Download as pdf or txt
You might also like
- Unconscious Influences On Decision Making - A Critical Review PDFDocument61 pagesUnconscious Influences On Decision Making - A Critical Review PDFMaicon GabrielNo ratings yet
- Cognitive DebiasingDocument7 pagesCognitive DebiasingJefferson ChavesNo ratings yet
- Jumping To ConclusionsDocument12 pagesJumping To ConclusionsYuzuki KokonoeNo ratings yet
- Journal Pone 0288275Document32 pagesJournal Pone 0288275Mauricio CastroNo ratings yet
- Dual Process Model For AutismDocument11 pagesDual Process Model For AutismATID Fabi Rodríguez de la ParraNo ratings yet
- Sjastad, H., & Baumeister, R. F., (2023), Fast Optimism, Slow Realism. Causal Evidence For Two-Step Model of Future ThinkingDocument14 pagesSjastad, H., & Baumeister, R. F., (2023), Fast Optimism, Slow Realism. Causal Evidence For Two-Step Model of Future Thinking9 PsychologyNo ratings yet
- Differences in Cognitive-Perceptual Factors Arising From Variations in Self-Professed Paranormal AbilityDocument8 pagesDifferences in Cognitive-Perceptual Factors Arising From Variations in Self-Professed Paranormal AbilityAnonymous v8EQ497yNo ratings yet
- Stanovich ThePsychologist PDFDocument4 pagesStanovich ThePsychologist PDFluistxo2680100% (1)
- Guia Demencia DCLDocument10 pagesGuia Demencia DCLmaricellap31No ratings yet
- Mandel 2019Document3 pagesMandel 2019Instituto Colombiano de PsicometriaNo ratings yet
- 2016 MDS PDFDocument15 pages2016 MDS PDFBognár ErzsébetNo ratings yet
- Evidence Based Case Report - Assessing Developmental Delay: BMJ Clinical Research August 2001Document3 pagesEvidence Based Case Report - Assessing Developmental Delay: BMJ Clinical Research August 2001Novie AstiniNo ratings yet
- DenneyDocument44 pagesDenneymaría del pinoNo ratings yet
- The Association of Anxiety and Depressive SymptomsDocument13 pagesThe Association of Anxiety and Depressive SymptomsAlina CiobanuNo ratings yet
- Research Paper:: Cognitive Process in Patients With Obsessive-Compulsive Disorder: A Cross-Sectional Analytic StudyDocument10 pagesResearch Paper:: Cognitive Process in Patients With Obsessive-Compulsive Disorder: A Cross-Sectional Analytic StudyTrifan DamianNo ratings yet
- 36 - Decision-Making and Risk-Taking in Forensic and Non-Forensic Patients With Schizophrenia Spectrum Disorders A Multicenter European StudyDocument8 pages36 - Decision-Making and Risk-Taking in Forensic and Non-Forensic Patients With Schizophrenia Spectrum Disorders A Multicenter European Studygabri93bioNo ratings yet
- 404 Letters: Reliability and Validity of Diagnostic TestsDocument2 pages404 Letters: Reliability and Validity of Diagnostic TestsLay LylyNo ratings yet
- Anxious People More Apt To Make Bad Decisions Amid UncertaintyDocument4 pagesAnxious People More Apt To Make Bad Decisions Amid UncertaintyMaria Lucia Sanchez GabinoNo ratings yet
- Childhood Onset Schizophrenia High Rate of Visual HallucinationsDocument9 pagesChildhood Onset Schizophrenia High Rate of Visual HallucinationsmiaaNo ratings yet
- Deterioro de La Toma de Decisiones en Los Intentos de Suicidio de AdolescentesDocument17 pagesDeterioro de La Toma de Decisiones en Los Intentos de Suicidio de AdolescentescarolinaNo ratings yet
- The Design Organization Test: Further Demonstration of Reliability and Validity As A Brief Measure of Visuospatial AbilityDocument14 pagesThe Design Organization Test: Further Demonstration of Reliability and Validity As A Brief Measure of Visuospatial AbilitySamorNo ratings yet
- Comprehensive Psychiatry: Paul T. Van Der Heijden, Irma Cefo, Cilia L.M. Witteman, Koen P. GrootensDocument4 pagesComprehensive Psychiatry: Paul T. Van Der Heijden, Irma Cefo, Cilia L.M. Witteman, Koen P. GrootensAnita DewiNo ratings yet
- Intelligence and Emotional Disorders - PAID - 2015 PDFDocument4 pagesIntelligence and Emotional Disorders - PAID - 2015 PDFOmar Azaña Velez100% (1)
- Imaginative and Dissociative Processes I No CD SampleDocument20 pagesImaginative and Dissociative Processes I No CD Sampleera kokedhimaNo ratings yet
- Material For IndecisionsDocument12 pagesMaterial For IndecisionsJuan Se DazaNo ratings yet
- Neuroxpsychological Assessment of Psychogeriatric Patients With Limited EducationDocument11 pagesNeuroxpsychological Assessment of Psychogeriatric Patients With Limited Educationmacarena.isebNo ratings yet
- Aulia Derra BerliantiDocument12 pagesAulia Derra BerliantiAulia Derra BerliantiNo ratings yet
- D6 N E1 EssayDocument8 pagesD6 N E1 EssayKa AlvarengaNo ratings yet
- People Need To Care About The Truth To Be RationalDocument9 pagesPeople Need To Care About The Truth To Be RationalPeter PetroffNo ratings yet
- Fpsyg 12 670959Document16 pagesFpsyg 12 670959sripoojitha511No ratings yet
- Autism Research - 2009 - Kuschner - Local Vs Global Approaches To Reproducing The Rey Osterrieth Complex Figure byDocument11 pagesAutism Research - 2009 - Kuschner - Local Vs Global Approaches To Reproducing The Rey Osterrieth Complex Figure byLiad BelaNo ratings yet
- Practitioner's Guide To Evaluating Change With Neuropsychological Assessment Instruments (PDFDrive)Document562 pagesPractitioner's Guide To Evaluating Change With Neuropsychological Assessment Instruments (PDFDrive)Miguel Alvarez100% (1)
- Reduced Behavioral Flexibility in Autism Spectrum Disorders: Neuropsychology March 2013Document18 pagesReduced Behavioral Flexibility in Autism Spectrum Disorders: Neuropsychology March 2013Andreia SilvaNo ratings yet
- 2020 First Prize Psychology EssayDocument3 pages2020 First Prize Psychology Essayzihan.zhou856No ratings yet
- Longitudinal Study of The Transition From Healthy Aging To Alzheimer DiseaseDocument22 pagesLongitudinal Study of The Transition From Healthy Aging To Alzheimer DiseasePaco Herencia PsicólogoNo ratings yet
- The Characteristics of Unacceptable/taboo Thoughts in Obsessive - Compulsive DisorderDocument8 pagesThe Characteristics of Unacceptable/taboo Thoughts in Obsessive - Compulsive DisorderMaria Isabel Montañez RestrepoNo ratings yet
- Is Knowing Always FeelingDocument2 pagesIs Knowing Always FeelingvitalieNo ratings yet
- Cognitive Insight As An Indicator of Competence To Consent To Treatment in SchizophreniaDocument4 pagesCognitive Insight As An Indicator of Competence To Consent To Treatment in SchizophreniaJulio DelgadoNo ratings yet
- The Value of BeliefsDocument5 pagesThe Value of BeliefsDavid PedrosaNo ratings yet
- An Exploratory Investigation of Real World Reasoning in ParanoiaDocument16 pagesAn Exploratory Investigation of Real World Reasoning in ParanoiaLizeth RosasNo ratings yet
- The Influence of Improper Sets of Information On Judgment: How Irrelevant Information Can Bias Judged ProbabilityDocument20 pagesThe Influence of Improper Sets of Information On Judgment: How Irrelevant Information Can Bias Judged ProbabilityJesse PanchoNo ratings yet
- Competence To Consent and Its Relationship With Cognitive Function in Patients With SchizophreniaDocument5 pagesCompetence To Consent and Its Relationship With Cognitive Function in Patients With SchizophreniaJulio DelgadoNo ratings yet
- Clinical PsychologyDocument7 pagesClinical PsychologykateNo ratings yet
- Issues Surrounding Reliability and Validity-1Document38 pagesIssues Surrounding Reliability and Validity-1kylieverNo ratings yet
- Cognitive Bias: Recognizing and Managing Our Unconscious BiasesDocument5 pagesCognitive Bias: Recognizing and Managing Our Unconscious BiasesYosephNo ratings yet
- Tuokko DCL To DemenciaDocument23 pagesTuokko DCL To DemenciaRAYMUNDO ARELLANONo ratings yet
- Taking Subjectivity Seriously: Towards A Uni Fication of Phenomenology, Psychiatry, and NeuroscienceDocument7 pagesTaking Subjectivity Seriously: Towards A Uni Fication of Phenomenology, Psychiatry, and NeurosciencealexandracastellanosgoNo ratings yet
- Journal Pcbi 1008484Document31 pagesJournal Pcbi 1008484thinh_41No ratings yet
- Ne Zirog Lu 1999Document22 pagesNe Zirog Lu 1999Ivan SBNo ratings yet
- Alternatives To Psychiatric DiagnosisDocument3 pagesAlternatives To Psychiatric Diagnosisfabiola.ilardo.15No ratings yet
- 22Q 11 2-WiscDocument21 pages22Q 11 2-WiscMRHNo ratings yet
- Idusohan Moizer2013Document12 pagesIdusohan Moizer2013patricia lodeiroNo ratings yet
- Nihms 1883904Document22 pagesNihms 1883904Tiago BaraNo ratings yet
- Ni Hms 467272Document13 pagesNi Hms 467272Sócrates BôrrasNo ratings yet
- Arousability, Personality, and Decision-Making Ability in Dissociative DisorderDocument7 pagesArousability, Personality, and Decision-Making Ability in Dissociative DisorderPrasanta RoyNo ratings yet
- The Choice Point Model of Acceptance and Commitment Therapy With Inpatient Substance Use and Co-Occurring PopulationsDocument14 pagesThe Choice Point Model of Acceptance and Commitment Therapy With Inpatient Substance Use and Co-Occurring PopulationsGustavo PaniaguaNo ratings yet
- Affect, Risk, and Decision Making: Paul Slovic and Ellen Peters Melissa L. FinucaneDocument6 pagesAffect, Risk, and Decision Making: Paul Slovic and Ellen Peters Melissa L. FinucaneBrick HartNo ratings yet
- Ranasinghe 2016Document12 pagesRanasinghe 2016Luciana CassimiroNo ratings yet
- Ni Hms 91893 ArticuloDocument14 pagesNi Hms 91893 ArticulomellaNo ratings yet
- Pediatric Neuropsychiatry: A Case-Based ApproachFrom EverandPediatric Neuropsychiatry: A Case-Based ApproachAaron J. HauptmanNo ratings yet
- SAP FM Organization ChartDocument1 pageSAP FM Organization Chartmalik_naseerullah100% (1)
- SAP Fund ManagementDocument4 pagesSAP Fund Managementmalik_naseerullah100% (1)
- MM SAP Create-Purchase-Order PDFDocument6 pagesMM SAP Create-Purchase-Order PDFmalik_naseerullahNo ratings yet
- Muslim Baby Boys & Girls Names PDFDocument72 pagesMuslim Baby Boys & Girls Names PDFmalik_naseerullahNo ratings yet
- UoL ITS Create Purchase Order R02Document16 pagesUoL ITS Create Purchase Order R02Sergio MorenoNo ratings yet
- SAP FICO BanK ConfigurationDocument46 pagesSAP FICO BanK ConfigurationSriram RangarajanNo ratings yet
- Pricing Configuration: Steps: Step 1: Create Condition TablesDocument6 pagesPricing Configuration: Steps: Step 1: Create Condition Tablesmalik_naseerullahNo ratings yet
- Sap FicoDocument44 pagesSap Ficomalik_naseerullah100% (1)
- 3871-Article Text-14575-1-10-20220629Document11 pages3871-Article Text-14575-1-10-20220629Nuurul BayaanNo ratings yet
- Mid Radius LocationDocument12 pagesMid Radius LocationKembhavi SMNo ratings yet
- SystatDocument8 pagesSystatSamuel BezerraNo ratings yet
- The Influence of Sociocultural Factors On Body Image: A Meta-AnalysisDocument13 pagesThe Influence of Sociocultural Factors On Body Image: A Meta-AnalysisIbec PagamentosNo ratings yet
- Canonical Correlation - MATLAB Canoncorr - MathWorks IndiaDocument2 pagesCanonical Correlation - MATLAB Canoncorr - MathWorks IndiaYuvaraj MaranNo ratings yet
- Priority Sector Lending and Non-Performing Assets: Status, Impact & IssuesDocument7 pagesPriority Sector Lending and Non-Performing Assets: Status, Impact & IssuespraharshithaNo ratings yet
- Validity and Reliability of A Postoperative Quality of Recovery Score: The Qor-40Document5 pagesValidity and Reliability of A Postoperative Quality of Recovery Score: The Qor-40Gaetano De BiaseNo ratings yet
- From Seeing To Remembering: Images With Harder-To-Reconstruct Representations Leave Stronger Memory TracesDocument23 pagesFrom Seeing To Remembering: Images With Harder-To-Reconstruct Representations Leave Stronger Memory TracesAnaNo ratings yet
- Infrastructure As Important Determinant of Tourism Development in The Countries of Southeast EuropeDocument7 pagesInfrastructure As Important Determinant of Tourism Development in The Countries of Southeast EuropeAliNo ratings yet
- The Effects of Oar-Shaft Stiffness andDocument9 pagesThe Effects of Oar-Shaft Stiffness andValentina DiamanteNo ratings yet
- Textbook Statistics For The Terrified John H Kranzler Ebook All Chapter PDFDocument53 pagesTextbook Statistics For The Terrified John H Kranzler Ebook All Chapter PDFstephen.jones510100% (6)
- Assignment 1 MIN E 613 Thiago MizunoDocument5 pagesAssignment 1 MIN E 613 Thiago MizunoThiago Alduini MizunoNo ratings yet
- A Level Math Paper 2 Correlation and Scatter DiagramsDocument30 pagesA Level Math Paper 2 Correlation and Scatter DiagramsAyiko MorganNo ratings yet
- Hotel Lobby Ambient Lighting Case StudyDocument12 pagesHotel Lobby Ambient Lighting Case StudyVerin IchiharaNo ratings yet
- 2021 The Reliability of Dental Age Estimation in AdultsDocument5 pages2021 The Reliability of Dental Age Estimation in AdultsrofieimNo ratings yet
- Quiz RegressionDocument27 pagesQuiz Regressionnancy 1996100% (2)
- Week 5, Unit 2 Quantitative and Qualitative Data AnalysisDocument54 pagesWeek 5, Unit 2 Quantitative and Qualitative Data AnalysisKevin Davis100% (1)
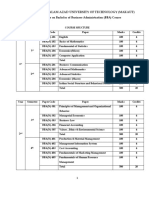
- BBM 3rd Sem Syllabus 2014 PDFDocument12 pagesBBM 3rd Sem Syllabus 2014 PDFBhuwanNo ratings yet
- Evaluation of Allen and Meyer's Organizational Commitment Scale: A Cross-Cultural Application in PakistanDocument8 pagesEvaluation of Allen and Meyer's Organizational Commitment Scale: A Cross-Cultural Application in PakistansabahatfatimaNo ratings yet
- Neuromarketing & Ethics: How Far Should We Go With Predicting Consumer Behavior?Document10 pagesNeuromarketing & Ethics: How Far Should We Go With Predicting Consumer Behavior?adelineo vlog ONo ratings yet
- Soil PH, Bone Preservation, and Sampling Bias at Mortuary SitesDocument7 pagesSoil PH, Bone Preservation, and Sampling Bias at Mortuary SitesCeilidh Lerwick100% (1)
- S1 Correlation and Regression - PMCCDocument22 pagesS1 Correlation and Regression - PMCCsakibsultan_308No ratings yet
- Individual AssigngmentDocument13 pagesIndividual AssigngmentKeyd MuhumedNo ratings yet
- Standard Costing Vs Normal Costing in ManufacturingDocument19 pagesStandard Costing Vs Normal Costing in ManufacturingkrisNo ratings yet
- Bine MakautDocument37 pagesBine Makauts ghoshNo ratings yet
- NicolaidouECEL2019 Paper Social Media LiteracyDocument8 pagesNicolaidouECEL2019 Paper Social Media LiteracySveta SlyvchenkoNo ratings yet
- Mathematics: Pearson Edexcel Level 3 GCEDocument25 pagesMathematics: Pearson Edexcel Level 3 GCEayesha safdarNo ratings yet
- K - PPT - Simple Regression and CorrelationDocument21 pagesK - PPT - Simple Regression and CorrelationDhara MehtaNo ratings yet
- Applying Statistics To Analysis of Corrosion Data: Standard Guide ForDocument14 pagesApplying Statistics To Analysis of Corrosion Data: Standard Guide Forsriram vikasNo ratings yet
- Exploratory Data Analysis-1 (EDA-1)Document38 pagesExploratory Data Analysis-1 (EDA-1)Sparsh VijayvargiaNo ratings yet