Download as pdf or txt
You might also like
- Electrical Certificate of Compliance and Electrical Safety CertificateDocument1 pageElectrical Certificate of Compliance and Electrical Safety CertificateAnonymous uwpXtHwLNo ratings yet
- How To Calculate An Intrinsically Safe Loop ApprovalDocument7 pagesHow To Calculate An Intrinsically Safe Loop ApprovalAlexander Ariza Nadjar100% (1)
- Airbus ESLD ECAM System Logic DataDocument3,736 pagesAirbus ESLD ECAM System Logic Datapontoo100% (2)
- Biomedical Instrumentation (BM8502)Document34 pagesBiomedical Instrumentation (BM8502)1011 BMENo ratings yet
- Ec 8073 - Medical Electronics Unit - I Electro - Phisiology and Bio Potential RecordingDocument9 pagesEc 8073 - Medical Electronics Unit - I Electro - Phisiology and Bio Potential RecordingJackie SparrowNo ratings yet
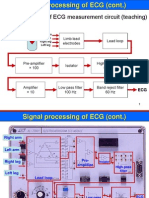
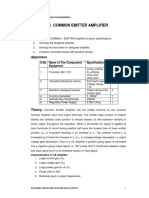
- Lecture 5 (13.3.2024) - ECG CircuitDocument22 pagesLecture 5 (13.3.2024) - ECG CircuitJihad Al-NajjarNo ratings yet
- Waleed Abdel Aziz Salem Attia - ECG (L1-L2-L3)Document57 pagesWaleed Abdel Aziz Salem Attia - ECG (L1-L2-L3)Mandy745No ratings yet
- Unit III Signal Conditioning CircuitsDocument15 pagesUnit III Signal Conditioning CircuitsAleeshaNo ratings yet
- ECG With ImageDocument7 pagesECG With ImagemathavanNo ratings yet
- Electrodes - Limb Electrodes - Floating Electrodes - Pregelled Disposable Electrodes - Micro, Needle and Surface ElectrodesDocument33 pagesElectrodes - Limb Electrodes - Floating Electrodes - Pregelled Disposable Electrodes - Micro, Needle and Surface ElectrodesBarani DharanNo ratings yet
- 203 MDE ECG2 LectuersDocument8 pages203 MDE ECG2 LectuersBhaskar BelavadiNo ratings yet
- SaikatDocument50 pagesSaikatSaurabh MondalNo ratings yet
- 01 2018 BMI - Biopotential Amplifiers PDFDocument52 pages01 2018 BMI - Biopotential Amplifiers PDFviki mikiNo ratings yet
- Biomedical Instrumentation: Biopotential AmplifiersDocument52 pagesBiomedical Instrumentation: Biopotential Amplifiersviki mikiNo ratings yet
- ECG and XRAYDocument47 pagesECG and XRAYSwaroop KumarNo ratings yet
- Instrumentationamplifier ECGDocument35 pagesInstrumentationamplifier ECGRoiNo ratings yet
- Omd551/Basics of Biomedical Instrumentation Two Marks With Answer Unit I Bio Potential Generation and Electrodes TypesDocument13 pagesOmd551/Basics of Biomedical Instrumentation Two Marks With Answer Unit I Bio Potential Generation and Electrodes TypesAleesha100% (1)
- Biopot. Amp 1Document17 pagesBiopot. Amp 1etome05No ratings yet
- Biopotential AmplifiersDocument94 pagesBiopotential AmplifiersAhmed Magdy HassanNo ratings yet
- Unit-3 Notes PDFDocument16 pagesUnit-3 Notes PDF03 Anton P JacksonNo ratings yet
- Characteristics of Blood FlowDocument11 pagesCharacteristics of Blood FlowPriyamvada VermaNo ratings yet
- By: Gebremariam Fisseha Adigrat University, Ethiopia 2010E.CDocument21 pagesBy: Gebremariam Fisseha Adigrat University, Ethiopia 2010E.CmillionNo ratings yet
- Biopotential Amplifiers: Operational Amplifier Differential Amplifier Instrumentation AmplifierDocument28 pagesBiopotential Amplifiers: Operational Amplifier Differential Amplifier Instrumentation AmplifierEZHIL NNo ratings yet
- Biomedical Engineering Theory and Practice-Biomedical Instrumentation-ElectrocardiographyDocument4 pagesBiomedical Engineering Theory and Practice-Biomedical Instrumentation-Electrocardiographyvicky_ani1986No ratings yet
- Lecture-2 Bioelectric Amplifiers and Measuring InstrumentsDocument29 pagesLecture-2 Bioelectric Amplifiers and Measuring InstrumentsHundessa DabaNo ratings yet
- Some RandomDocument57 pagesSome RandomPratham TapadiaNo ratings yet
- Activity 4Document9 pagesActivity 4Lucille YuNo ratings yet
- Pre-Lab Assignment: Read and Review Sections 2.4, 2.8.2, 9.9.3, 13.4, 13.5, and 13.9 inDocument11 pagesPre-Lab Assignment: Read and Review Sections 2.4, 2.8.2, 9.9.3, 13.4, 13.5, and 13.9 inThe_Dude1138No ratings yet
- Design Considerations For Ecg Systems Hann Apr2010 Compatibility ModeDocument87 pagesDesign Considerations For Ecg Systems Hann Apr2010 Compatibility ModeJeffrey MarshallNo ratings yet
- Bio Intrumentation Lab 01Document10 pagesBio Intrumentation Lab 01roroy43581No ratings yet
- A Precision Low-Level DAS/ECG Cardiotachometer Demo BoardDocument43 pagesA Precision Low-Level DAS/ECG Cardiotachometer Demo BoardEddy Santiago Neira SisaNo ratings yet
- Unit - 1 PDFDocument39 pagesUnit - 1 PDFLouie Lucero DomingoNo ratings yet
- Un Mundo Feliz - Aldous HuxleyDocument43 pagesUn Mundo Feliz - Aldous HuxleyAlbertanoNo ratings yet
- SBM1301Document84 pagesSBM1301g8248418302No ratings yet
- Electrocardiogram (ECG) Circuit: InstructablesDocument10 pagesElectrocardiogram (ECG) Circuit: InstructablesDulanjalee KatulandaNo ratings yet
- Capacitor ESR MeterDocument2 pagesCapacitor ESR MeterMarkoNo ratings yet
- Lab 3Document5 pagesLab 3Ricardo VelazquezNo ratings yet
- 03 - Biosignal CharacteristicsDocument46 pages03 - Biosignal CharacteristicsdarNo ratings yet
- Electroni C Projects: Low-Voltage AC VoltmeterDocument2 pagesElectroni C Projects: Low-Voltage AC VoltmeterpestaNo ratings yet
- Be 3600 Biomedical Instrumentation (Lab) - : Experiment 4Document5 pagesBe 3600 Biomedical Instrumentation (Lab) - : Experiment 4Abhay GuptaNo ratings yet
- 6-ECG Circuit-PreparedDocument29 pages6-ECG Circuit-PreparedFarhanNo ratings yet
- Ecg CircuitDocument12 pagesEcg CircuitAbdullah AfifiNo ratings yet
- AmplifierDocument13 pagesAmplifierShafiq MohammadNo ratings yet
- ECG Circuit PDFDocument6 pagesECG Circuit PDFarduino signaux cardiaquesNo ratings yet
- Unit - I Electrical - BeeeDocument27 pagesUnit - I Electrical - BeeeBubblee BennuNo ratings yet
- ECG Circuit Analysis and Design Engineers LabsDocument29 pagesECG Circuit Analysis and Design Engineers LabsDebasish HalderNo ratings yet
- Design ECG AmplifierDocument9 pagesDesign ECG Amplifierm_wssNo ratings yet
- ELEC4810 Notes-4 PDFDocument27 pagesELEC4810 Notes-4 PDFKwan ChanNo ratings yet
- Biomedicak Instrumentation LabDocument56 pagesBiomedicak Instrumentation LabMD. ASHIQUR RAHMAN 1602111No ratings yet
- Fundamentals of Substation ProtectionDocument113 pagesFundamentals of Substation Protectionmaynard pacala100% (1)
- EmtDocument115 pagesEmtRaj SharmaNo ratings yet
- Lecture 1b Electrical Safety CH 14Document18 pagesLecture 1b Electrical Safety CH 14api-27535945No ratings yet
- 3264.TI ECG Fundamentals Condensed v08 PDFDocument105 pages3264.TI ECG Fundamentals Condensed v08 PDFAshish BeheraNo ratings yet
- Ecd Manuals 1-7Document46 pagesEcd Manuals 1-7Muhammad Hozaifa100% (1)
- Conference Proceeding NTAFM 2013Document3 pagesConference Proceeding NTAFM 2013atifthestarNo ratings yet
- ECG Design ConsiderationDocument3 pagesECG Design ConsiderationBridget ThomasNo ratings yet
- 1.2.3.A.SIM ElectricalCircuits1Document10 pages1.2.3.A.SIM ElectricalCircuits1patrick mNo ratings yet
- Lec 1 - Introduction To BiopotentialsDocument30 pagesLec 1 - Introduction To BiopotentialsAbdallah MahmoudNo ratings yet
- To Demonstrate Electrical Symbols and Electrical Measuring InstrumentsDocument4 pagesTo Demonstrate Electrical Symbols and Electrical Measuring InstrumentsFaaiz QamarNo ratings yet
- Reference Guide To Useful Electronic Circuits And Circuit Design Techniques - Part 2From EverandReference Guide To Useful Electronic Circuits And Circuit Design Techniques - Part 2No ratings yet
- Reference Guide To Useful Electronic Circuits And Circuit Design Techniques - Part 1From EverandReference Guide To Useful Electronic Circuits And Circuit Design Techniques - Part 1Rating: 2.5 out of 5 stars2.5/5 (3)
- Layout of 33kV Daram Khola HPP Feeder at Receiving End Substation (Harichaur Substation)Document1 pageLayout of 33kV Daram Khola HPP Feeder at Receiving End Substation (Harichaur Substation)KrishnaChhusyakiNo ratings yet
- Sanyo Eco-I Central Address SettingDocument2 pagesSanyo Eco-I Central Address SettingJacek NawrotNo ratings yet
- 2b - NMR For Oil Gas Prospecting PDFDocument10 pages2b - NMR For Oil Gas Prospecting PDFGheorghe Alexandru GabrielNo ratings yet
- Kaneka Brochure GEBDocument4 pagesKaneka Brochure GEBSolarShop AustraliaNo ratings yet
- A Handbook of Coaxial Microwave MeasurementsDocument169 pagesA Handbook of Coaxial Microwave Measurementspravin maliNo ratings yet
- Angular GripperDocument12 pagesAngular GripperAman RajNo ratings yet
- Linksys RE6500 (Ingles)Document11 pagesLinksys RE6500 (Ingles)Victor GomezNo ratings yet
- Switchmatic Switchmatic 2: Advanced SettingsDocument6 pagesSwitchmatic Switchmatic 2: Advanced SettingsHay ThemNo ratings yet
- Wireless LANDocument19 pagesWireless LANManishNo ratings yet
- R D A 6 2 3 1 D A T A S H e e TDocument11 pagesR D A 6 2 3 1 D A T A S H e e Trendra zeeNo ratings yet
- 056-054 DSE8x10 in Fixed Export (Base Load)Document4 pages056-054 DSE8x10 in Fixed Export (Base Load)hariana100% (1)
- Win Easunlock SuiteDocument23 pagesWin Easunlock SuiteMarc MorrisonNo ratings yet
- HPX Xuv SpecsDocument1 pageHPX Xuv SpecspravinkumarkrNo ratings yet
- Ackermann Clino System99Document121 pagesAckermann Clino System99Syed Rahmath AliNo ratings yet
- Magnetrol 45-115 PDFDocument28 pagesMagnetrol 45-115 PDFdonjazonNo ratings yet
- Frequency Selective Surface: A Modernized Efficient Way of Filtering in Microwave FieldDocument82 pagesFrequency Selective Surface: A Modernized Efficient Way of Filtering in Microwave FieldRiyanSahaNo ratings yet
- Cordless TelephonesDocument23 pagesCordless TelephonesVishal Kumar ShawNo ratings yet
- Conthermo Warming ChamberDocument4 pagesConthermo Warming ChamberArstNo ratings yet
- W 48 × H 48 MM Power ON Delay Analog Timers: ATE8 SeriesDocument3 pagesW 48 × H 48 MM Power ON Delay Analog Timers: ATE8 Seriesyanier martinezNo ratings yet
- Abdullah Computer AcessoriesDocument4 pagesAbdullah Computer AcessoriesAbdullah QasimNo ratings yet
- Polarization Interferometer For Measuring Small DisplacementDocument4 pagesPolarization Interferometer For Measuring Small Displacementchung phamNo ratings yet
- Tesmec Se 1250 frb615 en Rev00Document1 pageTesmec Se 1250 frb615 en Rev00myn maliQueNo ratings yet
- Tps 92512Document30 pagesTps 92512ppanagosNo ratings yet
- Hailei-186KWh Rack Open High Voltage ESS Solution-A0Document15 pagesHailei-186KWh Rack Open High Voltage ESS Solution-A0Alex TarasovetsNo ratings yet
- Gamma Correction - TV Problems and Repair SolutionsDocument4 pagesGamma Correction - TV Problems and Repair SolutionsNsb El-kathiriNo ratings yet
- CERAFILTEC Product Data Sheet - Tower-RackDocument1 pageCERAFILTEC Product Data Sheet - Tower-Rackxxxx222xxxxNo ratings yet
- Aspire T120: User's ManualDocument20 pagesAspire T120: User's ManualvladamarkoNo ratings yet