Download as pdf or txt
You might also like
- Prediabetes 1Document21 pagesPrediabetes 1Nirmaa100% (2)
- 35d PDFDocument8 pages35d PDFhuskerchamps0% (1)
- Lakshmi NarayananTextbook of THERAPEUTIC EXERCISES MasudDocument249 pagesLakshmi NarayananTextbook of THERAPEUTIC EXERCISES Masudsandeep92% (217)
- DiabetesDocument99 pagesDiabetes489226fahimNo ratings yet
- Diabetes Mellitus 2021Document61 pagesDiabetes Mellitus 2021Andarge ImperialNo ratings yet
- Diabetes MellitusDocument38 pagesDiabetes MellitustantsaNo ratings yet
- Case 4 SlidesDocument10 pagesCase 4 SlidesOmar RamadanNo ratings yet
- Dsa 698Document12 pagesDsa 698Mwanja MosesNo ratings yet
- Perioperative Management 0F Diabetes Mellitus: BY DR - Vamsi Krishna Moderator: DR - RameshDocument46 pagesPerioperative Management 0F Diabetes Mellitus: BY DR - Vamsi Krishna Moderator: DR - Rameshashwini priyaNo ratings yet
- Diabetes MellitusDocument36 pagesDiabetes Mellitusayeshakhan1060774No ratings yet
- Presenter: Dr. P. Usha Rani Resident, ASRAMS, EluruDocument60 pagesPresenter: Dr. P. Usha Rani Resident, ASRAMS, EluruDivya Rekha KolliNo ratings yet
- DM OGDocument81 pagesDM OGBhagawathgitha Arul MuruganNo ratings yet
- DIABETES MELLITUS FinalDocument83 pagesDIABETES MELLITUS FinalYuvi Yuvaraj100% (1)
- Emergent Disorders of Glucose Metabolism 2010Document56 pagesEmergent Disorders of Glucose Metabolism 2010anuchittakattuNo ratings yet
- Diabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDDocument23 pagesDiabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيار100% (1)
- DM DR - ShamolDocument192 pagesDM DR - ShamolZeeshan AhamedNo ratings yet
- 15 - DiabetesDocument49 pages15 - Diabetesallakami777yousefNo ratings yet
- Diabetes Mellitus: Anne Dawnay Biochemical MedicineDocument26 pagesDiabetes Mellitus: Anne Dawnay Biochemical MedicineJoni HermawanNo ratings yet
- Current Trends in The Diagnosis and Management ofDocument42 pagesCurrent Trends in The Diagnosis and Management ofseun williamsNo ratings yet
- 16.laboratory Support For DiabetesDocument39 pages16.laboratory Support For DiabetesIgwe SolomonNo ratings yet
- 6.2 Diabetes MellitusDocument53 pages6.2 Diabetes MellitusMohammad AlrefaiNo ratings yet
- Diabetes and PregnancyDocument63 pagesDiabetes and PregnancyAyesha KhatunNo ratings yet
- DiabetesDocument14 pagesDiabetesRashmi ThakurNo ratings yet
- Diabetes Mellitus Type 1Document19 pagesDiabetes Mellitus Type 1QwertyNo ratings yet
- Laboratory Diagnosis and Monitoring of Diabetes MellitusDocument65 pagesLaboratory Diagnosis and Monitoring of Diabetes MellitusSonia Afika AzizaNo ratings yet
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocument20 pagesDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- Acute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaDocument30 pagesAcute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaCristinaGheorgheNo ratings yet
- Diabetes MellitusDocument29 pagesDiabetes MellitusIMAFD67% (3)
- Blood Glucose Practical Handout For 2nd Year MBBSDocument10 pagesBlood Glucose Practical Handout For 2nd Year MBBSIMDCBiochemNo ratings yet
- CukrzycaDocument52 pagesCukrzycatyhbbhhNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusLorebellNo ratings yet
- Metabolic Disorders Diabetes HandoutDocument21 pagesMetabolic Disorders Diabetes HandoutEdelen GaleNo ratings yet
- Lecture 6 Carbohydrate MetabolismDocument36 pagesLecture 6 Carbohydrate MetabolismDuduetsang MosalakataneNo ratings yet
- Diabetes Mellitus LectureDocument68 pagesDiabetes Mellitus LectureDikyAksiramNo ratings yet
- Oral Glucose Tolerance TestDocument29 pagesOral Glucose Tolerance TestAhmedmmhNo ratings yet
- Farmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikDocument42 pagesFarmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikAnonymous h76WT2cFdkNo ratings yet
- Blood GlucoseDocument42 pagesBlood GlucoseShaira De La CruzNo ratings yet
- Session 4 Phase 2Document65 pagesSession 4 Phase 2ayoub shams mohamedNo ratings yet
- Pharmaceutical Care of Diabetic MellitusDocument72 pagesPharmaceutical Care of Diabetic Mellitusulfiah rofiantiNo ratings yet
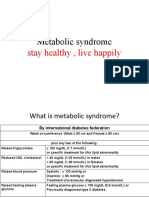
- Metabolic Syndrome: Stay Healthy, Live HappilyDocument32 pagesMetabolic Syndrome: Stay Healthy, Live HappilykomalscientistNo ratings yet
- Diabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022Document93 pagesDiabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022The AbyssinicansNo ratings yet
- DiabetesmellitusDocument24 pagesDiabetesmellitusSania SaeedNo ratings yet
- GESTASIONAL DIABETES MELLITUS SimposiumDocument18 pagesGESTASIONAL DIABETES MELLITUS SimposiumHabiby Habibaty QolbiNo ratings yet
- Glucose Tolerance TestDocument27 pagesGlucose Tolerance Testsiya sharmaNo ratings yet
- Diabetes Mellitus: Dr. Sajid Abbas JaffriDocument37 pagesDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinNo ratings yet
- Diabetes Mellitus CPGDocument137 pagesDiabetes Mellitus CPGKristine-Joy Legaspi FrancoNo ratings yet
- Class 7 (26.07.2022)Document53 pagesClass 7 (26.07.2022)Ãqûã FîggâNo ratings yet
- Diabetes MellitusDocument9 pagesDiabetes MellitusM. Joyce100% (2)
- Diabetes MellitusDocument17 pagesDiabetes MellitusKeeping up with ania kokoNo ratings yet
- Hypoglycemia: Yeditepe University Medical Faculty Department of Endocrinology and MetabolismDocument47 pagesHypoglycemia: Yeditepe University Medical Faculty Department of Endocrinology and MetabolismnawarajNo ratings yet
- Diabetes Mellitus: Nestan BostoganashviliDocument31 pagesDiabetes Mellitus: Nestan BostoganashviliAlireza FarhadiehNo ratings yet
- Diabetes Mellitus: DR Sravan Kumar G MBBS M.D. (Medicine) PGIMER Chandigarh Asst. Prof. of MedicineDocument24 pagesDiabetes Mellitus: DR Sravan Kumar G MBBS M.D. (Medicine) PGIMER Chandigarh Asst. Prof. of MedicineSravan Kumar100% (1)
- 2 - DMDocument18 pages2 - DMRawabi rawabi1997No ratings yet
- What Is Diabetes (PSEm) 02 - 2Document41 pagesWhat Is Diabetes (PSEm) 02 - 2tridewantiwNo ratings yet
- Diabetes Mellitus: - ClassificationDocument22 pagesDiabetes Mellitus: - ClassificationFernando Junior Parra UchasaraNo ratings yet
- DM Part 1 PDFDocument31 pagesDM Part 1 PDFShaila PiloNo ratings yet
- Diabetes Mellitus 2020Document18 pagesDiabetes Mellitus 2020ashmitaaryan01No ratings yet
- Glucose Indices 2022Document40 pagesGlucose Indices 2022mustafa.abdo23112001No ratings yet
- DiabetesDocument59 pagesDiabetesshiv gautamNo ratings yet
- Assessment - and - Management - of - Patients - With - Diabetes - Mellitus (1) FINALDocument80 pagesAssessment - and - Management - of - Patients - With - Diabetes - Mellitus (1) FINALAMIT MODWALNo ratings yet
- Diabetes Mellitus: Investagtion, Diagnosis & Management: DR - Vivek Reddy 1 M.D.SDocument36 pagesDiabetes Mellitus: Investagtion, Diagnosis & Management: DR - Vivek Reddy 1 M.D.SBHEEMREDDY VIVEKREDDY100% (1)
- Answer To Case Study 1 - PASION, MARIA GIE-ANNELYN H.Document4 pagesAnswer To Case Study 1 - PASION, MARIA GIE-ANNELYN H.MARIAGIEANNELYNMANNYLYN PASIONNo ratings yet
- UNIT 3 Animal ProductionDocument15 pagesUNIT 3 Animal ProductionCarla Angela AngwasNo ratings yet
- An Analysis On Maternity Benefit Laws of BangladeshDocument33 pagesAn Analysis On Maternity Benefit Laws of Bangladeshayesha.siddika.241No ratings yet
- Mu350 1Document2 pagesMu350 1kresekjoy2No ratings yet
- LR FPSO DesignDocument34 pagesLR FPSO Designcxb07164No ratings yet
- Pembagian Distribusi Publikasi Peserta Poster IcprpDocument8 pagesPembagian Distribusi Publikasi Peserta Poster IcprpimaNo ratings yet
- TỔNG HỢP CÁC ĐỀ CHUYÊN ANH QUỐC HỌC CÁC NĂMDocument61 pagesTỔNG HỢP CÁC ĐỀ CHUYÊN ANH QUỐC HỌC CÁC NĂMLan Phong TranNo ratings yet
- Kheerganga TrekDocument15 pagesKheerganga TrekMahesh RautNo ratings yet
- Lesson Plan of Education (MS (Document9 pagesLesson Plan of Education (MS (charanjit kaurNo ratings yet
- Prezantimi - Pristina International Airport-AjDocument61 pagesPrezantimi - Pristina International Airport-AjPerparim ShapiNo ratings yet
- RENOLD (Worm Gear - Models PH)Document60 pagesRENOLD (Worm Gear - Models PH)Rodrigo Leal GuzmanNo ratings yet
- James Joyce and The English ViceDocument14 pagesJames Joyce and The English Vicejanna100% (1)
- Surgery 2Document27 pagesSurgery 2junaid4shaikhNo ratings yet
- Ali Baba Vs Amazon SummaryDocument3 pagesAli Baba Vs Amazon SummaryUFC 247100% (1)
- 20140725162928461Document66 pages20140725162928461Edmar AberinNo ratings yet
- CPG - Management of AcneDocument97 pagesCPG - Management of Acneumiraihana1No ratings yet
- Site OrientationDocument2 pagesSite OrientationHitesh VaghasiyaNo ratings yet
- OB-56-Chapter 02 - INP3004-Research Methods in Industrial-Organizational PsychologyDocument40 pagesOB-56-Chapter 02 - INP3004-Research Methods in Industrial-Organizational PsychologyberitahrNo ratings yet
- Widest Selection of Grouting Equipment in The WorldDocument6 pagesWidest Selection of Grouting Equipment in The Worldjet toledoNo ratings yet
- Mountain Man Brewery Company Case AnalysisDocument4 pagesMountain Man Brewery Company Case AnalysisAmit PathakNo ratings yet
- Basic Waste Management Training After Revision (Compatibility Mode)Document64 pagesBasic Waste Management Training After Revision (Compatibility Mode)Gangsar LukmanjayaNo ratings yet
- 5V6 DiodeDocument5 pages5V6 DiodeAchmad Rifdatul HisanNo ratings yet
- Delayed-Action AcceleratorDocument3 pagesDelayed-Action AcceleratorMOHD FIRDAUSNo ratings yet
- LED Main CID2-ATEXDocument4 pagesLED Main CID2-ATEXmarco lezcanoNo ratings yet
- Director Risk Management Investment Accountant in NYC Resume James DwyerDocument2 pagesDirector Risk Management Investment Accountant in NYC Resume James DwyerJamesDwyerNo ratings yet
- Stop Work Authority TBTDocument9 pagesStop Work Authority TBTEeverPaul Casaclang DeLeonNo ratings yet
- Polyaluminium Chloride MSDS DikonversiDocument7 pagesPolyaluminium Chloride MSDS DikonversiPUJI ASTUTINo ratings yet
- Corticosteroids: Dr.R.Prameela, Assistant Professor of Pharmacology, GMC, SrikakulamDocument64 pagesCorticosteroids: Dr.R.Prameela, Assistant Professor of Pharmacology, GMC, SrikakulamRamadi PrameelaNo ratings yet