APPENDIX A:
SSM Health Risk Stratification Methodology for Monoclonal Antibody
Bamlanivimab and casirivimab/imdevimab infusions recently received Emergency Use Authorization by
the FDA. Bamlanivimab and casirivimab/imdevimab are monoclonal antibodies indicated for use in high
risk outpatients with mild/moderate COVID-19 to prevent hospitalization. The System AMS/ID
committee have developed a risk stratification system and scoring methodology created by the analyst
team within SSM Health based off the Utah Hospital Association and Utah Health Risk Stratification
criteria. This risk stratification system utilizes discrete criteria to determine patients at highest risk of
hospitalization and allocation of bamlanivimab and casirivimab/imdevimab to those at highest risk.
Given that bamlanivimab and casirivimab/imdevimab are more efficacious when administered earlier in
the disease course, administration should occur within 5 days of symptom onset.
Patient Selection Criteria
General Inclusion – for patients 12 years or older
• Laboratory-confirmed COVID-19 (PCR)
• Symptomatic, with no more than 5 days from symptom onset
• Positive Covid test within the last 4 days
• High Risk for Hospitalization based on Risk Stratification
Exclusion Criteria (any of the following):
• New Hypoxemia (SpO2<92% on room air or receiving new/increased
supplemental oxygen
• Being admitted or already admitted to an acute care hospital
• Pregnancy (inadequate safety data)
• Positive antibody test
*See Risk Stratification Tool section below
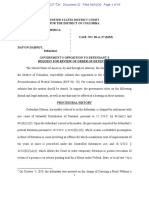
COVID-19 Risk Scoring Methodology
Demographic Risk Factors Points
Male 2
Age 3 for every decade:
12-19=3, 20-29=6, 30-39=9, 40-49=12, 50-
59=15, 60-69=18, 70-79=21, 80-89=24,
9099=27 30
Non-White Race or Hispanic/Latinx Ethnicity 7
Highest-Risk Comorbidities
Diabetes mellitus 3
Obesity (BMI>35) 1
Other High-Risk Comorbidities
Hypertension 1
Asthma 1
Symptom Risk Factor
New Shortness of Breath 4
Total
Ethical Justification for Using Race/Ethnicity in Patient Selection: COVID-19 has had a disproportionate
impact on low income communities and certain racial/ ethnic minorities in the United States. Equity calls
attention to the systematic differences in health outcomes and opportunities to be healthy that
adversely affect socially discounted and/or marginalized groups. For COVID-19, these inequities may
arise from higher burdens of preexisting comorbid disease, poor health care access, or not having the
option for social distancing due to living in densely populated neighborhoods or households. There are
also more economically disadvantaged individuals working essential jobs during the pandemic, and many
are unable to perform job functions from the safety of their home. This puts them at greater risk of
interacting with others who may transmit COVID-19. Public health interventions may be used to attempt
to mitigate these disparities in COVID-19 by recognizing the structural inequities that underlie them. One
way to do this is to include race/ethnicity in the patient selection criteria.
You might also like
- (DAILY CALLER OBTAINED) - Letter To National SJP 5.29.24Document4 pages(DAILY CALLER OBTAINED) - Letter To National SJP 5.29.24Henry RodgersNo ratings yet
- Swords of Iron: UNRWA-Hamas RelationsDocument5 pagesSwords of Iron: UNRWA-Hamas RelationsWashington Free Beacon100% (1)
- 2023-10-08 Emergency Meeting NotesDocument5 pages2023-10-08 Emergency Meeting NotesWashington Free BeaconNo ratings yet
- (DAILY CALLER OBTAINED) - Goldman Complaint 2Document12 pages(DAILY CALLER OBTAINED) - Goldman Complaint 2Henry Rodgers100% (2)
- Johnson Dear Colleague On New Israel BillDocument1 pageJohnson Dear Colleague On New Israel BillZerohedge JanitorNo ratings yet
- Abbe Lowell Letter To Comer Nov. 28Document3 pagesAbbe Lowell Letter To Comer Nov. 28James LynchNo ratings yet
- Leslie McAdoo Gordon: Position Statement As To Subpoenas With AddendumDocument25 pagesLeslie McAdoo Gordon: Position Statement As To Subpoenas With AddendumThe FederalistNo ratings yet
- Jim Jordan Letter To Merrick GarlandDocument2 pagesJim Jordan Letter To Merrick GarlandThe FederalistNo ratings yet
- Whistle-Blower's Letter To Congressional LeadersDocument16 pagesWhistle-Blower's Letter To Congressional LeadersJeffrey DunetzNo ratings yet
- Christopher Steele Ruling in Alfa Bank CaseDocument52 pagesChristopher Steele Ruling in Alfa Bank CaseChuck Ross67% (3)
- Jan 6Document154 pagesJan 6ZerohedgeNo ratings yet
- Letter To WH CounselDocument3 pagesLetter To WH CounselJames LynchNo ratings yet
- Dhs TV TP ReportDocument49 pagesDhs TV TP ReportSusan DuclosNo ratings yet
- Sidney Powell First Offender Terms Georgia Plea DealDocument3 pagesSidney Powell First Offender Terms Georgia Plea DealRobert GouveiaNo ratings yet
- 2016.10.26 - Doug Band MemoDocument12 pages2016.10.26 - Doug Band MemoZerohedge100% (2)
- Minnesota Chamber of Commerce v. ChoiDocument34 pagesMinnesota Chamber of Commerce v. ChoiScott JohnsonNo ratings yet
- New Venture Fund Document Preservation Notice RedactedDocument5 pagesNew Venture Fund Document Preservation Notice RedactedWashington Free BeaconNo ratings yet
- Jordan Letter To Wray 11/30Document4 pagesJordan Letter To Wray 11/30Gabe KaminskyNo ratings yet
- Jordan Letter To FBIDocument6 pagesJordan Letter To FBIThe FederalistNo ratings yet
- Jordan To WrayDocument6 pagesJordan To WrayWashington ExaminerNo ratings yet
- Government's Memorandum in Support of Detention, United States v. Smirnov (D. NV., Feb. 20, 2024), ECF No. 15Document28 pagesGovernment's Memorandum in Support of Detention, United States v. Smirnov (D. NV., Feb. 20, 2024), ECF No. 15Daily Caller News Foundation100% (1)
- House Oversight Letter To BowserDocument4 pagesHouse Oversight Letter To BowserHenry RodgersNo ratings yet
- 4.27.23 Letter To CDC Director Regarding Contradicting Pandemic GuidanceDocument3 pages4.27.23 Letter To CDC Director Regarding Contradicting Pandemic GuidanceMichael GinsbergNo ratings yet
- Hpsci Memo Key Points FinalDocument3 pagesHpsci Memo Key Points FinalBreitbart News100% (3)
- GOA: No Compromise Alliance PBRDocument2 pagesGOA: No Compromise Alliance PBRZerohedgeNo ratings yet
- Psaki Letter Regarding Ethics and Non-Federal EmploymentDocument6 pagesPsaki Letter Regarding Ethics and Non-Federal EmploymentWashington ExaminerNo ratings yet
- Quinnipiac Biden ApprovalDocument12 pagesQuinnipiac Biden ApprovalGregory PriceNo ratings yet
- Maricopa Board ArrestDocument2 pagesMaricopa Board ArrestRaheem Kassam100% (2)
- Jordan To GarlandDocument3 pagesJordan To GarlandWashington ExaminerNo ratings yet
- Biggs To MayorkasDocument9 pagesBiggs To MayorkasJohn BinderNo ratings yet
- Deb ArtmentDocument6 pagesDeb ArtmentZerohedge JanitorNo ratings yet
- White House Classified Docs - Special Counsel HurDocument3 pagesWhite House Classified Docs - Special Counsel HurBreitbart NewsNo ratings yet
- Gov - Uscourts.lawd.189520.301.0 1Document13 pagesGov - Uscourts.lawd.189520.301.0 1Susie MooreNo ratings yet
- Jake Sullivan Removal LetterDocument2 pagesJake Sullivan Removal LetterBreitbart NewsNo ratings yet
- Letter To Leadership On 2A Data PurchasesDocument4 pagesLetter To Leadership On 2A Data PurchasesZerohedge JanitorNo ratings yet
- Affirmative Action Letter FINAL1Document5 pagesAffirmative Action Letter FINAL1Washington ExaminerNo ratings yet
- 2024 05 09 Letter To IrsDocument4 pages2024 05 09 Letter To IrsZerohedge JanitorNo ratings yet
- Garland Memo DOJ IG RequestDocument4 pagesGarland Memo DOJ IG RequestMaurA Dowling100% (1)
- Oversight Republicans Seek Documents On Border Wall SaleDocument5 pagesOversight Republicans Seek Documents On Border Wall SaleFox NewsNo ratings yet
- Letter To GAO From Senators Toomey and JohnsonDocument3 pagesLetter To GAO From Senators Toomey and JohnsonFedSmith Inc.No ratings yet
- Notice of Appeal by Donald J. Trump in People of The State of New York v. Trump, Et. Al. (Feb. 26, 2024)Document102 pagesNotice of Appeal by Donald J. Trump in People of The State of New York v. Trump, Et. Al. (Feb. 26, 2024)Daily Caller News FoundationNo ratings yet
- US V Rhodes - Letter Regarding Potential PenaltiesDocument4 pagesUS V Rhodes - Letter Regarding Potential PenaltiesAmerican GreatnessNo ratings yet
- Bverify ActDocument10 pagesBverify ActFox NewsNo ratings yet
- GOA To Senate Banking Committee On Secretary YellenDocument3 pagesGOA To Senate Banking Committee On Secretary YellenZerohedge JanitorNo ratings yet
- Coalition For TJ v. Fairfax County School Board, No. 23-170 (601 U.S. - , Feb. 20, 2024) (Cert. Denied)Document10 pagesCoalition For TJ v. Fairfax County School Board, No. 23-170 (601 U.S. - , Feb. 20, 2024) (Cert. Denied)Daily Caller News FoundationNo ratings yet
- Stephen Bannon Indictment Clerk Stamped 1Document9 pagesStephen Bannon Indictment Clerk Stamped 1New York PostNo ratings yet
- (DAILY CALLER OBTAINED) - 2022-04-27 Letter To DHS Re Disinformation Governance BoardDocument3 pages(DAILY CALLER OBTAINED) - 2022-04-27 Letter To DHS Re Disinformation Governance BoardHenry RodgersNo ratings yet
- (DAILY CALLER OBTAINED) - 2021-10-13 HJC GOP To Garland - DOJ Re Ethics QuestionsDocument4 pages(DAILY CALLER OBTAINED) - 2021-10-13 HJC GOP To Garland - DOJ Re Ethics QuestionsHenry RodgersNo ratings yet
- 2021-04-30 Request For Emergency Status Conference Re The Court - S SUA Sponte Release of Exhibit D9 To The PublicDocument33 pages2021-04-30 Request For Emergency Status Conference Re The Court - S SUA Sponte Release of Exhibit D9 To The PublicNicole Valdes67% (3)
- 2023 03 20 JDJ Bs JC To Bragg Re Trump InvestigationDocument4 pages2023 03 20 JDJ Bs JC To Bragg Re Trump InvestigationJulia Johnson100% (2)
- Wolfe Case - DOJ Response To Defense Sentencing MemoDocument20 pagesWolfe Case - DOJ Response To Defense Sentencing MemoThe Conservative Treehouse75% (4)
- Memorandum of Plea Agreement: Hunter Biden CaseDocument10 pagesMemorandum of Plea Agreement: Hunter Biden CaseKyle BeckerNo ratings yet
- Letter To AG Barr Special Counsel Hunter BidenDocument2 pagesLetter To AG Barr Special Counsel Hunter BidenFox News75% (4)
- Attempts to Impeach Donald Trump: Declassified Government Documents, Investigation of Russian Election Interference & Legislative ProceduresFrom EverandAttempts to Impeach Donald Trump: Declassified Government Documents, Investigation of Russian Election Interference & Legislative ProceduresNo ratings yet
- Voting Madness: A SAPIENT Being's Guide to Election Irregularities, Voter Fraud, Mail-In Ballots, HR1 and MoreFrom EverandVoting Madness: A SAPIENT Being's Guide to Election Irregularities, Voter Fraud, Mail-In Ballots, HR1 and MoreNo ratings yet
- BCBSA HOA Maternal Health DispairitiesDocument12 pagesBCBSA HOA Maternal Health DispairitiesBillNo ratings yet
- Obesity AND The Metabolic Syndrome: BY DR Anyamele IbuchimDocument49 pagesObesity AND The Metabolic Syndrome: BY DR Anyamele IbuchimPrincewill SmithNo ratings yet
- 1 s2.0 S0140673621005298 MainDocument1 page1 s2.0 S0140673621005298 MainMvelako StoryNo ratings yet
- Cardiovascular Morbidity, Diabetes and Cancer Risk Among Children and Adolescents With Severe ObesityDocument14 pagesCardiovascular Morbidity, Diabetes and Cancer Risk Among Children and Adolescents With Severe ObesityResti Eka SaputriNo ratings yet
- Kenaikan Risiko t2dm Pas PandemiDocument10 pagesKenaikan Risiko t2dm Pas PandemiINDAH KUSUMA NINGRUM 1No ratings yet
- National 2023 Israel Survey ToplineDocument12 pagesNational 2023 Israel Survey ToplineWashington Free BeaconNo ratings yet
- Tennessee Files ESG Lawsuit Against BlackRockDocument73 pagesTennessee Files ESG Lawsuit Against BlackRockWashington Free BeaconNo ratings yet
- FW SLSNLG NLG Board Statement On The Protest of The Federalist Society EventDocument4 pagesFW SLSNLG NLG Board Statement On The Protest of The Federalist Society EventWashington Free BeaconNo ratings yet
- GUEST VIEWPOINT - Baseball Fans Should Adopt New PastimeDocument3 pagesGUEST VIEWPOINT - Baseball Fans Should Adopt New PastimeWashington Free BeaconNo ratings yet
- D&I 07 Sept 22 TrainingDocument18 pagesD&I 07 Sept 22 TrainingWashington Free BeaconNo ratings yet
- New Venture Fund Document Preservation Notice RedactedDocument5 pagesNew Venture Fund Document Preservation Notice RedactedWashington Free BeaconNo ratings yet
- Rev NLPC Irs Compliaint Vs Warnock Oct 11 2022Document5 pagesRev NLPC Irs Compliaint Vs Warnock Oct 11 2022Washington Free Beacon100% (1)
- FW Aftermath of Thursdays EventsDocument2 pagesFW Aftermath of Thursdays EventsWashington Free BeaconNo ratings yet
- State & Local Elected Letter For Immigrant Inclusion - September 2021 - FINALDocument15 pagesState & Local Elected Letter For Immigrant Inclusion - September 2021 - FINALWashington Free BeaconNo ratings yet
- Coalition For TJ v. Fairfax County School Board Application To Vacate StayDocument37 pagesCoalition For TJ v. Fairfax County School Board Application To Vacate StayWashington Free BeaconNo ratings yet
- A Toolkit To Advance Racial Health Equity in Primary Care ImprovementDocument51 pagesA Toolkit To Advance Racial Health Equity in Primary Care ImprovementWashington Free BeaconNo ratings yet
- NIAID FOIA by White Coat Waste ProjectDocument81 pagesNIAID FOIA by White Coat Waste ProjectWashington Free BeaconNo ratings yet
- 2022-01 EPI Economist Survey (2) - EmbargoedDocument24 pages2022-01 EPI Economist Survey (2) - EmbargoedWashington Free BeaconNo ratings yet
- Justice For Sale LELDF ReportDocument17 pagesJustice For Sale LELDF ReportWashington Free Beacon100% (1)
- NAAG Fees Letter, Strategic UpdateDocument21 pagesNAAG Fees Letter, Strategic UpdateWashington Free BeaconNo ratings yet
- Uber v. AAA ComplaintDocument47 pagesUber v. AAA ComplaintWashington Free BeaconNo ratings yet
- The News Journal Tue Oct 24 1978Document1 pageThe News Journal Tue Oct 24 1978Washington Free BeaconNo ratings yet
- Biden v. Texas Immigration Orgs Amicus BriefDocument44 pagesBiden v. Texas Immigration Orgs Amicus BriefWashington Free BeaconNo ratings yet
- Break Up The Ninth Circuit Shapiro and HarveyDocument31 pagesBreak Up The Ninth Circuit Shapiro and HarveyWashington Free BeaconNo ratings yet
- Wilkofsky ECF 1 Complaint 04.11.22Document10 pagesWilkofsky ECF 1 Complaint 04.11.22Washington Free BeaconNo ratings yet
- Cassirer v. TBCF Opening BriefDocument49 pagesCassirer v. TBCF Opening BriefWashington Free BeaconNo ratings yet
- Coalition For TJ v. Fairfax County School Board Response in OppositionDocument347 pagesCoalition For TJ v. Fairfax County School Board Response in OppositionWashington Free BeaconNo ratings yet
- Davis v. Sharp ComplaintDocument30 pagesDavis v. Sharp ComplaintWashington Free BeaconNo ratings yet
- US v. Wiggins Opinion and Order On Request For ReleaseDocument21 pagesUS v. Wiggins Opinion and Order On Request For ReleaseWashington Free BeaconNo ratings yet
- US v. Dunlap Govt Brief Opposing Compassionate ReleaseDocument19 pagesUS v. Dunlap Govt Brief Opposing Compassionate ReleaseWashington Free BeaconNo ratings yet
- YLS Philly Statement Letter 040722Document23 pagesYLS Philly Statement Letter 040722Washington Free BeaconNo ratings yet
- US v. Dabney Govt Brief Opposing Pretrial ReleaseDocument44 pagesUS v. Dabney Govt Brief Opposing Pretrial ReleaseWashington Free BeaconNo ratings yet
- US v. Dunlap Opinion and Order Granting Supervised ReleaseDocument12 pagesUS v. Dunlap Opinion and Order Granting Supervised ReleaseWashington Free BeaconNo ratings yet
- Dresser Micro Corrector 2 (MC2) PTZ+Log: Volume Converter Model 197Document4 pagesDresser Micro Corrector 2 (MC2) PTZ+Log: Volume Converter Model 197Carlos Kcho AsportNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaMaulinaNo ratings yet
- The Education of Albert Einstein: Clayton A. GearhartDocument23 pagesThe Education of Albert Einstein: Clayton A. GearhartJudith Banabatac OreganoNo ratings yet
- Vo Dai Quang Semantics - Lectures in Broad OutlineDocument89 pagesVo Dai Quang Semantics - Lectures in Broad OutlineThu PhạmNo ratings yet
- Resume - Jessica Minch WebsiteDocument3 pagesResume - Jessica Minch Websiteapi-594661640No ratings yet
- September 2005 Limpkin Call Oklawaha Valley Audubon SocietyDocument4 pagesSeptember 2005 Limpkin Call Oklawaha Valley Audubon SocietyOklawaha Valley Audubon SocietyNo ratings yet
- Vision of Narayana Murthy For A Better IndiaDocument2 pagesVision of Narayana Murthy For A Better IndiadushyantNo ratings yet
- Epiphone Elite Catalog 2003Document12 pagesEpiphone Elite Catalog 2003dan_martin_21100% (1)
- IQN - Diploma in SCM Guidelines - Nov 2019Document43 pagesIQN - Diploma in SCM Guidelines - Nov 2019AlexanderDeFreitasNo ratings yet
- Please Quote This Reference Number in All Future CorrespondenceDocument2 pagesPlease Quote This Reference Number in All Future CorrespondenceSaipraveen PerumallaNo ratings yet
- Fundamentals Activities PrintDocument514 pagesFundamentals Activities PrintTOP NOTCHNo ratings yet
- TvtgurpsnewDocument94 pagesTvtgurpsnewKevin HutchingsNo ratings yet
- The Literary Formofthe QuranDocument10 pagesThe Literary Formofthe QuranTrina CanizoNo ratings yet
- Esip 2021-2024 LinabuisDocument107 pagesEsip 2021-2024 LinabuisJheryl Malapad Fortun-Guibelondo50% (2)
- Code of Ethics For Teacher As Legal Pillar To Improve Educational ProfessionalismDocument5 pagesCode of Ethics For Teacher As Legal Pillar To Improve Educational Professionalismjoycedacillo47No ratings yet
- Math 7 Post TestDocument2 pagesMath 7 Post TestDonabel Carios100% (3)
- Nitrogrn - Gate Valve Data SheetDocument2 pagesNitrogrn - Gate Valve Data SheetHabib ur rahmanNo ratings yet
- Singala SuttaDocument8 pagesSingala SuttaAshin Sucitta PkNo ratings yet
- Maintenance Instructions: AH-CraneDocument43 pagesMaintenance Instructions: AH-CraneRômulo França VelosoNo ratings yet
- ThermoFisherScientific 10K 20130227Document157 pagesThermoFisherScientific 10K 20130227siddk0312No ratings yet
- Paper 5 Examiner's Script: 3 Minutes (5 Minutes For Groups of Three)Document5 pagesPaper 5 Examiner's Script: 3 Minutes (5 Minutes For Groups of Three)IsaMar NuñezNo ratings yet
- Family Nursing Care Plan #2: Education of Their Child As Foreseeable CrisisDocument3 pagesFamily Nursing Care Plan #2: Education of Their Child As Foreseeable CrisisBakushido33% (9)
- The Impact of Organizational Justice On Employee's Job Satisfaction: The Malaysian Companies PerspectivesDocument8 pagesThe Impact of Organizational Justice On Employee's Job Satisfaction: The Malaysian Companies PerspectivesNaim NordinNo ratings yet
- Ckla g1 U4 TG EngageDocument248 pagesCkla g1 U4 TG EngageRivka ShareNo ratings yet
- Wallbox Supernova BrochureDocument8 pagesWallbox Supernova BrochuresaraNo ratings yet
- Ii Sem Case Study - I PartDocument9 pagesIi Sem Case Study - I PartVenkatesh100% (1)
- Hankel TransformDocument30 pagesHankel TransformMuhammad KamranNo ratings yet
- PPCoN 2169-2000Document113 pagesPPCoN 2169-2000Minh Hong PhamNo ratings yet
- CS 507 Mid TermDocument10 pagesCS 507 Mid TermMuddsir AmanNo ratings yet
- Dear Sirs and Madams Cover LetterDocument4 pagesDear Sirs and Madams Cover Letterc2yyr2c3100% (1)