Download as pdf or txt
You might also like
- Richie Spencer Qualitative Data Analysis For Applied Policy ResearchDocument13 pagesRichie Spencer Qualitative Data Analysis For Applied Policy ResearchAlex Richie100% (2)
- Humor in AdvertisingDocument18 pagesHumor in AdvertisingAlex RichieNo ratings yet
- Drug-Induced Diseases PDFDocument1,135 pagesDrug-Induced Diseases PDFGiang Vớ Vẩn100% (1)
- Severe Acute Respiratory Syndrome in Children: C D C P R ADocument7 pagesSevere Acute Respiratory Syndrome in Children: C D C P R Amelyta01_rahmisariNo ratings yet
- Trends of The Global, Regional, and National Incidence of Measles, Vaccine Coverage, and Risk Factors in 204 Countries From 1990 To 2019Document12 pagesTrends of The Global, Regional, and National Incidence of Measles, Vaccine Coverage, and Risk Factors in 204 Countries From 1990 To 2019Min YoojinNo ratings yet
- Precautionary Behavior in ResponseDocument7 pagesPrecautionary Behavior in ResponseMich PringNo ratings yet
- Update 28 Covid 19 What We Know May 2020Document18 pagesUpdate 28 Covid 19 What We Know May 2020Mohammed ImenksNo ratings yet
- Simulacion de Fakes News en EpidemiasDocument10 pagesSimulacion de Fakes News en EpidemiasjavenacostaNo ratings yet
- Attitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudyDocument7 pagesAttitude Anxiety and Behavior Practices Regarding COVID 19 Among University Students in Jordan.a Cross Sectional StudydauntlessNo ratings yet
- 1 - s2.0 - S1525505020307769 - Main With Cover Page v2Document8 pages1 - s2.0 - S1525505020307769 - Main With Cover Page v2nurhasanah nanaNo ratings yet
- Research in Social and Administrative PharmacyDocument6 pagesResearch in Social and Administrative PharmacyKaraengGalesongNo ratings yet
- Jurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesDocument6 pagesJurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesMusdaliva Tri Riskiani AlminNo ratings yet
- Psychological Impact of COVID-19 Pandemic in The Philippines PDFDocument13 pagesPsychological Impact of COVID-19 Pandemic in The Philippines PDFAndrea KamilleNo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author ManuscriptRizky Saraswati IndraputriNo ratings yet
- All-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisDocument12 pagesAll-Cause and Cause-Specific Mortality in Psoriasis: A Systematic Review and Meta-AnalysisRielz ThereaperzNo ratings yet
- Case-Control Study of Patient Characteristics, Knowledge of The COVID-19 Disease, Risk Behaviour and Mental State in Patients Visiting An Emergency Room With COVID-19 Symptoms in The NetherlandsDocument13 pagesCase-Control Study of Patient Characteristics, Knowledge of The COVID-19 Disease, Risk Behaviour and Mental State in Patients Visiting An Emergency Room With COVID-19 Symptoms in The NetherlandsRevi RidayantiNo ratings yet
- Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19Document10 pagesAssessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19andris mejia alvarezNo ratings yet
- Risk Factors For HIV and STI Among Female Sex Workers in A High HIV Prevalent Region of EcuadorDocument13 pagesRisk Factors For HIV and STI Among Female Sex Workers in A High HIV Prevalent Region of EcuadorFrans LandiNo ratings yet
- Chapter 7Document34 pagesChapter 7Regina MunaamadaniNo ratings yet
- Maurice (2015)Document1 pageMaurice (2015)SammerNo ratings yet
- TJPS 17 242Document7 pagesTJPS 17 242AVITA TRISTA NINGRUMNo ratings yet
- Medical Students and COVID-19: Knowledge, Attitudes, and Precautionary Measures. A Descriptive Study From JordanDocument9 pagesMedical Students and COVID-19: Knowledge, Attitudes, and Precautionary Measures. A Descriptive Study From JordanAllison Velasquez MirandaNo ratings yet
- 1 s2.0 S1198743X14604614 MainDocument5 pages1 s2.0 S1198743X14604614 Mained_mariachiNo ratings yet
- Koodak PDFDocument9 pagesKoodak PDFHugoMarcelo77No ratings yet
- Article in Press: Journal of Infection and Public HealthDocument5 pagesArticle in Press: Journal of Infection and Public HealthabganNo ratings yet
- 02 Perceptions of Risks and Impacts of COVID-19 Among The Public in EthiopiaDocument12 pages02 Perceptions of Risks and Impacts of COVID-19 Among The Public in Ethiopiasami peterNo ratings yet
- Dengue in Latin AmericaDocument19 pagesDengue in Latin AmericaCarolina Neciosup TullumeNo ratings yet
- Respiratory Distress in PediatricsDocument6 pagesRespiratory Distress in Pediatricsthirunagari praveenNo ratings yet
- Honarvar2020 Article KnowledgeAttitudesRiskPerceptiDocument9 pagesHonarvar2020 Article KnowledgeAttitudesRiskPerceptiYuni MonesaNo ratings yet
- Species Distribution Models Are Inappropriate For COVID-19: CommentDocument2 pagesSpecies Distribution Models Are Inappropriate For COVID-19: CommenthermalfaroncalNo ratings yet
- Pathophysiology of Covid19Document6 pagesPathophysiology of Covid19KHOUNo ratings yet
- Lived Experiences Wiith Covid - 19Document9 pagesLived Experiences Wiith Covid - 19Freddy JunsayNo ratings yet
- Review of Related LiteratureDocument16 pagesReview of Related LiteratureHavier EsparagueraNo ratings yet
- Wang, C., Horby, P. W., Hayden, F. G., & Gao, G. F. (2020) - A Novel Coronavirus Outbreak of Global Health Concern. The Lancet, 395 (10223), 470-473.Document5 pagesWang, C., Horby, P. W., Hayden, F. G., & Gao, G. F. (2020) - A Novel Coronavirus Outbreak of Global Health Concern. The Lancet, 395 (10223), 470-473.Macky AlihuddinNo ratings yet
- 1 s2.0 S152169422100005X MainDocument10 pages1 s2.0 S152169422100005X MainnordonkNo ratings yet
- Byu Covid Masks AbbottDocument11 pagesByu Covid Masks AbbottAlyssa RobertsNo ratings yet
- Clinical Course and Mortality Risk of Severe COVID-19: CommentDocument2 pagesClinical Course and Mortality Risk of Severe COVID-19: CommentmizraimNo ratings yet
- Covid 20 PDFDocument2 pagesCovid 20 PDFmizraimNo ratings yet
- A Novel Coronavirus Outbreak of Global Health Concern: CommentDocument8 pagesA Novel Coronavirus Outbreak of Global Health Concern: CommentMuhammad Adil BaigNo ratings yet
- Jurnal English Covid.3Document3 pagesJurnal English Covid.3Dina AryaniNo ratings yet
- COVID-19 in HIV: A Review of Published Case ReportsDocument11 pagesCOVID-19 in HIV: A Review of Published Case Reports6ixSideCreate MNo ratings yet
- A Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirDocument11 pagesA Study On Impact of COVID-19 Lockdown On Psychological Health, Economy and Social Life of People in KashmirAnnuNo ratings yet
- Who Severe Malaria Tmih Supplement 2014Document125 pagesWho Severe Malaria Tmih Supplement 2014RizkaNNatsirNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesndutaNo ratings yet
- Dengue KAPDocument9 pagesDengue KAPElinNo ratings yet
- High Risk-Low Risk Stroke SudanDocument12 pagesHigh Risk-Low Risk Stroke SudanAhmed BadawyNo ratings yet
- ISIDOG+guidelines+for+COVID19 in PregnancyDocument32 pagesISIDOG+guidelines+for+COVID19 in PregnancyWawan Febri RamdaniNo ratings yet
- Public Stroke KSADocument12 pagesPublic Stroke KSAAhmed BadawyNo ratings yet
- Knowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointDocument6 pagesKnowledge Attitude and Risk Perception of COVID 19 in Rural Ghana A ViewpointAthenaeum Scientific PublishersNo ratings yet
- Pone 0236918Document13 pagesPone 0236918MegbaruNo ratings yet
- Rose Prevention Paradox (Presentation Slide)Document10 pagesRose Prevention Paradox (Presentation Slide)Teh NuraqilahNo ratings yet
- Coronavirus Disease 2019 and Children What Pediatric Health Care Clinicians Need To KnowDocument2 pagesCoronavirus Disease 2019 and Children What Pediatric Health Care Clinicians Need To KnowTor JaNo ratings yet
- Hesitancy Towards A COVID-19 Vaccine and Prospects For Herd ImmunityDocument51 pagesHesitancy Towards A COVID-19 Vaccine and Prospects For Herd ImmunityA009Karin Kurniati NurfatmahNo ratings yet
- Mirzaei2020 Article COVID-19AmongPeopleLivingWithHDocument8 pagesMirzaei2020 Article COVID-19AmongPeopleLivingWithHyasiNo ratings yet
- Children 'S Heart and COVID-19: Up-To-Date Evidence in The Form of A Systematic ReviewDocument9 pagesChildren 'S Heart and COVID-19: Up-To-Date Evidence in The Form of A Systematic ReviewArif Nurhadi AtmokoNo ratings yet
- Covid 19Document7 pagesCovid 19Saurav KumarNo ratings yet
- AsdsfDocument6 pagesAsdsfvirta andhikaNo ratings yet
- A Pharmacology-Based Comprehensive Review On Medicinal PlantsDocument14 pagesA Pharmacology-Based Comprehensive Review On Medicinal PlantsissamebenNo ratings yet
- Coronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentFrom EverandCoronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentRating: 5 out of 5 stars5/5 (1)
- will it ever go away?: Practical Answers to Your Questions About COVID-19From Everandwill it ever go away?: Practical Answers to Your Questions About COVID-19No ratings yet
- A Multidisciplinary Approach To Talent Identification in SoccerDocument9 pagesA Multidisciplinary Approach To Talent Identification in SoccerAlex RichieNo ratings yet
- Young and Biased Children's Perceptions of Overweight PeersDocument15 pagesYoung and Biased Children's Perceptions of Overweight PeersAlex RichieNo ratings yet
- Ojanen2013Document17 pagesOjanen2013Alex RichieNo ratings yet
- Why Do I Study and What Do I Want To Achieve by Studying Understanding The Reasons and The Aims of Student EngagementDocument18 pagesWhy Do I Study and What Do I Want To Achieve by Studying Understanding The Reasons and The Aims of Student EngagementAlex RichieNo ratings yet
- NU Ijerph-19-09413Document25 pagesNU Ijerph-19-09413Alex RichieNo ratings yet
- Psysical Attractivened As Advertisement ToolDocument8 pagesPsysical Attractivened As Advertisement ToolAlex RichieNo ratings yet
- Personality and Individual Differences: Karin Sobocko, John M. ZelenskiDocument6 pagesPersonality and Individual Differences: Karin Sobocko, John M. ZelenskiAlex RichieNo ratings yet
- Self-Affirmation Theory and The Science of Well-Being PDFDocument19 pagesSelf-Affirmation Theory and The Science of Well-Being PDFAlex RichieNo ratings yet
- The Highly Sensitive Person: Stress and Physical Symptom ReportsDocument8 pagesThe Highly Sensitive Person: Stress and Physical Symptom ReportsAlex RichieNo ratings yet
- Consumer Sketicism AdvertisingDocument28 pagesConsumer Sketicism AdvertisingAlex RichieNo ratings yet
- Psysical Attractivenes and Personality in AdvertismentDocument7 pagesPsysical Attractivenes and Personality in AdvertismentAlex RichieNo ratings yet
- Experimental Manipulations of Self-Affirmation REVIEW PDFDocument67 pagesExperimental Manipulations of Self-Affirmation REVIEW PDFAlex RichieNo ratings yet
- Humor in Advertising ReviewDocument9 pagesHumor in Advertising ReviewAlex RichieNo ratings yet
- Alexithymia Body IlusionsDocument8 pagesAlexithymia Body IlusionsAlex RichieNo ratings yet
- DRRR VocabularyDocument2 pagesDRRR VocabularygailNo ratings yet
- Cheadle Area Committee 15th March 2016Document176 pagesCheadle Area Committee 15th March 2016IainRobertsNo ratings yet
- Ethics in Healthcare Setting (Therapy)Document10 pagesEthics in Healthcare Setting (Therapy)Milcah ShabanjiNo ratings yet
- Jetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsDocument61 pagesJetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsShalimar BasmanNo ratings yet
- Vehicle Inspection Checklist PDFDocument9 pagesVehicle Inspection Checklist PDFSampahNo ratings yet
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- Genetics and EugenicsDocument518 pagesGenetics and EugenicsTapuwa ChizunzaNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Inquiries, Investigation, and Immersion: Quarter 2 Module 2 - Lesson 3Document12 pagesInquiries, Investigation, and Immersion: Quarter 2 Module 2 - Lesson 3Max TofuNo ratings yet
- Unit 10-lớp 7-Phiếu 04-BaiLamDocument3 pagesUnit 10-lớp 7-Phiếu 04-BaiLamAmong Us ByNo ratings yet
- SZ Sales ProgramDocument28 pagesSZ Sales ProgramrossifrancescoNo ratings yet
- Psychosexual Theory - Sigmund Freud: Neurologist PsychoanalysisDocument4 pagesPsychosexual Theory - Sigmund Freud: Neurologist PsychoanalysisEmmajean'Ricky GustiloNo ratings yet
- Cells Teachers Guide Discovery EducationDocument38 pagesCells Teachers Guide Discovery EducationKari Kristine Hoskins BarreraNo ratings yet
- Sore ThroatDocument10 pagesSore Throatapi-551073862No ratings yet
- Tecan Sunrise Absorbance Reader Analyser - User ManualDocument74 pagesTecan Sunrise Absorbance Reader Analyser - User Manualomer oartbNo ratings yet
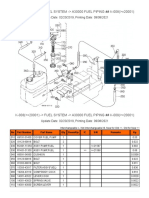
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Tle CSS Mod5Document2 pagesTle CSS Mod5john kingNo ratings yet
- BiochemistryDocument68 pagesBiochemistry20AR018 HARIHARA SUBRAMANIANNo ratings yet
- Copper (RJ-45) SFP: Technical SpecificationsDocument1 pageCopper (RJ-45) SFP: Technical SpecificationsDanielLopezNo ratings yet
- Essay C DraftDocument7 pagesEssay C Draftapi-242837115No ratings yet
- Appendix 66 Rpci Updated Ues JehanDocument58 pagesAppendix 66 Rpci Updated Ues JehanOmar Gulam JrNo ratings yet
- Infinix Hot 10: Best Gaming Smartphone Under 20k in Nepal, LaunchedDocument7 pagesInfinix Hot 10: Best Gaming Smartphone Under 20k in Nepal, LaunchedSulavNo ratings yet
- ISC BiotechnologyDocument6 pagesISC BiotechnologySamikshaNo ratings yet
- Luserne Tree InformationDocument26 pagesLuserne Tree Informationpierre van wykNo ratings yet
- Code of Sports EthicsDocument4 pagesCode of Sports EthicsRadu MiclausNo ratings yet
- Activated Carbon From BambooDocument19 pagesActivated Carbon From BambooErik WeeksNo ratings yet
- Printable Cosmetology LawbookDocument42 pagesPrintable Cosmetology LawbookCaro TNo ratings yet
- Supreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsDocument2 pagesSupreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsAdv Akshay KshirsagarNo ratings yet