Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- Principles of Deformity Correction (PDFDrive)Document821 pagesPrinciples of Deformity Correction (PDFDrive)akb6010% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Labour Rate RecommendedDocument102 pagesLabour Rate RecommendedSarinNo ratings yet
- Log in Sign Up Browse: Answers To The Questions in Question Paper From MBA in TQMDocument6 pagesLog in Sign Up Browse: Answers To The Questions in Question Paper From MBA in TQMthakur_neha20_903303No ratings yet
- Vertical VaporizersDocument2 pagesVertical VaporizersMeravigliorso76No ratings yet
- OTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be DoneDocument6 pagesOTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be Doneakb601No ratings yet
- Pipkin Article - Femoral Head FractureDocument17 pagesPipkin Article - Femoral Head Fractureakb601No ratings yet
- Irreducible Fracture-Dislocations of The Femoral Head Without Posterior Wall Acetabular FracturesDocument7 pagesIrreducible Fracture-Dislocations of The Femoral Head Without Posterior Wall Acetabular Fracturesakb601No ratings yet
- The Insall Legacy in Total Knee Arthroplasty: Giles R. Scuderi, MD W. Norman Scott, MD and Gregory H. Tchejeyan, MDDocument12 pagesThe Insall Legacy in Total Knee Arthroplasty: Giles R. Scuderi, MD W. Norman Scott, MD and Gregory H. Tchejeyan, MDakb601No ratings yet
- FC Sem 3 Science in Every Day LifeDocument12 pagesFC Sem 3 Science in Every Day LifeHamza GhadiallyNo ratings yet
- Valdheim: Versión AlphaDocument13 pagesValdheim: Versión AlphaLuis Antonio PelozoNo ratings yet
- Wilderness Survival - Edible and Medicinal Plants PDFDocument60 pagesWilderness Survival - Edible and Medicinal Plants PDFprivatnoNo ratings yet
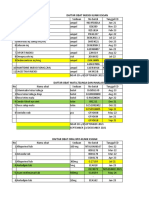
- Hasil Stok Opname Untuk Bap (Fix)Document35 pagesHasil Stok Opname Untuk Bap (Fix)WARDA NABIELANo ratings yet
- My Name: C/o London Hall 1140 Western Road (XXX) XXX-XXXX London, ON, N6G 0A3 E-Mail@addressDocument2 pagesMy Name: C/o London Hall 1140 Western Road (XXX) XXX-XXXX London, ON, N6G 0A3 E-Mail@addressAriellaNo ratings yet
- 98 EntrepreneurshipDocument11 pages98 Entrepreneurshipdolly gorlakorakanaNo ratings yet
- Poverty 2Document9 pagesPoverty 2Camid AlanissahNo ratings yet
- Jainism: "Jain" and "Jainas" Redirect Here. For Other Uses, See andDocument33 pagesJainism: "Jain" and "Jainas" Redirect Here. For Other Uses, See andBhanu MehraNo ratings yet
- AWNMag5 07Document68 pagesAWNMag5 07Michał MrózNo ratings yet
- Irrigation and Water Power Engineering by Dr. B. C. Punmia - Dr. Pande Brij Basi Lal - Ashok Kumar Jain - Arun Kumar JainDocument187 pagesIrrigation and Water Power Engineering by Dr. B. C. Punmia - Dr. Pande Brij Basi Lal - Ashok Kumar Jain - Arun Kumar JainSaritha Reddy85% (85)
- LM10b XSLT To Code ExecutionDocument10 pagesLM10b XSLT To Code ExecutionSaw GyiNo ratings yet
- Relationships PoetryDocument32 pagesRelationships Poetrypierrette1No ratings yet
- Seven Basic Toolsof Quality Control The Appropriate Techniquesfor Solving Quality Problemsinthe OrganizationsDocument11 pagesSeven Basic Toolsof Quality Control The Appropriate Techniquesfor Solving Quality Problemsinthe OrganizationsNigel LimNo ratings yet
- Unfinished Pow UTOLDocument251 pagesUnfinished Pow UTOLresty tacataNo ratings yet
- Intro To MacroeconimicsDocument128 pagesIntro To MacroeconimicsVikas Kumar0% (1)
- Exam Slip 1 SemesterDocument1 pageExam Slip 1 SemesternajwaNo ratings yet
- Post Tensioning System July 2018Document12 pagesPost Tensioning System July 2018pandianNo ratings yet
- Hydro OneDocument28 pagesHydro Onefruitnuts67% (3)
- 1677071391BS German Final Term Result Jan 2023Document2 pages1677071391BS German Final Term Result Jan 2023Raja ZainNo ratings yet
- Non-Local Consciousness and The Anthropo PDFDocument4 pagesNon-Local Consciousness and The Anthropo PDFtoffaloniNo ratings yet
- Syllabus 8 SemDocument9 pagesSyllabus 8 SemRahulNo ratings yet
- B.A. (Gen. English)Document156 pagesB.A. (Gen. English)sandiNo ratings yet
- Failure Codes Fendt 900 Vario 09 2007Document20 pagesFailure Codes Fendt 900 Vario 09 2007Maureen100% (66)
- VMP 530vhmDocument2 pagesVMP 530vhmelienai10% (1)
- GS 2646Document108 pagesGS 2646Wagner BernardinaNo ratings yet
- International Strategic ManagementDocument3 pagesInternational Strategic ManagementmiriiNo ratings yet
- BLM Physics II Um 2021Document78 pagesBLM Physics II Um 2021Tanmayi KartikNo ratings yet