Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 24 Oet Full TestsDocument212 pages24 Oet Full TestsJoe Single89% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Viruses H2 BioDocument13 pagesViruses H2 BioJin Yang ChewNo ratings yet
- Abzymes and Its ApplicationsDocument36 pagesAbzymes and Its ApplicationsKritika Verma100% (2)
- Stephen J. Marsden - CCH Australia Limited Australian Practical Accounting Guide Wolters Kluwer 2020Document384 pagesStephen J. Marsden - CCH Australia Limited Australian Practical Accounting Guide Wolters Kluwer 2020Jenny NguyenNo ratings yet
- Men4b Psa TechnicalDocument98 pagesMen4b Psa TechnicalJenny NguyenNo ratings yet
- RHW ANSC Guidelines (February V2 2018)Document36 pagesRHW ANSC Guidelines (February V2 2018)Jenny NguyenNo ratings yet
- National Guide 3rd Adult Chart Sept 2018 WebDocument2 pagesNational Guide 3rd Adult Chart Sept 2018 WebJenny NguyenNo ratings yet
- Revised HMIS Indicators, Recording & Reporting Tools: PresenterDocument22 pagesRevised HMIS Indicators, Recording & Reporting Tools: PresenterZerihun Bekele100% (2)
- Nursing Care of Child With LIFE THREATENING CONDITIONSDocument70 pagesNursing Care of Child With LIFE THREATENING CONDITIONSinno so qtNo ratings yet
- Chapter 1 Intro To CellDocument6 pagesChapter 1 Intro To CellrexartoozNo ratings yet
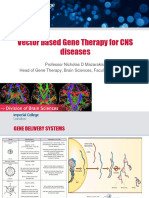
- Prof N D Mazarakis MSC GT Lecture 2022Document23 pagesProf N D Mazarakis MSC GT Lecture 2022hdin431No ratings yet
- ImmunochemistryDocument44 pagesImmunochemistryJowe VarnalNo ratings yet
- History of Blood BankingDocument5 pagesHistory of Blood Bankingradiz.soltaNo ratings yet
- AIDS Case StudyDocument4 pagesAIDS Case StudyAlexandria BrooksNo ratings yet
- Sciences: Grade 11 TextbookDocument376 pagesSciences: Grade 11 TextbookPriyanka KanaNo ratings yet
- Step NotesDocument132 pagesStep NotesjohnkadNo ratings yet
- "Serosurveillance of Blood Donors" Dr. Anandkumar GurupadappaDocument145 pages"Serosurveillance of Blood Donors" Dr. Anandkumar GurupadappaTEJU MURTHYNo ratings yet
- Hiv and Aids - ReportDocument8 pagesHiv and Aids - Reportchezyl cadinongNo ratings yet
- Rekambys Epar Product Information - en PDFDocument74 pagesRekambys Epar Product Information - en PDFCamelia AirineiNo ratings yet
- Mark Scheme For January 2011: BiologyDocument25 pagesMark Scheme For January 2011: BiologyshavindriNo ratings yet
- HIV and AIDSDocument75 pagesHIV and AIDSMarc Imhotep Cray, M.D.100% (1)
- Virology User ManualDocument24 pagesVirology User ManualMedo2012No ratings yet
- Hivaids - Book ChapterDocument9 pagesHivaids - Book ChapterNnaji OgochukwuNo ratings yet
- Mms Protocol - Hiv & AidsDocument4 pagesMms Protocol - Hiv & AidsThandolwetu Sipuye100% (1)
- Immunity, Infection & ForensicsDocument8 pagesImmunity, Infection & ForensicshtbfdgNo ratings yet
- H.I.V. Crossword PuzzleDocument3 pagesH.I.V. Crossword Puzzlejackie pascualNo ratings yet
- Karp CH 1Document17 pagesKarp CH 1mikadeguzman100% (1)
- BIO CHEM University Papers With Model AnswersDocument58 pagesBIO CHEM University Papers With Model AnswersSp Ppv100% (1)
- Concepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionDocument9 pagesConcepts in Immunologic Function: Chapter 35: Assessment of Immune FunctionKristine KimNo ratings yet
- Hiv Awareness Purpose: GoalDocument2 pagesHiv Awareness Purpose: GoalChristopher GalivoNo ratings yet
- Anti-Hiv Using NanorobotsDocument10 pagesAnti-Hiv Using NanorobotsashiNo ratings yet
- 15 Impressive Herbs With Antiviral Activity PDFDocument6 pages15 Impressive Herbs With Antiviral Activity PDFdan4scribdNo ratings yet
- Life CellDocument2 pagesLife CellSuman HazariNo ratings yet