Download as pdf or txt
You might also like
- ACR Sample OntarioDocument5 pagesACR Sample OntarioAlisha PowerNo ratings yet
- Incident/Investigation: Rowan County Sheriffs OfficeDocument1 pageIncident/Investigation: Rowan County Sheriffs OfficeAnonymous k3grAlCT1eNo ratings yet
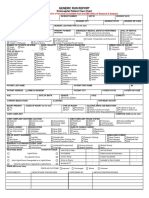
- Sample-Ems Generic Run Report FormDocument2 pagesSample-Ems Generic Run Report FormmeljamerlanNo ratings yet
- SSSForm EC Medical ReimbursementDocument4 pagesSSSForm EC Medical Reimbursementmel7sumatraNo ratings yet
- Generic Run Report: Prehospital Patient Care ChartDocument2 pagesGeneric Run Report: Prehospital Patient Care ChartBCF PRODUCTIONNo ratings yet
- 08 INSARAG Patient Treatment Record PDFDocument1 page08 INSARAG Patient Treatment Record PDFluisacocaliNo ratings yet
- Murder of Marvin Vargas-Osorio Statement of ChargesDocument22 pagesMurder of Marvin Vargas-Osorio Statement of ChargesWJLA-TV100% (2)
- Oods Tebolats Death CertDocument1 pageOods Tebolats Death Certkitty shengpaiNo ratings yet
- DMC Patient FormsDocument6 pagesDMC Patient FormsScott cosentinoNo ratings yet
- Medical History ReportDocument4 pagesMedical History ReportRacel AbulaNo ratings yet
- 20200727082947WEHU-A1A2 - Occupational Accident and Dangerous OccurrenceDocument3 pages20200727082947WEHU-A1A2 - Occupational Accident and Dangerous OccurrenceNORASHIDA BT ABU HASSAN (MOH)No ratings yet
- Incident Report: Please Print Confidential InformationDocument2 pagesIncident Report: Please Print Confidential InformationMuhammad Aulia RahmanNo ratings yet
- Work Related InjuryDocument1 pageWork Related Injuryteguhgama98No ratings yet
- Death Form - 0001Document1 pageDeath Form - 0001mordhwajsingh.jat76No ratings yet
- D.C. Police Incident Report No. 15006043Document3 pagesD.C. Police Incident Report No. 15006043wamu885No ratings yet
- DermatologyDocument8 pagesDermatologySwati joshiNo ratings yet
- WC-1 Submitted Template - a0i53000001Du92AACDocument3 pagesWC-1 Submitted Template - a0i53000001Du92AACnga23sem33300No ratings yet
- EMSPatient First Care FormDocument2 pagesEMSPatient First Care FormJm uniteNo ratings yet
- New NHF Application FormDocument2 pagesNew NHF Application FormEnglishSBAclassNo ratings yet
- CT-FORM 3 BLANKDocument1 pageCT-FORM 3 BLANKArce RostumNo ratings yet
- Health, Safety and Environment Incident and Accident Investigation ReportDocument6 pagesHealth, Safety and Environment Incident and Accident Investigation ReportMuhammad FirdhausNo ratings yet
- M-OSH-009-Incident Report FormDocument1 pageM-OSH-009-Incident Report Formmulugeta114985No ratings yet
- Form No. SO-001-0 - Incident-Accident Investigation ReportDocument1 pageForm No. SO-001-0 - Incident-Accident Investigation Reportannalim.maxiproNo ratings yet
- Police Report Concerning Vandalism of "Silent Sam" Statue at University of North Carolina-Chapel HillDocument1 pagePolice Report Concerning Vandalism of "Silent Sam" Statue at University of North Carolina-Chapel HillThe College FixNo ratings yet
- Emergensi Unit FormDocument2 pagesEmergensi Unit FormMuhammad ridhoNo ratings yet
- First Aid Report FormDocument2 pagesFirst Aid Report FormpestshieldsmarketingNo ratings yet
- WSIB Form6Document4 pagesWSIB Form6Ginette BelangerNo ratings yet
- IBR - Incident Report - 202205004428Document3 pagesIBR - Incident Report - 202205004428Alaska's News SourceNo ratings yet
- Adobe Scan Dec 11, 2022Document1 pageAdobe Scan Dec 11, 2022sukainavazir6No ratings yet
- Accident ReportDocument1 pageAccident ReportwirnosNo ratings yet
- Aaron Kali Quinones Arrested and Charged With Attempted Felony Murder in Miami-Dade County, FL - Jan. 2, 2022Document2 pagesAaron Kali Quinones Arrested and Charged With Attempted Felony Murder in Miami-Dade County, FL - Jan. 2, 2022Omar Rodriguez OrtizNo ratings yet
- Incident Report Muhammad IrfanDocument4 pagesIncident Report Muhammad Irfanarfa vaince100% (1)
- RMD1 Accident Claim FormDocument3 pagesRMD1 Accident Claim FormEffort NkalaNo ratings yet
- Assi ST: Increased Medical PlanDocument7 pagesAssi ST: Increased Medical PlanCarme Ann S. RollonNo ratings yet
- Unity Games Players ProfileDocument3 pagesUnity Games Players ProfilefaithegaloyNo ratings yet
- Death Claim Form RSA: For Death/Final Expenses/ Funeral ClaimsDocument4 pagesDeath Claim Form RSA: For Death/Final Expenses/ Funeral ClaimsMartha MtikaNo ratings yet
- Transforming Global HealthDocument12 pagesTransforming Global HealthShahedul islamNo ratings yet
- Arrest Form in Christopher Luis April 12 Arrest in Feb 13 ShootingDocument1 pageArrest Form in Christopher Luis April 12 Arrest in Feb 13 ShootingAndreaTorresNo ratings yet
- Death at Camelot by The Sea 4.5.17Document2 pagesDeath at Camelot by The Sea 4.5.17ABC15 NewsNo ratings yet
- Notification of Occupational Accident and Dangerous OccurrenceDocument3 pagesNotification of Occupational Accident and Dangerous OccurrenceThevanath Gunasekaran100% (1)
- Incident FormDocument1 pageIncident FormkenandkaraNo ratings yet
- Death Certificate Amended FormDocument1 pageDeath Certificate Amended FormMohammad FamuNo ratings yet
- Smi - Hse Firf02Document11 pagesSmi - Hse Firf02Talal AlrwyanNo ratings yet
- Adverse Events Following Immunization: Philippine Integrated DiseaseDocument2 pagesAdverse Events Following Immunization: Philippine Integrated DiseaseRex DoctoNo ratings yet
- Employer'S Report OF Occupational Injury or Disease: Employer Instructions and Wage Information On Reverse SideDocument2 pagesEmployer'S Report OF Occupational Injury or Disease: Employer Instructions and Wage Information On Reverse SidePete CNo ratings yet
- Final Report - Incident Investigation - Lifting Rafter BeamDocument7 pagesFinal Report - Incident Investigation - Lifting Rafter Beamakbar zulazmiNo ratings yet
- Pla - El Dec 1Document1 pagePla - El Dec 1vale.jimmyjrNo ratings yet
- Cert of Death Tobe FalknerDocument1 pageCert of Death Tobe Falknerras rahmaniNo ratings yet
- Ministry of Public HealthDocument1 pageMinistry of Public Healthfareed121.khamoshNo ratings yet
- Esic Form11Document1 pageEsic Form11Velamala ChhetanNo ratings yet
- SBI Life DEATH CLAIM FORMDocument4 pagesSBI Life DEATH CLAIM FORMCloudy ChefNo ratings yet
- Critical Incident Report FormDocument3 pagesCritical Incident Report FormjirehcounselingNo ratings yet
- Death InvestigateDocument6 pagesDeath InvestigateVanessa DagoocNo ratings yet
- PAO Monthly Report On Person With Disability (PWD)Document1 pagePAO Monthly Report On Person With Disability (PWD)Alinaida MKNo ratings yet
- DOG Houser Incident ReportDocument1 pageDOG Houser Incident ReportDuff LewisNo ratings yet
- Tiger Woods Police ReportDocument14 pagesTiger Woods Police ReportCork GainesNo ratings yet
- Incident Report FromDocument3 pagesIncident Report Fromannerie.krugerNo ratings yet
- 18-Article Word Document-46-2-10-20171111Document5 pages18-Article Word Document-46-2-10-20171111Vaibhav ManeNo ratings yet
- 2014 - Maturation of The Middle Phalanx and CMV - Comperative Study - PerinettiDocument10 pages2014 - Maturation of The Middle Phalanx and CMV - Comperative Study - PerinettiSrdjan StojanovskiNo ratings yet
- Price List NewDocument47 pagesPrice List NewharisNo ratings yet
- Blue and White Illustrated Medical Healthcare in The 21st Century Education Presentation - 20230925 - 110030 - 0000Document8 pagesBlue and White Illustrated Medical Healthcare in The 21st Century Education Presentation - 20230925 - 110030 - 0000Janix MagbanuaNo ratings yet
- Wound Bed PreparationDocument24 pagesWound Bed PreparationnudiaNo ratings yet
- Câu bị độngDocument6 pagesCâu bị độngphamtiendat310705No ratings yet
- BUK Merivaara Accessories BrochureDocument21 pagesBUK Merivaara Accessories Brochureviniciustim9No ratings yet
- Myths About Acute Mountain Sickness (AMS) : # It Cannot Happen To Me. I Am Fit!Document2 pagesMyths About Acute Mountain Sickness (AMS) : # It Cannot Happen To Me. I Am Fit!chahatNo ratings yet
- Waste Dental in IndiaDocument3 pagesWaste Dental in IndiaOktavia DewiNo ratings yet
- Suturing RemovalDocument16 pagesSuturing Removalandrie febriansyahNo ratings yet
- Lyibsiinfi: DinnerDocument173 pagesLyibsiinfi: DinnerdenecsNo ratings yet
- Eye Metaphors Analogies and SimileDocument46 pagesEye Metaphors Analogies and SimileIsus Davi100% (1)
- Formato para Toma de Pedido Antonio 23-02-2024Document8 pagesFormato para Toma de Pedido Antonio 23-02-2024yasmery perezNo ratings yet
- Dwnload Full Davis Advantage For Medical Surgical Nursing Making Connections To Practice 1st Edition Hoffman Test Bank PDFDocument36 pagesDwnload Full Davis Advantage For Medical Surgical Nursing Making Connections To Practice 1st Edition Hoffman Test Bank PDFsparpoil.pian.dpxd100% (17)
- 1 SMDocument10 pages1 SMAnindita GaluhNo ratings yet
- Wellness Brošura: Vaš Kompletan Vodič Za Wellness by Oriflame ProizvodeDocument72 pagesWellness Brošura: Vaš Kompletan Vodič Za Wellness by Oriflame Proizvodesanja_arambasicNo ratings yet
- enDocument78 pagesenElvis Felix fernandes100% (1)
- Sip PresentationDocument19 pagesSip PresentationRAJ KUMAR mefgiNo ratings yet
- BA Dan Hasil Uji Paparan Radiasi Philips MobileDiagnost WDR RSUD Boven DigoelDocument9 pagesBA Dan Hasil Uji Paparan Radiasi Philips MobileDiagnost WDR RSUD Boven DigoelLetsoin MadaNo ratings yet
- Biology TextDocument23 pagesBiology TextMd Fahimul IslamNo ratings yet
- 3-MSDS Rat Granulat - PolandDocument4 pages3-MSDS Rat Granulat - PolandRazaNo ratings yet
- 3shape Implant Studio Surgical Report: ApprovedDocument3 pages3shape Implant Studio Surgical Report: Approvednha khoa NHƯ NGỌCNo ratings yet
- Guide To The Quality EDQM For Human ApplicationDocument462 pagesGuide To The Quality EDQM For Human ApplicationFREDY ALONSO MANTILLA CABALLERONo ratings yet
- Admit Card - AnkushDocument4 pagesAdmit Card - AnkushSurajitNo ratings yet
- List of Hospitals Tajikistan December2020Document12 pagesList of Hospitals Tajikistan December2020Emerit MusicNo ratings yet
- Surgical Approaches in OtorhinolaryngologyDocument381 pagesSurgical Approaches in OtorhinolaryngologyAlice TimbNo ratings yet
- IFR Scout Measurement StepsDocument1 pageIFR Scout Measurement Stepsmajid mierNo ratings yet
- Instilling Nose DropsDocument4 pagesInstilling Nose DropsHarvey T. Dato-onNo ratings yet
- Dass-42 Assessment Form PDFDocument4 pagesDass-42 Assessment Form PDFmarchaNo ratings yet
- Nearest Hospital Road MapDocument1 pageNearest Hospital Road Mapimran.muhammadNo ratings yet