1186@s13017 018 0185 2Roque Alberto PríncipeNo ratings yet
- Anaesthesia - 2018 - Apricot 2 Severe Critical Events in Paediatric Anaesthesia in The United KingdomDocument12 pagesAnaesthesia - 2018 - Apricot 2 Severe Critical Events in Paediatric Anaesthesia in The United KingdomAbisaid Jonathan Salinas MemijeNo ratings yet
- Shortstay LiteratureDocument5 pagesShortstay LiteratureDon RicaforteNo ratings yet
- Hypertensive Disorders in PregnancyDocument15 pagesHypertensive Disorders in PregnancyHania AliNo ratings yet
- Design of A Model To Predict Surge Capacity Bottlenecks For Burn Mass Casualties at A Large Academic Medical CenterDocument10 pagesDesign of A Model To Predict Surge Capacity Bottlenecks For Burn Mass Casualties at A Large Academic Medical CenterSaraNo ratings yet
- Critique..Senior ProjectDocument19 pagesCritique..Senior Projectmykitkat1973No ratings yet
- p2 - Patients and Carers Experiences of InteractingDocument12 pagesp2 - Patients and Carers Experiences of InteractingShruthi KrishnamoorthyNo ratings yet
- Davenport 2004Document12 pagesDavenport 2004Licitacion04 msNo ratings yet
- Corticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisDocument10 pagesCorticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisEviNo ratings yet
- Intensivist To Patient RatioDocument8 pagesIntensivist To Patient RatioroykelumendekNo ratings yet
- HHS Public AccessDocument19 pagesHHS Public AccesschristienNo ratings yet
- Lit Review of Nursing RoleDocument11 pagesLit Review of Nursing RoleSnowyNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- European J Cancer Care - 2021 - Kerr - Evaluation of The Role of The Clinical Nurse Specialist in Cancer Care AnDocument13 pagesEuropean J Cancer Care - 2021 - Kerr - Evaluation of The Role of The Clinical Nurse Specialist in Cancer Care AnmfarooqafzalNo ratings yet
- A Human FactorsDocument19 pagesA Human FactorsYonataNo ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- I J C C M: Ndian Ournal Ritical ARE EdicineDocument5 pagesI J C C M: Ndian Ournal Ritical ARE EdicinedranilbgNo ratings yet
- Comparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessDocument6 pagesComparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessS3V4_9154No ratings yet
- Imaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusDocument9 pagesImaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusPacoNo ratings yet
- Disiplin CareDocument6 pagesDisiplin CareOnea Nie NierwanaNo ratings yet
- Neuroblastoma Current Imaging and TherapeuticsDocument22 pagesNeuroblastoma Current Imaging and TherapeuticsLeddyNo ratings yet
- Forecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationDocument8 pagesForecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationARTZchebilNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- Merola 2021Document10 pagesMerola 2021FedericoNo ratings yet
- Safety of Cupping Therapy in Studies Conducted in Twenty One Century: A Review of LiteratureDocument12 pagesSafety of Cupping Therapy in Studies Conducted in Twenty One Century: A Review of LiteratureMona HassanNo ratings yet
- Ni Hms 765335Document21 pagesNi Hms 765335cricket66No ratings yet
- Jurnal InternasionalDocument7 pagesJurnal InternasionalDina AryaniNo ratings yet
- Evaluating Barriers To Adopting Telemedicine WorldDocument9 pagesEvaluating Barriers To Adopting Telemedicine WorldAlbertus FrediNo ratings yet
- Litz 2017Document4 pagesLitz 2017ilsa ArfiyanaNo ratings yet
- Fall RiskDocument10 pagesFall Riskjinsi georgeNo ratings yet
- The SAGES Manual: Volume 2 Advanced Laparoscopy and EndoscopyFrom EverandThe SAGES Manual: Volume 2 Advanced Laparoscopy and EndoscopyNo ratings yet
- Test Oil Compressor #4067 (06-12-22)Document1 pageTest Oil Compressor #4067 (06-12-22)albertoNo ratings yet
- Assessment 1 IMINT Exercise BRAVODocument6 pagesAssessment 1 IMINT Exercise BRAVOYousef Al HashemiNo ratings yet
- Bad For Democracy How The Presidency Undermines The Power of The PeopleDocument272 pagesBad For Democracy How The Presidency Undermines The Power of The PeoplePaulNo ratings yet
- RuttDocument6 pagesRuttJustinian FiloteosNo ratings yet
- CDP Virtual Appliance Getting Started GuideDocument18 pagesCDP Virtual Appliance Getting Started GuideJulio RodanesNo ratings yet
- The Multi-Crew Pilot Licence (MPL)Document28 pagesThe Multi-Crew Pilot Licence (MPL)Vivek ChaturvediNo ratings yet
- RINA NCC92 - Rules For The Type Approval CertificationDocument9 pagesRINA NCC92 - Rules For The Type Approval CertificationMarianoNo ratings yet
- Tyler Street News November 2010Document4 pagesTyler Street News November 2010tsumcNo ratings yet
- Historiography On The Origins of The Cold WarDocument4 pagesHistoriography On The Origins of The Cold Warapi-297872327100% (2)
- Circus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressDocument151 pagesCircus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressLaura GăvanNo ratings yet
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- Surcharge Preloading As A Method For Engineering Reservoir Foundations in Silty SoilsDocument6 pagesSurcharge Preloading As A Method For Engineering Reservoir Foundations in Silty SoilsBalaji MLNo ratings yet
- The Ascent and Decline of A Great Balneological Resort: PucioasaDocument6 pagesThe Ascent and Decline of A Great Balneological Resort: PucioasaStefan RaduNo ratings yet
- Super VIP Cheat Sheet: Arti Cial IntelligenceDocument18 pagesSuper VIP Cheat Sheet: Arti Cial IntelligenceAthaurRahmanNo ratings yet
- GuillermoAG - Reading The ImageDocument15 pagesGuillermoAG - Reading The ImageAdrienne Villanueva100% (1)
- ENIE - 100 Technical Communication Skills Week-1 Lecture # 1 & 2Document7 pagesENIE - 100 Technical Communication Skills Week-1 Lecture # 1 & 2HIMANo ratings yet
- Dairy Farm10Document3 pagesDairy Farm10GarNo ratings yet
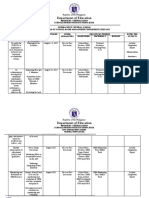
- Department of Education: Republic of The PhilippinesDocument3 pagesDepartment of Education: Republic of The PhilippinesRussel RapisoraNo ratings yet
- Article 1619693458Document10 pagesArticle 1619693458samrakshyaNo ratings yet
- Huawei Ban in The US: Projected Consequences For International TradeDocument4 pagesHuawei Ban in The US: Projected Consequences For International Trademuhammad samsu saputraNo ratings yet
- BEE301Document4 pagesBEE301cshohil300No ratings yet
- DB en Macx MCR T Ui Up 104595 en 10Document49 pagesDB en Macx MCR T Ui Up 104595 en 10Dante LupuNo ratings yet
- P PotassiumDocument12 pagesP PotassiumHeleneSmithNo ratings yet
- Dio125 and Hornet2 RepsolDocument2 pagesDio125 and Hornet2 RepsolSibi SundarNo ratings yet
- 001 GEYSERSD23Final PDFDocument100 pages001 GEYSERSD23Final PDFVasu ThakurNo ratings yet
























































































Download as pdf or txt
You might also like
- ECM3701 Electronic Communcation Technology: Minor Test No: 01 Year ModuleDocument4 pagesECM3701 Electronic Communcation Technology: Minor Test No: 01 Year ModuleTale Banks0% (1)
- QuantecDocument6 pagesQuantecapi-282901112No ratings yet
- Introduction To Spectroscopy Pavia 4th Solutions ManualDocument5 pagesIntroduction To Spectroscopy Pavia 4th Solutions Manualسیاہ پوش100% (1)
- Creating Custom SU01 Transaction Code With Display and Password Reset Buttons PDFDocument7 pagesCreating Custom SU01 Transaction Code With Display and Password Reset Buttons PDFSanjay DesaiNo ratings yet
- VM EnginesDocument7 pagesVM EnginesraulNo ratings yet
- Live ProjectDocument53 pagesLive Projectritesh chauhanNo ratings yet
- Sadki Xie Chauvin 2011Document26 pagesSadki Xie Chauvin 2011NadiaNadiaNo ratings yet
- 170 Arun KumarDocument6 pages170 Arun KumarRiyazkhan MpNo ratings yet
- Intensive Care Unit NursingDocument10 pagesIntensive Care Unit NursingCute Clothing Store0% (1)
- Evidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsDocument11 pagesEvidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsSarahi Rodriguez GalindoNo ratings yet
- 1 s2.0 S0168851019301563 MainDocument8 pages1 s2.0 S0168851019301563 MainAprillianRizkyaNo ratings yet
- Assessment of KnowledgeDocument17 pagesAssessment of KnowledgeNiningNo ratings yet
- Machine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating TheatreDocument24 pagesMachine Learning Based Integrated Scheduling and Rescheduling For Elective and Emergency Patients in The Operating Theatreayed latifaNo ratings yet
- Anthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFDocument6 pagesAnthropometric Measurement of Patients Admitted To An Intensive Care Unit Jpcic 1000113 PDFAiya Auri GumantiNo ratings yet
- Efficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisDocument10 pagesEfficacy and Safety of Topical Oxygen Therapy For Diabetic Foot Ulcers: An Updated Systematic Review and Meta-AnalysisChangjing ZhangNo ratings yet
- Intensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Document48 pagesIntensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Indhu JayavelNo ratings yet
- Get Homework/Assignment DoneDocument6 pagesGet Homework/Assignment Donehomeworkping1No ratings yet
- Critical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesDocument6 pagesCritical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesAngela SaoNo ratings yet
- Quality and Safety in AnaesthesiaDocument10 pagesQuality and Safety in Anaesthesiaanna67890No ratings yet
- The International Journal of Humanities & Social StudiesDocument12 pagesThe International Journal of Humanities & Social StudiesmarcosdabataNo ratings yet
- Turning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewDocument12 pagesTurning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewfajaqaNo ratings yet
- LJMU Research Online: Intend To Cite From This Work)Document18 pagesLJMU Research Online: Intend To Cite From This Work)AbeerNo ratings yet
- An Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CareDocument18 pagesAn Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CarePATRICK OTIATONo ratings yet
- The Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsDocument12 pagesThe Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsKanameMizumiNo ratings yet
- Diagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical TechnologyDocument11 pagesDiagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical Technologycarmen rosa secce pedrazaNo ratings yet
- Integrative Review of The LiteratureDocument25 pagesIntegrative Review of The Literatureapi-540011183No ratings yet
- SBRT PDFDocument14 pagesSBRT PDFrubenNo ratings yet
- Real ProposalDocument16 pagesReal ProposalAlamgir Khan YousafzaiNo ratings yet
- Validation of A Tool To Assess Patient Satisfaction Waiting Times Healthcare Utilization and CostDocument8 pagesValidation of A Tool To Assess Patient Satisfaction Waiting Times Healthcare Utilization and Costokta sariNo ratings yet
- Laparoscopic Versus Open Pediatric Inguinal Hernia RepairDocument15 pagesLaparoscopic Versus Open Pediatric Inguinal Hernia Repairmelon segerNo ratings yet
- Costs of Hospital MalnutritionDocument6 pagesCosts of Hospital MalnutritionAmalia SarsolNo ratings yet
- Comunikasi Dengan Pasien Sadar Venti Sist ReviewDocument14 pagesComunikasi Dengan Pasien Sadar Venti Sist Reviewemil kemenkesNo ratings yet
- Intensive Care Unit (ICU) Readmission: A Mixed-Method Systematic ReviewDocument7 pagesIntensive Care Unit (ICU) Readmission: A Mixed-Method Systematic ReviewSupitchaya WiNo ratings yet
- 10.1186@s13017 018 0185 2Document13 pages10.1186@s13017 018 0185 2Roque Alberto PríncipeNo ratings yet
- Anaesthesia - 2018 - Apricot 2 Severe Critical Events in Paediatric Anaesthesia in The United KingdomDocument12 pagesAnaesthesia - 2018 - Apricot 2 Severe Critical Events in Paediatric Anaesthesia in The United KingdomAbisaid Jonathan Salinas MemijeNo ratings yet
- Shortstay LiteratureDocument5 pagesShortstay LiteratureDon RicaforteNo ratings yet
- Hypertensive Disorders in PregnancyDocument15 pagesHypertensive Disorders in PregnancyHania AliNo ratings yet
- Design of A Model To Predict Surge Capacity Bottlenecks For Burn Mass Casualties at A Large Academic Medical CenterDocument10 pagesDesign of A Model To Predict Surge Capacity Bottlenecks For Burn Mass Casualties at A Large Academic Medical CenterSaraNo ratings yet
- Critique..Senior ProjectDocument19 pagesCritique..Senior Projectmykitkat1973No ratings yet
- p2 - Patients and Carers Experiences of InteractingDocument12 pagesp2 - Patients and Carers Experiences of InteractingShruthi KrishnamoorthyNo ratings yet
- Davenport 2004Document12 pagesDavenport 2004Licitacion04 msNo ratings yet
- Corticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisDocument10 pagesCorticosteroid Use and Intensive Care Unit-Acquired Weakness: A Systematic Review and Meta-AnalysisEviNo ratings yet
- Intensivist To Patient RatioDocument8 pagesIntensivist To Patient RatioroykelumendekNo ratings yet
- HHS Public AccessDocument19 pagesHHS Public AccesschristienNo ratings yet
- Lit Review of Nursing RoleDocument11 pagesLit Review of Nursing RoleSnowyNo ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- European J Cancer Care - 2021 - Kerr - Evaluation of The Role of The Clinical Nurse Specialist in Cancer Care AnDocument13 pagesEuropean J Cancer Care - 2021 - Kerr - Evaluation of The Role of The Clinical Nurse Specialist in Cancer Care AnmfarooqafzalNo ratings yet
- A Human FactorsDocument19 pagesA Human FactorsYonataNo ratings yet
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- I J C C M: Ndian Ournal Ritical ARE EdicineDocument5 pagesI J C C M: Ndian Ournal Ritical ARE EdicinedranilbgNo ratings yet
- Comparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessDocument6 pagesComparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessS3V4_9154No ratings yet
- Imaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusDocument9 pagesImaging in Suspected Renal Colic: Systematic Review of The Literature and Multispecialty ConsensusPacoNo ratings yet
- Disiplin CareDocument6 pagesDisiplin CareOnea Nie NierwanaNo ratings yet
- Neuroblastoma Current Imaging and TherapeuticsDocument22 pagesNeuroblastoma Current Imaging and TherapeuticsLeddyNo ratings yet
- Forecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationDocument8 pagesForecasting Emergency Department Crowding: A Prospective, Real-Time EvaluationARTZchebilNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- Merola 2021Document10 pagesMerola 2021FedericoNo ratings yet
- Safety of Cupping Therapy in Studies Conducted in Twenty One Century: A Review of LiteratureDocument12 pagesSafety of Cupping Therapy in Studies Conducted in Twenty One Century: A Review of LiteratureMona HassanNo ratings yet
- Ni Hms 765335Document21 pagesNi Hms 765335cricket66No ratings yet
- Jurnal InternasionalDocument7 pagesJurnal InternasionalDina AryaniNo ratings yet
- Evaluating Barriers To Adopting Telemedicine WorldDocument9 pagesEvaluating Barriers To Adopting Telemedicine WorldAlbertus FrediNo ratings yet
- Litz 2017Document4 pagesLitz 2017ilsa ArfiyanaNo ratings yet
- Fall RiskDocument10 pagesFall Riskjinsi georgeNo ratings yet
- The SAGES Manual: Volume 2 Advanced Laparoscopy and EndoscopyFrom EverandThe SAGES Manual: Volume 2 Advanced Laparoscopy and EndoscopyNo ratings yet
- Test Oil Compressor #4067 (06-12-22)Document1 pageTest Oil Compressor #4067 (06-12-22)albertoNo ratings yet
- Assessment 1 IMINT Exercise BRAVODocument6 pagesAssessment 1 IMINT Exercise BRAVOYousef Al HashemiNo ratings yet
- Bad For Democracy How The Presidency Undermines The Power of The PeopleDocument272 pagesBad For Democracy How The Presidency Undermines The Power of The PeoplePaulNo ratings yet
- RuttDocument6 pagesRuttJustinian FiloteosNo ratings yet
- CDP Virtual Appliance Getting Started GuideDocument18 pagesCDP Virtual Appliance Getting Started GuideJulio RodanesNo ratings yet
- The Multi-Crew Pilot Licence (MPL)Document28 pagesThe Multi-Crew Pilot Licence (MPL)Vivek ChaturvediNo ratings yet
- RINA NCC92 - Rules For The Type Approval CertificationDocument9 pagesRINA NCC92 - Rules For The Type Approval CertificationMarianoNo ratings yet
- Tyler Street News November 2010Document4 pagesTyler Street News November 2010tsumcNo ratings yet
- Historiography On The Origins of The Cold WarDocument4 pagesHistoriography On The Origins of The Cold Warapi-297872327100% (2)
- Circus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressDocument151 pagesCircus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressLaura GăvanNo ratings yet
- Chemistry Test 11 Chap 1-5Document2 pagesChemistry Test 11 Chap 1-5Sabitra RudraNo ratings yet
- Surcharge Preloading As A Method For Engineering Reservoir Foundations in Silty SoilsDocument6 pagesSurcharge Preloading As A Method For Engineering Reservoir Foundations in Silty SoilsBalaji MLNo ratings yet
- The Ascent and Decline of A Great Balneological Resort: PucioasaDocument6 pagesThe Ascent and Decline of A Great Balneological Resort: PucioasaStefan RaduNo ratings yet
- Super VIP Cheat Sheet: Arti Cial IntelligenceDocument18 pagesSuper VIP Cheat Sheet: Arti Cial IntelligenceAthaurRahmanNo ratings yet
- GuillermoAG - Reading The ImageDocument15 pagesGuillermoAG - Reading The ImageAdrienne Villanueva100% (1)
- ENIE - 100 Technical Communication Skills Week-1 Lecture # 1 & 2Document7 pagesENIE - 100 Technical Communication Skills Week-1 Lecture # 1 & 2HIMANo ratings yet
- Dairy Farm10Document3 pagesDairy Farm10GarNo ratings yet
- Department of Education: Republic of The PhilippinesDocument3 pagesDepartment of Education: Republic of The PhilippinesRussel RapisoraNo ratings yet
- Article 1619693458Document10 pagesArticle 1619693458samrakshyaNo ratings yet
- Huawei Ban in The US: Projected Consequences For International TradeDocument4 pagesHuawei Ban in The US: Projected Consequences For International Trademuhammad samsu saputraNo ratings yet
- BEE301Document4 pagesBEE301cshohil300No ratings yet
- DB en Macx MCR T Ui Up 104595 en 10Document49 pagesDB en Macx MCR T Ui Up 104595 en 10Dante LupuNo ratings yet
- P PotassiumDocument12 pagesP PotassiumHeleneSmithNo ratings yet
- Dio125 and Hornet2 RepsolDocument2 pagesDio125 and Hornet2 RepsolSibi SundarNo ratings yet
- 001 GEYSERSD23Final PDFDocument100 pages001 GEYSERSD23Final PDFVasu ThakurNo ratings yet