Download as pdf or txt
You might also like
- Iphone XS Schematic PDFDocument51 pagesIphone XS Schematic PDFМихаил ВаравваNo ratings yet
- Get Strong (Ebook)Document218 pagesGet Strong (Ebook)bncns96% (70)
- Welcome To Month 43 of Booty by Bret!: This Month Is A PlanDocument16 pagesWelcome To Month 43 of Booty by Bret!: This Month Is A Planolle3870100% (1)
- Esquema Eletrico Iphone XS Schematic Universotecnico Eagle Team Tech Micro DataDocument47 pagesEsquema Eletrico Iphone XS Schematic Universotecnico Eagle Team Tech Micro DataJoão Carlos FerreiraNo ratings yet
- STEM in Soccer PDFDocument51 pagesSTEM in Soccer PDFRichardVitaldaSilvaNo ratings yet
- Solarposter2023 v5Document1 pageSolarposter2023 v5Mitsuo TsudaNo ratings yet
- Rotulado FotovoltaicasDocument1 pageRotulado FotovoltaicasMauricio GalloNo ratings yet
- Billing Report - July 2022Document100 pagesBilling Report - July 2022Elaine ALdovinoNo ratings yet
- Weekly Adit 3 - 15 - 21 Maret 2021 Down StreamDocument5 pagesWeekly Adit 3 - 15 - 21 Maret 2021 Down Streamreza rNo ratings yet
- SolarPoster2017 Rev1Document1 pageSolarPoster2017 Rev1Ever HuertaNo ratings yet
- Extended Weld Socket Block Connector, Pipe Deep Weld Socket, Pipe / Code 61 or 62 Block Flange or PadDocument4 pagesExtended Weld Socket Block Connector, Pipe Deep Weld Socket, Pipe / Code 61 or 62 Block Flange or PadHuy NguyễnNo ratings yet
- DG List For Diat0323e-SadmmDocument42 pagesDG List For Diat0323e-SadmmAshley KamalasanNo ratings yet
- Msci Ac Asia Health Care Index Usd NetDocument2 pagesMsci Ac Asia Health Care Index Usd NetDanu Ariya NugrahaNo ratings yet
- Ascdc-Man-Op-Concrete Pouring & Testing Monitoring02Document15 pagesAscdc-Man-Op-Concrete Pouring & Testing Monitoring02aristeo garzonNo ratings yet
- Saej 2808 V 001Document10 pagesSaej 2808 V 001kyletgerberNo ratings yet
- RTN Field Procedures and Best Practices: New York State Association of Professional Land Surveyors January 20, 2016Document41 pagesRTN Field Procedures and Best Practices: New York State Association of Professional Land Surveyors January 20, 2016freddy ramdinNo ratings yet
- 005 WPK005-R-2019-RT (AMA Appr) PDFDocument14 pages005 WPK005-R-2019-RT (AMA Appr) PDFMarcus AntoniusNo ratings yet
- Science20200103 DLDocument132 pagesScience20200103 DLBrayann InlvNo ratings yet
- Format Laporan SupervisorDocument4 pagesFormat Laporan SupervisorAnaNo ratings yet
- IE Delhi 08-01-2023Document22 pagesIE Delhi 08-01-2023Harshit KumarNo ratings yet
- Summary ReportDocument16 pagesSummary ReportCRISTHNo ratings yet
- Weekly Adit 3 - Down Stream JanDocument6 pagesWeekly Adit 3 - Down Stream JanReza RomadhoniNo ratings yet
- Dailly Ms-Online Shop 12082020Document88 pagesDailly Ms-Online Shop 12082020jimyNo ratings yet
- Reporte de Matriz Adecco 2023 (2) (1) .Document168 pagesReporte de Matriz Adecco 2023 (2) (1) .Daniel Pachac EchajayaNo ratings yet
- Nomina Del 06 de Octubre Al 12 de Octubre de 2023Document1 pageNomina Del 06 de Octubre Al 12 de Octubre de 2023Victoria Stephania Hinojosa GarridoNo ratings yet
- National Ski Areas Association Catastrophic Injury Fact Sheet 2017Document2 pagesNational Ski Areas Association Catastrophic Injury Fact Sheet 2017Michael_Lee_RobertsNo ratings yet
- Right Side View: Loader FrameDocument2 pagesRight Side View: Loader Frametommy lanyonNo ratings yet
- Weekly Adit 3 - Down Stream FebruariDocument4 pagesWeekly Adit 3 - Down Stream FebruariReza RomadhoniNo ratings yet
- Schedule MP Hida-1Document7 pagesSchedule MP Hida-1TRI CANDRAKIRANANo ratings yet
- Jadwal Pelaksanaan Pekerjaan BarchartDocument1 pageJadwal Pelaksanaan Pekerjaan Barchartharrys manaluNo ratings yet
- Weekly Adit 3 - Down Stream MaretDocument4 pagesWeekly Adit 3 - Down Stream MaretReza RomadhoniNo ratings yet
- Elur Cp02 Sut 147 (ST) - Sy2 ResponseDocument14 pagesElur Cp02 Sut 147 (ST) - Sy2 ResponseRey Dominique VillarNo ratings yet
- 10 Times Faster Than Thought: Earth's Magnetic Field Can ChangeDocument2 pages10 Times Faster Than Thought: Earth's Magnetic Field Can ChangeGMNo ratings yet
- 6 10 10 Inlet 8"Fl 6 4: 19/03/2014 AriehDocument4 pages6 10 10 Inlet 8"Fl 6 4: 19/03/2014 AriehRobynfbNo ratings yet
- Cold War - Shape Message 15 Dec 80Document2 pagesCold War - Shape Message 15 Dec 80Anonymous MEPDHKzboD0% (1)
- Edminister ElectricCircuitsDocument220 pagesEdminister ElectricCircuitshiralalnhpcNo ratings yet
- Attendance 2023Document17 pagesAttendance 2023Koy DamalerioNo ratings yet
- Wacc TslaDocument11 pagesWacc Tslavlad vladNo ratings yet
- Endovascular Treatment of Acute Ischemic Stroke.7-1 PDFDocument22 pagesEndovascular Treatment of Acute Ischemic Stroke.7-1 PDFCristina GhizdavetNo ratings yet
- DanfeDocument1 pageDanfeAoNx Pro BitNo ratings yet
- 2 - Casing Slip Type UC-3Document1 page2 - Casing Slip Type UC-3leoNo ratings yet
- Lamp KM MasterplanDocument15 pagesLamp KM MasterplanBasukiNo ratings yet
- Weekly Adit 3 - Down Stream JuniDocument2 pagesWeekly Adit 3 - Down Stream JuniReza RomadhoniNo ratings yet
- Time Schedule R2 PROYEK GRAHA GATSU - Jl. Gatot Subroto Jakarta SelatanDocument1 pageTime Schedule R2 PROYEK GRAHA GATSU - Jl. Gatot Subroto Jakarta SelatanReza ZulfiNo ratings yet
- General Arrangement, AIR COOLED (R90-110) 23539836 GDocument7 pagesGeneral Arrangement, AIR COOLED (R90-110) 23539836 GCarlos JiménezNo ratings yet
- Radiogrphy Inspection of Corrosion Circuit (Wnd-Pj-Cs-27)Document14 pagesRadiogrphy Inspection of Corrosion Circuit (Wnd-Pj-Cs-27)Prasad ChakkrapaniNo ratings yet
- Warren Miller's SnoWorld #68Document92 pagesWarren Miller's SnoWorld #68Warren MillerNo ratings yet
- En Exhibitor GuideDocument9 pagesEn Exhibitor GuideNathalia Vasconcelos Barroso Todt AragãoNo ratings yet
- Cross Reference Chart: VibisaDocument1 pageCross Reference Chart: VibisaJose Ivan Carvajal CortizosNo ratings yet
- Professional Development Program Icc Indonesia 2022 v2 CompressedDocument50 pagesProfessional Development Program Icc Indonesia 2022 v2 CompressedKenia OvarianaNo ratings yet
- January, 2023 Gas Production and Utilization DataDocument1 pageJanuary, 2023 Gas Production and Utilization DataMohdNo ratings yet
- Jadwal Pelaksanaan Pekerjaan: Realisasi Bulan 1 MeiDocument1 pageJadwal Pelaksanaan Pekerjaan: Realisasi Bulan 1 Meielang supriyadiNo ratings yet
- Oktober 22Document3 pagesOktober 22alimin butonNo ratings yet
- Integrally Reinforced Forged Branch Outlet Fittings - Socket Welding, Threaded, and Buttwelding EndsDocument22 pagesIntegrally Reinforced Forged Branch Outlet Fittings - Socket Welding, Threaded, and Buttwelding EndsVinoth MechNo ratings yet
- India Today - May 14 2018Document128 pagesIndia Today - May 14 2018PoojaSharmaNo ratings yet
- February, 2023 Gas Production and Utilization DataDocument1 pageFebruary, 2023 Gas Production and Utilization DataMohdNo ratings yet
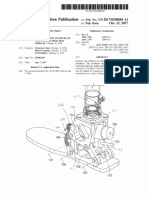
- 2017 Us20170290684a1Document19 pages2017 Us20170290684a1Daffa Hafiz ZaidanNo ratings yet
- Profile Structurale Si Prelucrari Mecanice: Divisione Acciaio Al CarbonioDocument17 pagesProfile Structurale Si Prelucrari Mecanice: Divisione Acciaio Al CarbonioStefanRazvanStanNo ratings yet
- Drawing NO.: Shipping CNTR Assy 14.5" IDDocument1 pageDrawing NO.: Shipping CNTR Assy 14.5" IDNguyễn LâmNo ratings yet
- Jadwal Pelaksanaan Induk (Cco-01)Document2 pagesJadwal Pelaksanaan Induk (Cco-01)surya bimaNo ratings yet
- Absensi Pegawai Uptd Puskesmas Way Jepara: Bulan: Januari 2021Document35 pagesAbsensi Pegawai Uptd Puskesmas Way Jepara: Bulan: Januari 2021arif_mzNo ratings yet
- Science Test-10TH-SCIENCEDocument5 pagesScience Test-10TH-SCIENCEtensazangestuiit24No ratings yet
- Integumentary System WorksheetDocument4 pagesIntegumentary System WorksheetLAQUESHA MAJORS0% (1)
- Azza Mohamed Ahmed Said Professor of Ophthalmology Ain Shams UniversityDocument54 pagesAzza Mohamed Ahmed Said Professor of Ophthalmology Ain Shams UniversityraeNo ratings yet
- Robin Gallant39s Intensive Max Glute Hypertrophy PDocument8 pagesRobin Gallant39s Intensive Max Glute Hypertrophy PSavitaNo ratings yet
- Organ SystemDocument2 pagesOrgan SystemCristina RamirezNo ratings yet
- Icd 9 CM Keterangan Di Icd 9 CM: Drainage Abscess Pada Mandibula / Sub MandibulaDocument2 pagesIcd 9 CM Keterangan Di Icd 9 CM: Drainage Abscess Pada Mandibula / Sub Mandibulanoerrekmed_816409184No ratings yet
- Teori AicaDocument22 pagesTeori AicaaghniajolandaNo ratings yet
- Higher Mental Functions OldDocument36 pagesHigher Mental Functions OldPriya Kuberan100% (1)
- The Eighteen Luohan Exercises According To Xu YushengDocument6 pagesThe Eighteen Luohan Exercises According To Xu YushengRoberto BaptistaNo ratings yet
- Delivery of The Aftercoming HeadDocument7 pagesDelivery of The Aftercoming HeadHendri KunNo ratings yet
- Autologous Tracheal Replacement Surgical Technique 2018 Thoracic Surgery CLDocument9 pagesAutologous Tracheal Replacement Surgical Technique 2018 Thoracic Surgery CLEdgar ForeroNo ratings yet
- Lapjag 13 OktDocument24 pagesLapjag 13 OktMartha SimonaNo ratings yet
- Brain Bee R1 P2Document9 pagesBrain Bee R1 P2sarahsyedazakiNo ratings yet
- Oral Habits 1233Document43 pagesOral Habits 1233Sayuj SureshNo ratings yet
- Nervous SystemDocument49 pagesNervous SystemJoyce NieveraNo ratings yet
- Lower Limb MusclesDocument43 pagesLower Limb MusclesJonah DelmundoNo ratings yet
- Module 8 - Physical AssessmentDocument10 pagesModule 8 - Physical AssessmentPaulette Poseskie CoatesNo ratings yet
- Test Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 DownloadDocument69 pagesTest Bank For Laboratory Manual For Seeleys Anatomy Physiology 11th Edition Eric Wise 3 Downloadcaseyyoungtoekwmcfdi100% (29)
- Lobes, Fissures, and Bronchopulmonary SegmentsDocument13 pagesLobes, Fissures, and Bronchopulmonary SegmentsJansi OrtizNo ratings yet
- Veterinary Medical Terminology: Dr.H.HoseinzadehDocument16 pagesVeterinary Medical Terminology: Dr.H.HoseinzadehJuk CondeNo ratings yet
- Special Senses 1 - (1) - NDocument128 pagesSpecial Senses 1 - (1) - Naoujahmed123456789010No ratings yet
- Physical Examination:-: Vital SignsDocument4 pagesPhysical Examination:-: Vital SignspriyaNo ratings yet
- Introductiontohumanphysiology PDFDocument30 pagesIntroductiontohumanphysiology PDFkrishna baithaNo ratings yet
- Recall April 19 DR MominDocument7 pagesRecall April 19 DR MominShariq ShaNo ratings yet
- Bio12 Cheat Sheet RubricDocument2 pagesBio12 Cheat Sheet Rubricapi-310678040No ratings yet
- Bioptron Colour 24Document35 pagesBioptron Colour 24diNo ratings yet
- 9780443049767Document15 pages9780443049767Angela PagliusoNo ratings yet
- Scapular Orientation Exercises JOSPTDocument8 pagesScapular Orientation Exercises JOSPTAnuj MehtaNo ratings yet