
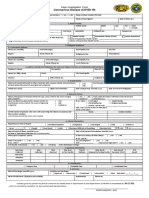
Case Lnvestigation Form
Case Lnvestigation Form
You might also like
- Benguet GIDA ListDocument1 pageBenguet GIDA ListChum ChitaruNo ratings yet
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument4 pagesCoronavirus Disease (COVID-19) : Case Investigation FormMaria JoselaNo ratings yet
- Health Declaration Form DOT AmendedDocument1 pageHealth Declaration Form DOT AmendedImee S. YuNo ratings yet
- 101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinDocument17 pages101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinFilipeCarvalho100% (7)
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- New Cif FormDocument2 pagesNew Cif FormNovie FeneciosNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- Saric CifDocument1 pageSaric CifMarav SymbNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Health Declaration Form: Applicant ProfileDocument1 pageHealth Declaration Form: Applicant ProfileOnyx XynoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Cif V9Document4 pagesCif V9SACH COVID 19 TASK FORCE SecretariatNo ratings yet
- Admitted in Multiple Health FacilitiesDocument5 pagesAdmitted in Multiple Health FacilitiesLemuel PetronioNo ratings yet
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesCase Investigation Form Coronavirus Disease (COVID-19)juwan decastroNo ratings yet
- Research Institute For Tropical Medicine: Admitted in Multiple Health FacilitiesDocument5 pagesResearch Institute For Tropical Medicine: Admitted in Multiple Health FacilitiesYescha FabitoNo ratings yet
- Youssry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Document5 pagesYoussry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Youssry JaranillaNo ratings yet
- CIF - Version 7wordDocument3 pagesCIF - Version 7wordBALIUAG DISTRICT LABORATORYNo ratings yet
- Chelsea L. Manalansan MD: Barangay Bulusan, Calapan City Oriental Mindoro 09634017938Document5 pagesChelsea L. Manalansan MD: Barangay Bulusan, Calapan City Oriental Mindoro 09634017938Youssry JaranillaNo ratings yet
- Case Investigation Form (CIF) - 2 PagesDocument2 pagesCase Investigation Form (CIF) - 2 PagesRexlee Alde LptNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Application For Non-Immigrant Visa: Foreign Service of The Philippines Philippine Consulate General, ChicagoDocument2 pagesApplication For Non-Immigrant Visa: Foreign Service of The Philippines Philippine Consulate General, ChicagoGrace Egbalic-AlumnoNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19) : Apply)Document4 pagesCase Investigation Form Coronavirus Disease (COVID-19) : Apply)handsam84No ratings yet
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- COVID 19 Form 1 1 PDFDocument1 pageCOVID 19 Form 1 1 PDFTuguinay EmilynNo ratings yet
- Travel Declaration and Contact Tracing Form For Guests HostelDocument2 pagesTravel Declaration and Contact Tracing Form For Guests HostelscribdNo ratings yet
- Asher Dan S. Dolina MD: Disease Surveillance Philippine Integrated and ResponseDocument5 pagesAsher Dan S. Dolina MD: Disease Surveillance Philippine Integrated and ResponseYoussry JaranillaNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesCase Investigation Form Coronavirus Disease (COVID-19)ILIGAN CJ Unit Welfare DevelopmentNo ratings yet
- DOT Health Declaration FormDocument1 pageDOT Health Declaration Formmark nielsen limNo ratings yet
- Opd Surveillance: Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesOpd Surveillance: Case Investigation Form Coronavirus Disease (COVID-19)kim aldonna muaNo ratings yet
- Philippine Integrated Disease Surveillance and Response: 14 DaysDocument1 pagePhilippine Integrated Disease Surveillance and Response: 14 DaysAlpha BatteryNo ratings yet
- Accident or Dangerous Incident Report FormDocument4 pagesAccident or Dangerous Incident Report FormFNo ratings yet
- Health Declaration Form of Dot Adopted by The Aquino Center For EventsDocument1 pageHealth Declaration Form of Dot Adopted by The Aquino Center For EventsLui SantosNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- Long-Stay Visa Application Form: French RepublicDocument3 pagesLong-Stay Visa Application Form: French RepublicFaye Isabelle SantiagoNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormcharleneNo ratings yet
- Covid 19 Cif Version 9 Sample BautistaDocument2 pagesCovid 19 Cif Version 9 Sample BautistaBautista MarizNo ratings yet
- Group Life Insurance Individual Application: ESP NEL and BelowDocument2 pagesGroup Life Insurance Individual Application: ESP NEL and BelowArianne Laydia100% (1)
- AEFI Reporting Form en Jan2016Document2 pagesAEFI Reporting Form en Jan2016madhuNo ratings yet
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaNo ratings yet
- KipiDocument1 pageKipiHeRha DAniarNo ratings yet
- Formulaire Ls Anglais PDFDocument2 pagesFormulaire Ls Anglais PDFgp_ph86No ratings yet
- Benford's Law: Applications for Forensic Accounting, Auditing, and Fraud DetectionFrom EverandBenford's Law: Applications for Forensic Accounting, Auditing, and Fraud DetectionRating: 3 out of 5 stars3/5 (1)
- The Science of Fingerprints: Classification and UsesFrom EverandThe Science of Fingerprints: Classification and UsesNo ratings yet
- Marvin - Resignation LetterDocument1 pageMarvin - Resignation LetterChum ChitaruNo ratings yet
- For Bahong Request of MedsDocument2 pagesFor Bahong Request of MedsChum ChitaruNo ratings yet
- Roving Clinic MedsDocument6 pagesRoving Clinic MedsChum ChitaruNo ratings yet
- Sworn Statement of Assets, Liabilities and Net WorthDocument2 pagesSworn Statement of Assets, Liabilities and Net WorthChum ChitaruNo ratings yet
- Ar NabelleDocument2 pagesAr NabelleChum ChitaruNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- Sign 0 1 2 Appearance Pulse GrimaceDocument2 pagesSign 0 1 2 Appearance Pulse GrimaceChum ChitaruNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- CDC IC Assessment Tool LTCFDocument14 pagesCDC IC Assessment Tool LTCFIsna Kencana ParamoreNo ratings yet
- BI SYNDROM - PPT 1 Theorie - De.enDocument31 pagesBI SYNDROM - PPT 1 Theorie - De.enSuhana hidayatNo ratings yet
- Responsible Use of Opioid in Indonesia: Highlight On OxycodoneDocument34 pagesResponsible Use of Opioid in Indonesia: Highlight On OxycodonearifwahyudiNo ratings yet
- Cholecystectomy Nursing Care PlanDocument1 pageCholecystectomy Nursing Care PlanJor Garcia100% (1)
- Did Alexander The Great Die From Guillain-Barré Syndrome - HallDocument26 pagesDid Alexander The Great Die From Guillain-Barré Syndrome - HallJAVIER AGUILAR CASASOLANo ratings yet
- Basic Life Support Training Manualnew PDFDocument88 pagesBasic Life Support Training Manualnew PDFkekoho4589100% (1)
- WR Tim Jaga 3Document285 pagesWR Tim Jaga 3VincentiusNo ratings yet
- Fonseca Et Al - 2017Document23 pagesFonseca Et Al - 2017TAINAH DE PAULANo ratings yet
- An Update On The New Investigations in Our ClinicDocument17 pagesAn Update On The New Investigations in Our ClinickhanasifalamNo ratings yet
- Anticipatory GrievingDocument2 pagesAnticipatory GrievingLeah Rebutiaco-Aguilar80% (5)
- Product Monograph - Zoledronic Acid For Injection ConcentrateDocument58 pagesProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaNo ratings yet
- Diagnosis of ADHD in AdultsDocument6 pagesDiagnosis of ADHD in Adultsdo lee100% (1)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Abortus Di Rsud Raden Mattaher Provinsi JambiDocument9 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Abortus Di Rsud Raden Mattaher Provinsi JambiIcha KristinaNo ratings yet
- Pelvic Physical Therapy For Chronic Pain and Dysfunction FollowinDocument13 pagesPelvic Physical Therapy For Chronic Pain and Dysfunction Followincode PVSNo ratings yet
- 3 Main Food Group: Reporter: Mercy Grace Yongco - MPA IDocument11 pages3 Main Food Group: Reporter: Mercy Grace Yongco - MPA ICHOSEN TABANASNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- Animalhealth Flyer Bovigam TB CO121138Document2 pagesAnimalhealth Flyer Bovigam TB CO121138PEACE TVNo ratings yet
- Table of Contents-AnoopDocument2 pagesTable of Contents-AnoopHernan JJNo ratings yet
- Imperforate AnusDocument24 pagesImperforate AnusGrace EspinoNo ratings yet
- Unit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraDocument17 pagesUnit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraZulkarnainNo ratings yet
- About Blood CellsDocument5 pagesAbout Blood CellsJoshua RaviNo ratings yet
- Anomalies of The Placenta and Cord 1Document52 pagesAnomalies of The Placenta and Cord 1Daniel Andre S. Somoray100% (1)
- Comparative Evaluation of Dry Eye Following Cataract Surgery: A Study From North IndiaDocument6 pagesComparative Evaluation of Dry Eye Following Cataract Surgery: A Study From North IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Inflammatory DermatologyDocument64 pagesInflammatory DermatologyDragonNo ratings yet
- Role of Dental AssistantsDocument11 pagesRole of Dental AssistantsJasmine Rey Quinto100% (1)
- Anello2019 PDFDocument2 pagesAnello2019 PDFandreiNo ratings yet
- Dress Syndrome A Review and UpdateDocument5 pagesDress Syndrome A Review and UpdateCarlos Alberto Torres LópezNo ratings yet
- Internalmedicine Sub AnsDocument90 pagesInternalmedicine Sub AnsSaneesh . SanthoshNo ratings yet
- Jan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonDocument3 pagesJan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonMarlon MejiaNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- Benguet GIDA ListDocument1 pageBenguet GIDA ListChum ChitaruNo ratings yet
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument4 pagesCoronavirus Disease (COVID-19) : Case Investigation FormMaria JoselaNo ratings yet
- Health Declaration Form DOT AmendedDocument1 pageHealth Declaration Form DOT AmendedImee S. YuNo ratings yet
- 101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinDocument17 pages101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinFilipeCarvalho100% (7)
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- New Cif FormDocument2 pagesNew Cif FormNovie FeneciosNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- Saric CifDocument1 pageSaric CifMarav SymbNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Health Declaration Form: Applicant ProfileDocument1 pageHealth Declaration Form: Applicant ProfileOnyx XynoNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Cif V9Document4 pagesCif V9SACH COVID 19 TASK FORCE SecretariatNo ratings yet
- Admitted in Multiple Health FacilitiesDocument5 pagesAdmitted in Multiple Health FacilitiesLemuel PetronioNo ratings yet
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesCase Investigation Form Coronavirus Disease (COVID-19)juwan decastroNo ratings yet
- Research Institute For Tropical Medicine: Admitted in Multiple Health FacilitiesDocument5 pagesResearch Institute For Tropical Medicine: Admitted in Multiple Health FacilitiesYescha FabitoNo ratings yet
- Youssry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Document5 pagesYoussry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Youssry JaranillaNo ratings yet
- CIF - Version 7wordDocument3 pagesCIF - Version 7wordBALIUAG DISTRICT LABORATORYNo ratings yet
- Chelsea L. Manalansan MD: Barangay Bulusan, Calapan City Oriental Mindoro 09634017938Document5 pagesChelsea L. Manalansan MD: Barangay Bulusan, Calapan City Oriental Mindoro 09634017938Youssry JaranillaNo ratings yet
- Case Investigation Form (CIF) - 2 PagesDocument2 pagesCase Investigation Form (CIF) - 2 PagesRexlee Alde LptNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Application For Non-Immigrant Visa: Foreign Service of The Philippines Philippine Consulate General, ChicagoDocument2 pagesApplication For Non-Immigrant Visa: Foreign Service of The Philippines Philippine Consulate General, ChicagoGrace Egbalic-AlumnoNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19) : Apply)Document4 pagesCase Investigation Form Coronavirus Disease (COVID-19) : Apply)handsam84No ratings yet
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- COVID 19 Form 1 1 PDFDocument1 pageCOVID 19 Form 1 1 PDFTuguinay EmilynNo ratings yet
- Travel Declaration and Contact Tracing Form For Guests HostelDocument2 pagesTravel Declaration and Contact Tracing Form For Guests HostelscribdNo ratings yet
- Asher Dan S. Dolina MD: Disease Surveillance Philippine Integrated and ResponseDocument5 pagesAsher Dan S. Dolina MD: Disease Surveillance Philippine Integrated and ResponseYoussry JaranillaNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesCase Investigation Form Coronavirus Disease (COVID-19)ILIGAN CJ Unit Welfare DevelopmentNo ratings yet
- DOT Health Declaration FormDocument1 pageDOT Health Declaration Formmark nielsen limNo ratings yet
- Opd Surveillance: Case Investigation Form Coronavirus Disease (COVID-19)Document3 pagesOpd Surveillance: Case Investigation Form Coronavirus Disease (COVID-19)kim aldonna muaNo ratings yet
- Philippine Integrated Disease Surveillance and Response: 14 DaysDocument1 pagePhilippine Integrated Disease Surveillance and Response: 14 DaysAlpha BatteryNo ratings yet
- Accident or Dangerous Incident Report FormDocument4 pagesAccident or Dangerous Incident Report FormFNo ratings yet
- Health Declaration Form of Dot Adopted by The Aquino Center For EventsDocument1 pageHealth Declaration Form of Dot Adopted by The Aquino Center For EventsLui SantosNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- Long-Stay Visa Application Form: French RepublicDocument3 pagesLong-Stay Visa Application Form: French RepublicFaye Isabelle SantiagoNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormcharleneNo ratings yet
- Covid 19 Cif Version 9 Sample BautistaDocument2 pagesCovid 19 Cif Version 9 Sample BautistaBautista MarizNo ratings yet
- Group Life Insurance Individual Application: ESP NEL and BelowDocument2 pagesGroup Life Insurance Individual Application: ESP NEL and BelowArianne Laydia100% (1)
- AEFI Reporting Form en Jan2016Document2 pagesAEFI Reporting Form en Jan2016madhuNo ratings yet
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaNo ratings yet
- KipiDocument1 pageKipiHeRha DAniarNo ratings yet
- Formulaire Ls Anglais PDFDocument2 pagesFormulaire Ls Anglais PDFgp_ph86No ratings yet
- Benford's Law: Applications for Forensic Accounting, Auditing, and Fraud DetectionFrom EverandBenford's Law: Applications for Forensic Accounting, Auditing, and Fraud DetectionRating: 3 out of 5 stars3/5 (1)
- The Science of Fingerprints: Classification and UsesFrom EverandThe Science of Fingerprints: Classification and UsesNo ratings yet
- Marvin - Resignation LetterDocument1 pageMarvin - Resignation LetterChum ChitaruNo ratings yet
- For Bahong Request of MedsDocument2 pagesFor Bahong Request of MedsChum ChitaruNo ratings yet
- Roving Clinic MedsDocument6 pagesRoving Clinic MedsChum ChitaruNo ratings yet
- Sworn Statement of Assets, Liabilities and Net WorthDocument2 pagesSworn Statement of Assets, Liabilities and Net WorthChum ChitaruNo ratings yet
- Ar NabelleDocument2 pagesAr NabelleChum ChitaruNo ratings yet
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Document6 pagesAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNo ratings yet
- Sign 0 1 2 Appearance Pulse GrimaceDocument2 pagesSign 0 1 2 Appearance Pulse GrimaceChum ChitaruNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- CDC IC Assessment Tool LTCFDocument14 pagesCDC IC Assessment Tool LTCFIsna Kencana ParamoreNo ratings yet
- BI SYNDROM - PPT 1 Theorie - De.enDocument31 pagesBI SYNDROM - PPT 1 Theorie - De.enSuhana hidayatNo ratings yet
- Responsible Use of Opioid in Indonesia: Highlight On OxycodoneDocument34 pagesResponsible Use of Opioid in Indonesia: Highlight On OxycodonearifwahyudiNo ratings yet
- Cholecystectomy Nursing Care PlanDocument1 pageCholecystectomy Nursing Care PlanJor Garcia100% (1)
- Did Alexander The Great Die From Guillain-Barré Syndrome - HallDocument26 pagesDid Alexander The Great Die From Guillain-Barré Syndrome - HallJAVIER AGUILAR CASASOLANo ratings yet
- Basic Life Support Training Manualnew PDFDocument88 pagesBasic Life Support Training Manualnew PDFkekoho4589100% (1)
- WR Tim Jaga 3Document285 pagesWR Tim Jaga 3VincentiusNo ratings yet
- Fonseca Et Al - 2017Document23 pagesFonseca Et Al - 2017TAINAH DE PAULANo ratings yet
- An Update On The New Investigations in Our ClinicDocument17 pagesAn Update On The New Investigations in Our ClinickhanasifalamNo ratings yet
- Anticipatory GrievingDocument2 pagesAnticipatory GrievingLeah Rebutiaco-Aguilar80% (5)
- Product Monograph - Zoledronic Acid For Injection ConcentrateDocument58 pagesProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaNo ratings yet
- Diagnosis of ADHD in AdultsDocument6 pagesDiagnosis of ADHD in Adultsdo lee100% (1)
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Abortus Di Rsud Raden Mattaher Provinsi JambiDocument9 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Abortus Di Rsud Raden Mattaher Provinsi JambiIcha KristinaNo ratings yet
- Pelvic Physical Therapy For Chronic Pain and Dysfunction FollowinDocument13 pagesPelvic Physical Therapy For Chronic Pain and Dysfunction Followincode PVSNo ratings yet
- 3 Main Food Group: Reporter: Mercy Grace Yongco - MPA IDocument11 pages3 Main Food Group: Reporter: Mercy Grace Yongco - MPA ICHOSEN TABANASNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- Animalhealth Flyer Bovigam TB CO121138Document2 pagesAnimalhealth Flyer Bovigam TB CO121138PEACE TVNo ratings yet
- Table of Contents-AnoopDocument2 pagesTable of Contents-AnoopHernan JJNo ratings yet
- Imperforate AnusDocument24 pagesImperforate AnusGrace EspinoNo ratings yet
- Unit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraDocument17 pagesUnit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraZulkarnainNo ratings yet
- About Blood CellsDocument5 pagesAbout Blood CellsJoshua RaviNo ratings yet
- Anomalies of The Placenta and Cord 1Document52 pagesAnomalies of The Placenta and Cord 1Daniel Andre S. Somoray100% (1)
- Comparative Evaluation of Dry Eye Following Cataract Surgery: A Study From North IndiaDocument6 pagesComparative Evaluation of Dry Eye Following Cataract Surgery: A Study From North IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Inflammatory DermatologyDocument64 pagesInflammatory DermatologyDragonNo ratings yet
- Role of Dental AssistantsDocument11 pagesRole of Dental AssistantsJasmine Rey Quinto100% (1)
- Anello2019 PDFDocument2 pagesAnello2019 PDFandreiNo ratings yet
- Dress Syndrome A Review and UpdateDocument5 pagesDress Syndrome A Review and UpdateCarlos Alberto Torres LópezNo ratings yet
- Internalmedicine Sub AnsDocument90 pagesInternalmedicine Sub AnsSaneesh . SanthoshNo ratings yet
- Jan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonDocument3 pagesJan 24 Skeletal Embryology and Limb Growth Stanmore Dr. Riego de Dios CPT TiongsonMarlon MejiaNo ratings yet