Download as pdf or txt
You might also like
- Rhetorical Analysis EssayDocument5 pagesRhetorical Analysis Essayapi-320095543No ratings yet
- Anemia Concept Mapping. Group 1Document82 pagesAnemia Concept Mapping. Group 1Giselle EstoquiaNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- COVID Clinical Management 14012022Document1 pageCOVID Clinical Management 14012022Naina DesaiNo ratings yet
- COVID Management 17th January 2022 DR Suvrankar Datta AIIMSDocument1 pageCOVID Management 17th January 2022 DR Suvrankar Datta AIIMSWhiteNo ratings yet
- Treatment Protocol Covid-19Document4 pagesTreatment Protocol Covid-19Shiv singhNo ratings yet
- Family Medicine Case FilesDocument44 pagesFamily Medicine Case FilesTazan VoNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- KEM Protocols - Hypertensive Emergency (Dr. Pritha)Document3 pagesKEM Protocols - Hypertensive Emergency (Dr. Pritha)Sonu AntonyNo ratings yet
- Resource ViewDocument54 pagesResource ViewHamza AdeelNo ratings yet
- Asma 1Document8 pagesAsma 1punkgatitNo ratings yet
- COVID MX BsmmuDocument2 pagesCOVID MX BsmmuNuhiat NahreenNo ratings yet
- CopdDocument16 pagesCopdHot MathNo ratings yet
- Laboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalDocument2 pagesLaboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalSujoyDeNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- PcolDocument17 pagesPcolThea JulianaNo ratings yet
- Treatment Protocol Covid EnglishDocument3 pagesTreatment Protocol Covid EnglishIchigo SnijdersNo ratings yet
- Icu Guidelines - 024219Document6 pagesIcu Guidelines - 024219M Hammad AshrafNo ratings yet
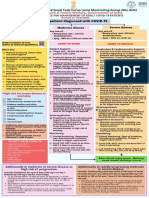
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Case 1: Health Maintenance in GeneralDocument44 pagesCase 1: Health Maintenance in GeneralJoshuaNo ratings yet
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Management of Acute Severe Asthma in PediatricsDocument53 pagesManagement of Acute Severe Asthma in PediatricsAmit AnandNo ratings yet
- Allergy and Immunology 2023 FINALDocument18 pagesAllergy and Immunology 2023 FINALBelinda ELISHANo ratings yet
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliNo ratings yet
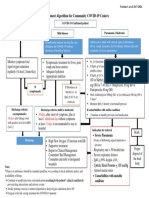
- Management Algorithm For Community COVID-19 CentersDocument1 pageManagement Algorithm For Community COVID-19 CentersSi Thu LwinNo ratings yet
- FINAL COVID19 1 April 2021Document14 pagesFINAL COVID19 1 April 2021Wleed KhledNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- Severe Sepsis&Septic Shock in Pediatrics.: Abdel Razzaq Abu Mayaleh, MDDocument27 pagesSevere Sepsis&Septic Shock in Pediatrics.: Abdel Razzaq Abu Mayaleh, MDlotskiNo ratings yet
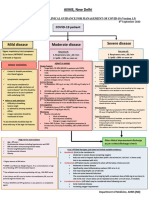
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarNo ratings yet
- Bronchial Asthma (1) SKDocument24 pagesBronchial Asthma (1) SKSafoora RafeeqNo ratings yet
- Covid-19 Protocol Severity and ManagementDocument4 pagesCovid-19 Protocol Severity and ManagementMardy DeponaNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- Acute Asthma - Care in The Emergency DepartmentDocument5 pagesAcute Asthma - Care in The Emergency DepartmentTanitNo ratings yet
- ANAESTHESIA For Copd AsthmaDocument20 pagesANAESTHESIA For Copd AsthmashikhaNo ratings yet
- Bronchial Asthma!: A C E S G V CDocument10 pagesBronchial Asthma!: A C E S G V CAmalNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- BCCA AB in Febrile Neutropenia GuidelinesDocument2 pagesBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieNo ratings yet
- MIS C Algorithim Version 2Document8 pagesMIS C Algorithim Version 2Saima UmairNo ratings yet
- Ace FinalDocument11 pagesAce FinalJude Andrian CasugayNo ratings yet
- Drugs For Treatment of Bronchial Asthma: DR Sanjay Junior Resident Department of Pharmacology Ims-BhuDocument19 pagesDrugs For Treatment of Bronchial Asthma: DR Sanjay Junior Resident Department of Pharmacology Ims-BhuBisweswar OjhaNo ratings yet
- AIIMS COVID Algorithm 1.5-1 PDFDocument1 pageAIIMS COVID Algorithm 1.5-1 PDFAnutosh BhaskarNo ratings yet
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDocument3 pagesComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNo ratings yet
- CPAMSDocument7 pagesCPAMSDominic chuaNo ratings yet
- Lecture 6Document5 pagesLecture 6Grafu Andreea AlexandraNo ratings yet
- AIIMS COVID Doc 1.6.1-1Document1 pageAIIMS COVID Doc 1.6.1-1mbhangaleNo ratings yet
- REVISED COVID-19 TREATMENT PROTOCOL - Version 3Document17 pagesREVISED COVID-19 TREATMENT PROTOCOL - Version 3abhishekNo ratings yet
- Status Asthmaticus: Triwahju AstutiDocument41 pagesStatus Asthmaticus: Triwahju AstutirianiNo ratings yet
- Common Pediatric Emergencies - A2Document46 pagesCommon Pediatric Emergencies - A2Ahmad JustNo ratings yet
- Asthma 1Document79 pagesAsthma 1DanishMandiNo ratings yet
- Referat Sepsis Dan ARDS - Lea SichiliaDocument24 pagesReferat Sepsis Dan ARDS - Lea SichiliaLea SichiliaNo ratings yet
- JLN Nafas 2 PDFDocument27 pagesJLN Nafas 2 PDFDiga AnaNo ratings yet
- Acute Severe Asthma Critical Care Management: Lokesh Tiwari Aiims PatnaDocument53 pagesAcute Severe Asthma Critical Care Management: Lokesh Tiwari Aiims PatnaYohana SepthiyaNo ratings yet
- Asthma Harrisons ClubDocument84 pagesAsthma Harrisons ClubLady AngodNo ratings yet
- Etiology & Triggers: AsthmaDocument6 pagesEtiology & Triggers: AsthmaNichole CollinsNo ratings yet
- Bronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387Document25 pagesBronchial Asthma: Mariam Lwasa Naluwugge Afrah 215-083011-07387NinaNo ratings yet
- High-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningDocument3 pagesHigh-Flow Nasal Cannula-Protocol For Initiation, Titration and WeaningMahmoud khedrNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Fast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseFrom EverandFast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Plantzichi80% (5)
- A Study On The Relationship Between Sport and AggressionDocument16 pagesA Study On The Relationship Between Sport and AggressionNur SyuhadahNo ratings yet
- ENS Guide To Diagnosis & Management (v2 - 09.2016)Document37 pagesENS Guide To Diagnosis & Management (v2 - 09.2016)Renato Mondani0% (1)
- Change'your'water.' ' ' ' ''Change'your'life'222': Some Beneficial Uses of Kangen WaterDocument1 pageChange'your'water.' ' ' ' ''Change'your'life'222': Some Beneficial Uses of Kangen WaterGyaan WallahNo ratings yet
- NEW SOP - ReviewedDocument2 pagesNEW SOP - ReviewedAparna RoyNo ratings yet
- Public Health Surveillance & ScreeningDocument58 pagesPublic Health Surveillance & ScreeningKonjit MitikuNo ratings yet
- Delsa Hea WD HWP (2021) 4Document140 pagesDelsa Hea WD HWP (2021) 4ghoudzNo ratings yet
- Documentation Asset Doc Loc 3417883 DeckingDocument9 pagesDocumentation Asset Doc Loc 3417883 DeckingCristiano SilvaNo ratings yet
- Daftar Pustaka Makalah Tahap IDocument2 pagesDaftar Pustaka Makalah Tahap IAulina Refri RahmiNo ratings yet
- Ross, C. (2020) - PTSD As A Future-Oriented Survival Strategy. Richardson The Colin A. Ross Institute For Psychological TraumaDocument5 pagesRoss, C. (2020) - PTSD As A Future-Oriented Survival Strategy. Richardson The Colin A. Ross Institute For Psychological TraumaEraNo ratings yet
- Remunerasi RSDocument39 pagesRemunerasi RSalfanNo ratings yet
- (Oxford Handbooks of Political Science) R. A. W. Rhodes, Sarah A. Binder, Bert A. Rockman-Handbook Political Institutions-Oxford University Press, USA (2006)Document456 pages(Oxford Handbooks of Political Science) R. A. W. Rhodes, Sarah A. Binder, Bert A. Rockman-Handbook Political Institutions-Oxford University Press, USA (2006)Perico de los Palotes100% (2)
- A Generation of Couch Potatoes Lesson Plan PDFDocument2 pagesA Generation of Couch Potatoes Lesson Plan PDFFBNo ratings yet
- Outline of Dissertation On ObesityDocument16 pagesOutline of Dissertation On ObesityLavarn PillaiNo ratings yet
- Bridging The Care GapDocument50 pagesBridging The Care GapChetna AroraNo ratings yet
- Juvenile Justice Reform/Restoring Arkansas Families BillDocument12 pagesJuvenile Justice Reform/Restoring Arkansas Families BillMarine GlisovicNo ratings yet
- Injury Statistics SheetDocument4 pagesInjury Statistics SheetEslam IsmaeelNo ratings yet
- Hostage Negotiation Semi FinalDocument10 pagesHostage Negotiation Semi Finalarianne ayalaNo ratings yet
- Clinical Significance Blood Group AntibodiesDocument8 pagesClinical Significance Blood Group AntibodiesSudeep RathoreNo ratings yet
- Nutrition of Blueberry 10-7-11 MO StrikDocument60 pagesNutrition of Blueberry 10-7-11 MO StrikJesús Miguel Maguiña EspinozaNo ratings yet
- EHS 085 General Security Procedure For Manufacturing Area SampleDocument3 pagesEHS 085 General Security Procedure For Manufacturing Area Samplerozario100% (1)
- Method Statement - MS PipingDocument13 pagesMethod Statement - MS PipingAnish KumarNo ratings yet
- Presentation 1Document15 pagesPresentation 1Hala YousefNo ratings yet
- CG 2nd QuarterDocument9 pagesCG 2nd QuarterAura Anne Rose TanNo ratings yet
- Three Legs of The Practitioner's (Skovholt & Starkey 2010)Document6 pagesThree Legs of The Practitioner's (Skovholt & Starkey 2010)Mia Valdes100% (1)
- Hiradc TableDocument1 pageHiradc TablejookapleeNo ratings yet
- EAPP Week 1-5Document10 pagesEAPP Week 1-5Mon Rey B. DuranNo ratings yet
- Hyperkalemia Approach AND Management: Dr. Renuka RayanaDocument38 pagesHyperkalemia Approach AND Management: Dr. Renuka RayanaSap Modules100% (1)
- VACCP Template Checklist - SafetyCultureDocument7 pagesVACCP Template Checklist - SafetyCulturepattysaborio520No ratings yet