Download as pdf or txt
You might also like
- Test Bank For Davis Advantage For Fundamentals of Nursing 2 Volume Set 4th Edition Judith M Wilkinson Leslie S Treas Karen L Barnett Mable H SmithDocument30 pagesTest Bank For Davis Advantage For Fundamentals of Nursing 2 Volume Set 4th Edition Judith M Wilkinson Leslie S Treas Karen L Barnett Mable H SmithElsie Dixon100% (37)
- Pharmacology For Canadian Health Care Practice, 3rd Canadian Edition: Chapter 03 - Legal and Ethical Considerations Chapter SummaryDocument4 pagesPharmacology For Canadian Health Care Practice, 3rd Canadian Edition: Chapter 03 - Legal and Ethical Considerations Chapter SummaryNadine MahadeoNo ratings yet
- Case Group Work #2 CHAPTER 6 Learning Exercise 6.4 L&M 03-03-2021 SituationDocument3 pagesCase Group Work #2 CHAPTER 6 Learning Exercise 6.4 L&M 03-03-2021 SituationZunnel CortesNo ratings yet
- Utilization Management: Prepared By: Dr. Alber PaulesDocument50 pagesUtilization Management: Prepared By: Dr. Alber Paulesmonir61No ratings yet
- Hospital Management SystemDocument57 pagesHospital Management SystemPuneet Gupta94% (17)
- SMEDA Private HospitalDocument25 pagesSMEDA Private HospitalKhan Ab75% (4)
- Care Enhancement Qualities of Health Workers in Community SettingDocument3 pagesCare Enhancement Qualities of Health Workers in Community SettingJon Eric74% (19)
- Letter From Svante Myrick To Gov. Andrew CuomoDocument1 pageLetter From Svante Myrick To Gov. Andrew CuomoKelsey O'ConnorNo ratings yet
- NARAYANA Project WorkDocument102 pagesNARAYANA Project Worknaveen chitiralaNo ratings yet
- MRD/ Clinical Information UnitDocument21 pagesMRD/ Clinical Information UnitMohd SalahuddinNo ratings yet
- Referral Systems For HEWDocument39 pagesReferral Systems For HEWmohammed AminNo ratings yet
- Applying Lean Principles To A Continuing CareDocument5 pagesApplying Lean Principles To A Continuing CareEva VillalbaNo ratings yet
- Kel 2 - Hospital DischargeDocument18 pagesKel 2 - Hospital DischargeFeby KartikasariNo ratings yet
- Discharge Planning Booklet ICN908184Document28 pagesDischarge Planning Booklet ICN908184Chelz Niia DheyvanNo ratings yet
- Discharge Planning ProtocolDocument11 pagesDischarge Planning Protocolatinkut eteneshNo ratings yet
- Access To Care ACC and PatientCentered Care PCCDocument44 pagesAccess To Care ACC and PatientCentered Care PCClucky.positivethinkNo ratings yet
- Final ACC 2021Document67 pagesFinal ACC 2021Karien UysNo ratings yet
- BIK Discharge SummaryDocument11 pagesBIK Discharge SummaryBetarie Anum AlmiraNo ratings yet
- DHA Part B OutpatientsDocument37 pagesDHA Part B OutpatientsMartin Rilloraza Jr.No ratings yet
- APH Surgical Service ProtocolDocument31 pagesAPH Surgical Service Protocolsami ketema50% (2)
- Presentation 1Document13 pagesPresentation 1RatulNo ratings yet
- OBM752 Unit 4 21.10.22Document26 pagesOBM752 Unit 4 21.10.22tempnew85No ratings yet
- Outpatient Services Implementation Standard: 1. PurposeDocument20 pagesOutpatient Services Implementation Standard: 1. PurposeReginaAstariTjoegitoNo ratings yet
- Chapter 4Document21 pagesChapter 4Luis DetriniadNo ratings yet
- Medical Staff Doctors - Hospital Discharge Action Cards RevisedDocument1 pageMedical Staff Doctors - Hospital Discharge Action Cards RevisedLuizaNo ratings yet
- Admission and Discharge ProtocolDocument38 pagesAdmission and Discharge Protocolatinkut eteneshNo ratings yet
- G15 ED DesignDocument25 pagesG15 ED DesignIrrum RazaNo ratings yet
- Patient Admittance and Care Process FlowchartDocument9 pagesPatient Admittance and Care Process FlowchartSammy ChegeNo ratings yet
- Medical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviDocument61 pagesMedical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviRashid AyubiNo ratings yet
- Hospital Admission To Discharge 13 3 12 OkDocument3 pagesHospital Admission To Discharge 13 3 12 OkHarry Wahyudhy UtamaNo ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- How To Conduct A Post-Discharge Follow-Up Phone Call 4.15.11Document49 pagesHow To Conduct A Post-Discharge Follow-Up Phone Call 4.15.11Arafat FaisalNo ratings yet
- Discharge Planning and ReferralDocument4 pagesDischarge Planning and ReferralNur Ighwana SariNo ratings yet
- SNF Hospital Collaboration White Paper 6.18.09Document2 pagesSNF Hospital Collaboration White Paper 6.18.09kudo01No ratings yet
- WEEK 3. Quality and Safe Management in The ERDocument19 pagesWEEK 3. Quality and Safe Management in The ERAira Espleguira100% (1)
- Outpatient DepartmentDocument3 pagesOutpatient DepartmentSneha ChowdhuryNo ratings yet
- Health Centers Referral ProtocolDocument13 pagesHealth Centers Referral ProtocolFikerte ZerihunNo ratings yet
- Part B - Health Facility Briefing & Design 260 Medical Imaging Unit - GeneralDocument26 pagesPart B - Health Facility Briefing & Design 260 Medical Imaging Unit - GeneralAdrian Fernando Del Castillo VelascoNo ratings yet
- Hospital Admission and DischargeDocument21 pagesHospital Admission and DischargeYogesh ChandraNo ratings yet
- OPDSerDocument39 pagesOPDSerDAD SHOTSNo ratings yet
- The Handbook For Hospital Planning and DesigningDocument24 pagesThe Handbook For Hospital Planning and Designingarch.anupNo ratings yet
- Utilization ManagementDocument7 pagesUtilization ManagementCommunityBridgesNo ratings yet
- Triage EnvironmentDocument2 pagesTriage EnvironmentmaithamNo ratings yet
- Accreditation Has Been Defined AsDocument15 pagesAccreditation Has Been Defined AsgayathrivdNo ratings yet
- Admissions and Discharge: GuidelinesDocument26 pagesAdmissions and Discharge: GuidelinesIshaan TalrejaNo ratings yet
- 17 Admission APP MED 001Document8 pages17 Admission APP MED 001HAMMYER ALROKHAMINo ratings yet
- An SAP ERP For The Hospital: ObjectiveDocument11 pagesAn SAP ERP For The Hospital: ObjectivesvewNo ratings yet
- IHFG Part B Renal Dialysis UnitDocument18 pagesIHFG Part B Renal Dialysis Unitmorton1472No ratings yet
- 13 ClinicalsummariesDocument2 pages13 Clinicalsummariesapi-101814919No ratings yet
- The Process of Discharge PlanningDocument6 pagesThe Process of Discharge Planningprabha100% (1)
- Textbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosFrom EverandTextbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosNo ratings yet
- Ahmed Linkage PresentationDocument15 pagesAhmed Linkage PresentationKRUSU ISAACNo ratings yet
- JCI Accreditation Presentation 4Document53 pagesJCI Accreditation Presentation 4Osama MarzoukNo ratings yet
- Hospital Support ServicesDocument7 pagesHospital Support ServicesAbhay DhawaleNo ratings yet
- Hospital ManagementDocument34 pagesHospital ManagementNavin JethwaniNo ratings yet
- Surgical Self-Assessment ChecklistDocument8 pagesSurgical Self-Assessment ChecklistJyoti KumarNo ratings yet
- Don't Lose PatientsDocument9 pagesDon't Lose PatientsdrustagiNo ratings yet
- Hospital ManagementDocument29 pagesHospital ManagementRohit YadavNo ratings yet
- Final Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphDocument11 pagesFinal Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphwendryNo ratings yet
- Mountain View Community Hospital: Goals and Critical Success FactorsDocument5 pagesMountain View Community Hospital: Goals and Critical Success Factorsfadicool007No ratings yet
- Lesson 9 HIS Hospital Information SystemDocument36 pagesLesson 9 HIS Hospital Information SystemKauline Joseph C. BrionesNo ratings yet
- Training MaterialDocument38 pagesTraining Materialvbhndari13No ratings yet
- Department: Col Zulfiquer Ahmed Amin Armed Forces Medical Institute (AFMI)Document64 pagesDepartment: Col Zulfiquer Ahmed Amin Armed Forces Medical Institute (AFMI)Gia 2k17No ratings yet
- Discharge Process SynopsisDocument7 pagesDischarge Process Synopsisdrbhavya250% (1)
- NABH Guidelines PDFDocument71 pagesNABH Guidelines PDFAshish kumarNo ratings yet
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
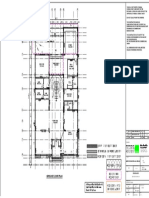
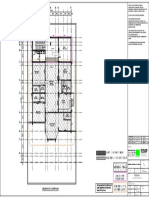
- A B C D E F C': Ground Floor PlanDocument1 pageA B C D E F C': Ground Floor Planchandan guptaNo ratings yet
- A B C D E F C': Schedule of Doors & WindowsDocument1 pageA B C D E F C': Schedule of Doors & Windowschandan guptaNo ratings yet
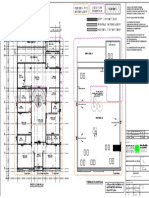
- A B C D E F C': First Floor Plan Terrace Floor PlanDocument1 pageA B C D E F C': First Floor Plan Terrace Floor Planchandan guptaNo ratings yet
- A B C D E F C': Leveling - 2 Floor PlanDocument1 pageA B C D E F C': Leveling - 2 Floor Planchandan guptaNo ratings yet
- Mechanical Engineer (FIRE ALARM & FIRE FIGHTING)Document1 pageMechanical Engineer (FIRE ALARM & FIRE FIGHTING)chandan guptaNo ratings yet
- Pharmacist's Role in The System of Palliative and Hospice Care in Ukraine and PolandDocument74 pagesPharmacist's Role in The System of Palliative and Hospice Care in Ukraine and PolandСофія ШунькінаNo ratings yet
- SAPDocument3 pagesSAPMs.cimnasunny MNo ratings yet
- Annual Report FinalDocument232 pagesAnnual Report FinalAshvini GoelNo ratings yet
- Rybelsus DataDocument252 pagesRybelsus Datasanskargaglani03No ratings yet
- The Importance of Antenatal CareDocument4 pagesThe Importance of Antenatal CareChennulNo ratings yet
- School Health ComponentDocument29 pagesSchool Health ComponentKim SorianoNo ratings yet
- WHO Guideline For Management of Chronic Low Back PainDocument274 pagesWHO Guideline For Management of Chronic Low Back PainRamji Rao RamijinniNo ratings yet
- IMPORTANT Delivering Better Oral Health 2021Document198 pagesIMPORTANT Delivering Better Oral Health 2021lindajenhaniNo ratings yet
- Resh ED 211221Document15 pagesResh ED 211221dkhatri01No ratings yet
- 81780-Article Text-195418-1-10-20120928Document5 pages81780-Article Text-195418-1-10-20120928Grace BasseyNo ratings yet
- Lesson Exemplar Health10 Luna San JuanDocument14 pagesLesson Exemplar Health10 Luna San JuanGiezelle LeopandoNo ratings yet
- Summary of Reviewed Articles-FinalDocument5 pagesSummary of Reviewed Articles-FinalMishuNo ratings yet
- Libreng Gamot For AllDocument6 pagesLibreng Gamot For AllDesiree Angelique RebonquinNo ratings yet
- Drug Tab PsychDocument10 pagesDrug Tab PsychtabiNo ratings yet
- ASHP Peds GuidelinesDocument3 pagesASHP Peds Guidelinesfineboy74No ratings yet
- Medtech Laws ReviewerDocument23 pagesMedtech Laws ReviewerAndrea Faye MONTERONANo ratings yet
- Live Music Promotes Positive Behaviours inDocument9 pagesLive Music Promotes Positive Behaviours inSaul MorenoNo ratings yet
- PDF Behavioral and Mental Health Care Policy and Practice A Biopsychosocial Perspective Cynthia Moniz Ebook Full ChapterDocument53 pagesPDF Behavioral and Mental Health Care Policy and Practice A Biopsychosocial Perspective Cynthia Moniz Ebook Full Chapterkristi.leroy709100% (3)
- An Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Document8 pagesAn Historical Perspective On Principles of Osteopathy - Jane Eliza Stark. 2013Adolfo Esteban Soto MartinezNo ratings yet
- 12 Core FunctionsDocument17 pages12 Core FunctionsAcep RanalNo ratings yet
- Pharmacy Management (PSW 404) BU 2023Document77 pagesPharmacy Management (PSW 404) BU 2023Emmanuella OffiongNo ratings yet
- PDF Transcript - Dr. A. P. J. Abdul Kalam-2Document6 pagesPDF Transcript - Dr. A. P. J. Abdul Kalam-2PSNo ratings yet
- 7 Best Natural Antibiotics - Uses, Evidence, and EffectivenessDocument10 pages7 Best Natural Antibiotics - Uses, Evidence, and Effectivenessbaek2mo340No ratings yet
- Sample FMEA: Comparison of Five Medication Dispensing ScenariosDocument19 pagesSample FMEA: Comparison of Five Medication Dispensing Scenarioscpears56No ratings yet