Download as pdf or txt
You might also like
- Carbon180 - A Review of Global and U.S. Total Available Markets For CarbontechDocument11 pagesCarbon180 - A Review of Global and U.S. Total Available Markets For CarbontechTito JankowskiNo ratings yet
- GU Moisture Analyzer enDocument44 pagesGU Moisture Analyzer enLalo RuizNo ratings yet
- 26 Manuals 3338, Anti-Aircraft Ammunition PDFDocument129 pages26 Manuals 3338, Anti-Aircraft Ammunition PDFKosta_g100% (1)
- Coroas Systematic ReviewDocument10 pagesCoroas Systematic ReviewEstaf EmkeyzNo ratings yet
- PuneDocument25 pagesPuneVarun JaiswarNo ratings yet
- De Sousa APBR - in Vitro Tooth Reattachment Technique PDFDocument23 pagesDe Sousa APBR - in Vitro Tooth Reattachment Technique PDFPatricia JesikaNo ratings yet
- A Comparative Evaluation of Masticatory Ef Ciency and Satisfaction With Different Types of Removable Partial Dentures: A Pilot Crossover Randomized StudyDocument6 pagesA Comparative Evaluation of Masticatory Ef Ciency and Satisfaction With Different Types of Removable Partial Dentures: A Pilot Crossover Randomized StudyBOHR International Journal of Current research in Dentistry (BIJCRID)No ratings yet
- Dentist Material Selection For Single-Unit Crowns (2016)Document8 pagesDentist Material Selection For Single-Unit Crowns (2016)JohnNo ratings yet
- The Quality of Denture Influencing Oral-Health-Related Quality of Life in Complete Denture Wearing Older Adults: A Systematic ReviewDocument10 pagesThe Quality of Denture Influencing Oral-Health-Related Quality of Life in Complete Denture Wearing Older Adults: A Systematic Reviewgentdolf5No ratings yet
- IDJ Vol 7 1Document6 pagesIDJ Vol 7 1Saatvik AtriNo ratings yet
- International Journal of Dental Science and Innovative Research (IJDSIR)Document7 pagesInternational Journal of Dental Science and Innovative Research (IJDSIR)yusfaNo ratings yet
- 20abhinav Thesis Article Part 2Document6 pages20abhinav Thesis Article Part 2bhupendraNo ratings yet
- CD005512 AbstractDocument4 pagesCD005512 Abstractkomal nanavatiNo ratings yet
- Orthodonticanchorage AsystematicreviewDocument10 pagesOrthodonticanchorage AsystematicreviewDrAkash VermaNo ratings yet
- Self-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The IOTNDocument7 pagesSelf-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The IOTNyolaNo ratings yet
- Gingival, Oral Hygiene and Periodontal Status of The Teeth Restored With Stainless Steel Crown: A Prospective StudyDocument6 pagesGingival, Oral Hygiene and Periodontal Status of The Teeth Restored With Stainless Steel Crown: A Prospective StudyRoxana OneaNo ratings yet
- Restorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresDocument18 pagesRestorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresRayhan DaneoNo ratings yet
- ArticleDocument17 pagesArticleUjNo ratings yet
- Endocrowns A Systematic ReviewDocument17 pagesEndocrowns A Systematic Reviewaulia lubisNo ratings yet
- Limited Evidence Suggests Benefits of Single Visit Revascularization Endodontic Procedures - A Systematic ReviewDocument9 pagesLimited Evidence Suggests Benefits of Single Visit Revascularization Endodontic Procedures - A Systematic ReviewMARIA NAENo ratings yet
- Orthodonticanchorage AsystematicreviewDocument10 pagesOrthodonticanchorage AsystematicreviewMohammed ijasNo ratings yet
- Bookshelf NBK304706 PDFDocument20 pagesBookshelf NBK304706 PDFAnrico Boy RiansyamNo ratings yet
- Self-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The IotnDocument7 pagesSelf-Perception of Malocclusion Among Nigerian Adolescents Using The Aesthetic Component of The Iotnamalia rieska mauliddyaNo ratings yet
- Accepted Manuscript: Journal of DentistryDocument21 pagesAccepted Manuscript: Journal of DentistryLuis Alberto Carpio MorenoNo ratings yet
- RR 18 Pandu SSCDocument6 pagesRR 18 Pandu SSCPandu UtamiNo ratings yet
- DR Neha ArticleDocument7 pagesDR Neha ArticleVinod ViswanathanNo ratings yet
- Research Methodology in Dentistry: Part I - The Essentials and Relevance of ResearchDocument8 pagesResearch Methodology in Dentistry: Part I - The Essentials and Relevance of ResearchRomNo ratings yet
- Deo GadeDocument8 pagesDeo GadeFebe GracewithaNo ratings yet
- BP RestorativedentDocument14 pagesBP RestorativedentKhan MustafaNo ratings yet
- Bookshelf NBK401552Document24 pagesBookshelf NBK401552Hanina mamiNo ratings yet
- Treatment Concepts For Restorations of Endodontically Treated TeethDocument8 pagesTreatment Concepts For Restorations of Endodontically Treated TeethAliaNo ratings yet
- CRISConceptnoteDocument5 pagesCRISConceptnoteaka88No ratings yet
- Cephalometric Norms For Mewari Children Using Steiner's AnalysisDocument6 pagesCephalometric Norms For Mewari Children Using Steiner's AnalysisDenis KimNo ratings yet
- Measuring Children's Dental Anxiety: Oral Cancer /paediatric DentistryDocument2 pagesMeasuring Children's Dental Anxiety: Oral Cancer /paediatric DentistryManda JoanNo ratings yet
- Australian Dental Journal - 2011 - Lewis - Prosthodontic Considerations Designed To Optimize Outcomes For Single ToothDocument12 pagesAustralian Dental Journal - 2011 - Lewis - Prosthodontic Considerations Designed To Optimize Outcomes For Single ToothOumaima DabbouNo ratings yet
- Articulo 12Document9 pagesArticulo 12lyes BrionesNo ratings yet
- Ijdr 201721 07Document4 pagesIjdr 201721 07jdmaneNo ratings yet
- Assessment of Oral Hygiene Practices Dentition Status and Treatment Needs of Institutionalized Elderly Living in Geriatric Homes of Dakshina Kannada District Karnataka IndiaDocument6 pagesAssessment of Oral Hygiene Practices Dentition Status and Treatment Needs of Institutionalized Elderly Living in Geriatric Homes of Dakshina Kannada District Karnataka IndiaAthenaeum Scientific PublishersNo ratings yet
- Success Criteria For Dental Implant - A Literature Review: Research ArticleDocument5 pagesSuccess Criteria For Dental Implant - A Literature Review: Research Articlehimanshu vadherNo ratings yet
- 3583-Article Text-6597-1-10-20210423Document8 pages3583-Article Text-6597-1-10-20210423Gitika SinghNo ratings yet
- TL3 8 Garbim2021Document33 pagesTL3 8 Garbim2021bomonnhacongdongNo ratings yet
- Nano 1Document8 pagesNano 1jennifertaniaNo ratings yet
- Quality Assessment of Systematic Reviews On Alveolar Socket Preservation.Document9 pagesQuality Assessment of Systematic Reviews On Alveolar Socket Preservation.andreita_loppNo ratings yet
- JPharmBioallSci12514-1547558 0417551Document7 pagesJPharmBioallSci12514-1547558 0417551Mary SmileNo ratings yet
- DentalimplantinchildrenDocument14 pagesDentalimplantinchildrenVinay MuppanaNo ratings yet
- A Scoping Review On Design Modifications of Lingual Holing Arch ApplianceDocument6 pagesA Scoping Review On Design Modifications of Lingual Holing Arch ApplianceSaumya SinghNo ratings yet
- Assessment of Knowledge, Attitude and Practices Regarding Bioethics Among Students in Dental Institutes of PunjabDocument7 pagesAssessment of Knowledge, Attitude and Practices Regarding Bioethics Among Students in Dental Institutes of PunjabIJAR JOURNALNo ratings yet
- JIndianSocPedodPrevDent362198-2600776 071327 PDFDocument8 pagesJIndianSocPedodPrevDent362198-2600776 071327 PDFayano23No ratings yet
- 2016 Article 320Document8 pages2016 Article 320Milena RamirezNo ratings yet
- Prosthodontics and Implant DentistryDocument9 pagesProsthodontics and Implant DentistryCaroline AngoneseNo ratings yet
- Irrigantes IntracanalDocument14 pagesIrrigantes Intracanaljhon valdiviezoNo ratings yet
- Dental Implant and Aesthetics A Systematic ReviewDocument7 pagesDental Implant and Aesthetics A Systematic Reviewabdulaziz alzaidNo ratings yet
- Clinical Oral Implants Res - 2018 - Morton - Group 2 ITI Consensus Report Prosthodontics and Implant DentistryDocument9 pagesClinical Oral Implants Res - 2018 - Morton - Group 2 ITI Consensus Report Prosthodontics and Implant DentistryTao LinksNo ratings yet
- Jcpe 12078Document12 pagesJcpe 12078SitiKhadijahNo ratings yet
- Laser DopplerDocument10 pagesLaser Dopplerodontoedu66No ratings yet
- Jurnal Ortho 5Document6 pagesJurnal Ortho 5Santika IndahsariNo ratings yet
- Pediatric Dentists' Choices of Restorative Materials For Primary MolarsDocument5 pagesPediatric Dentists' Choices of Restorative Materials For Primary MolarsdermagaNo ratings yet
- Applications of Research Methodology in Oral and Maxillofacial SurgeryDocument15 pagesApplications of Research Methodology in Oral and Maxillofacial SurgeryRomNo ratings yet
- BJBMS 20 13Document8 pagesBJBMS 20 13yessicalopezodontologiaNo ratings yet
- Group 2 ITI Consensus Report Prosthodontics and Implant DentistryDocument9 pagesGroup 2 ITI Consensus Report Prosthodontics and Implant Dentistry6mp57dy74sNo ratings yet
- Assessment of in Vivo Bond Strength Studies of The Orthodontic Bracket Adhesive System: A Systematic ReviewDocument10 pagesAssessment of in Vivo Bond Strength Studies of The Orthodontic Bracket Adhesive System: A Systematic ReviewNoNo ratings yet
- Long-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewDocument10 pagesLong-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewArcelino FariasNo ratings yet
- An Introduction to Clinical Research for Health and Social Care ProfessionalsFrom EverandAn Introduction to Clinical Research for Health and Social Care ProfessionalsNo ratings yet
- Prescribing Dental Radiographs For Infants, Children, Adolescents, and Individuals With Special Health Care NeedsDocument4 pagesPrescribing Dental Radiographs For Infants, Children, Adolescents, and Individuals With Special Health Care Needsnona aryanNo ratings yet
- BP RecordkeepingDocument8 pagesBP Recordkeepingnona aryanNo ratings yet
- E Iadt-IntroDocument5 pagesE Iadt-Intronona aryanNo ratings yet
- Management of Dental Patients With Special Health Care NeedsDocument8 pagesManagement of Dental Patients With Special Health Care Needsnona aryanNo ratings yet
- Evidence-Based Clinical Practice Guideline For The Use of Pit-and-Fissure SealantsDocument17 pagesEvidence-Based Clinical Practice Guideline For The Use of Pit-and-Fissure Sealantsnona aryanNo ratings yet
- OS Single Tooth ExtractionDocument9 pagesOS Single Tooth Extractionnona aryanNo ratings yet
- Acquired Temporomandibular Disorders in Infants, Children, and AdolescentsDocument9 pagesAcquired Temporomandibular Disorders in Infants, Children, and Adolescentsnona aryanNo ratings yet
- Open SectionsDocument142 pagesOpen Sectionsnona aryanNo ratings yet
- Overall Grading Components Critical Assessment Paper 40 % Online Quizzes 10% Laboratory Simulation Project 20% Final Exam 30%Document123 pagesOverall Grading Components Critical Assessment Paper 40 % Online Quizzes 10% Laboratory Simulation Project 20% Final Exam 30%nona aryanNo ratings yet
- Eating DisordersDocument3 pagesEating Disordersnona aryanNo ratings yet
- Quiz 1: Interarch Distance (When There Is An Opposing Tooth) Should Be Minimum - Mm. in The Anterior Sites and 1Document2 pagesQuiz 1: Interarch Distance (When There Is An Opposing Tooth) Should Be Minimum - Mm. in The Anterior Sites and 1nona aryanNo ratings yet
- Management Considerations For Pediatric Oral Surgery and Oral PathologyDocument11 pagesManagement Considerations For Pediatric Oral Surgery and Oral Pathologynona aryanNo ratings yet
- Preparing For Your Child's Sedation VisitDocument2 pagesPreparing For Your Child's Sedation Visitnona aryanNo ratings yet
- Use of Antibiotic Therapy For Pediatric Dental Patients: Latest RevisionDocument4 pagesUse of Antibiotic Therapy For Pediatric Dental Patients: Latest Revisionnona aryanNo ratings yet
- Pain Management in Infants, Children, Adolescents, and Individuals With Special Health Care NeedsDocument9 pagesPain Management in Infants, Children, Adolescents, and Individuals With Special Health Care Needsnona aryanNo ratings yet
- BP ChildabuseDocument6 pagesBP Childabusenona aryanNo ratings yet
- BP ClassperiodiseasesDocument15 pagesBP Classperiodiseasesnona aryan100% (1)
- Caries-Risk Assessment and Management For Infants, Children, and AdolescentsDocument6 pagesCaries-Risk Assessment and Management For Infants, Children, and Adolescentsnona aryanNo ratings yet
- Adolescent Oral Health Care: Latest RevisionDocument10 pagesAdolescent Oral Health Care: Latest Revisionnona aryanNo ratings yet
- BP AnesthesiapersonnelDocument5 pagesBP Anesthesiapersonnelnona aryanNo ratings yet
- Use of Protective Stabilization For Pediatric Dental PatientsDocument7 pagesUse of Protective Stabilization For Pediatric Dental Patientsnona aryanNo ratings yet
- R MedhistoryformDocument3 pagesR Medhistoryformnona aryanNo ratings yet
- Common Laboratory Values: Test Normal Value Function SignificanceDocument1 pageCommon Laboratory Values: Test Normal Value Function Significancenona aryanNo ratings yet
- EJ1045976Document8 pagesEJ1045976nona aryanNo ratings yet
- Policy On Tobacco Use: Latest RevisionDocument5 pagesPolicy On Tobacco Use: Latest Revisionnona aryanNo ratings yet
- Sedation Record: Patient Selection Criteria DateDocument2 pagesSedation Record: Patient Selection Criteria Datenona aryanNo ratings yet
- Policy On Use of Xylitol in Pediatric Dentistry: Latest RevisionDocument2 pagesPolicy On Use of Xylitol in Pediatric Dentistry: Latest Revisionnona aryanNo ratings yet
- Chapter 13Document31 pagesChapter 13DrakzNo ratings yet
- Aashto M145-91Document5 pagesAashto M145-91KkNo ratings yet
- Woodcraft Construction Kit Product CatalogueDocument35 pagesWoodcraft Construction Kit Product CatalogueBoban Svemogući ĐokićNo ratings yet
- Ben Senouci Douidi: Certificate of AchievementDocument2 pagesBen Senouci Douidi: Certificate of AchievementDakota624No ratings yet
- Sem - Ii Pharmacology Lab ManualDocument36 pagesSem - Ii Pharmacology Lab ManualLokesh MahataNo ratings yet
- Susten DS For WebDocument1 pageSusten DS For WebkinamedeboNo ratings yet
- Mapping Kemuning 1 - 2 Maret 2023Document1 pageMapping Kemuning 1 - 2 Maret 2023josephNo ratings yet
- Pile Capacity Calculation in Accordance With IS-2911: As Per Geotech Report As Per Geotech Report As Per Geotech ReportDocument4 pagesPile Capacity Calculation in Accordance With IS-2911: As Per Geotech Report As Per Geotech Report As Per Geotech ReportShuja ShowkatNo ratings yet
- Aemr-Unit 1-Piston EngineDocument85 pagesAemr-Unit 1-Piston Engineuthira100% (1)
- Words of PleasureDocument211 pagesWords of PleasureallendraNo ratings yet
- RLO CableDocument1 pageRLO CableLeiden O'SullivanNo ratings yet
- Preconception Counselling PDFDocument4 pagesPreconception Counselling PDFponekNo ratings yet
- Lista de Exercicios Reported Speech 786250Document3 pagesLista de Exercicios Reported Speech 786250Ricardo SazaNo ratings yet
- Topic 8 Cell Respiration and PhotosynthesisDocument12 pagesTopic 8 Cell Respiration and PhotosynthesisCedric Williams100% (1)
- Reviewer PurComm Communications and BarriersDocument5 pagesReviewer PurComm Communications and BarriersMhavs CasimiroNo ratings yet
- Amm 320 Novo-1Document23 pagesAmm 320 Novo-1gabriel eugen staminNo ratings yet
- Design of Material Handling System For SpecificDocument14 pagesDesign of Material Handling System For SpecificKaran Virbhadre100% (3)
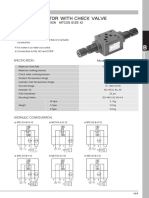
- MTC 03 W Throttle Check ValveDocument4 pagesMTC 03 W Throttle Check Valve박준용No ratings yet
- Olive Oil InfrastructuresDocument5 pagesOlive Oil InfrastructuresShahzad ShameemNo ratings yet
- Parasitology For DummiesDocument8 pagesParasitology For DummiesimranNo ratings yet
- The Potential of 3D Printing To Reduce The Environmental Impacts of ProductionDocument9 pagesThe Potential of 3D Printing To Reduce The Environmental Impacts of ProductionAlexi WiedemannNo ratings yet
- Concept of Disaster Risk Reduction and ManagementDocument2 pagesConcept of Disaster Risk Reduction and ManagementPrincess BalquinNo ratings yet
- SonicFill Handpiece Instructions For UseDocument58 pagesSonicFill Handpiece Instructions For UseZulfahmi NurdinNo ratings yet
- Where Does The Glycolysis OccourDocument2 pagesWhere Does The Glycolysis OccourMaria Claudette Andres AggasidNo ratings yet
- Cranial Nerves Rule of 4Document3 pagesCranial Nerves Rule of 4ashr9No ratings yet
- 4 Central Venous Pressure MonitoringDocument1 page4 Central Venous Pressure MonitoringCAROLYN BORDONNo ratings yet
- EMPM5103-PQMP Assignment - Part BDocument60 pagesEMPM5103-PQMP Assignment - Part Bnorizam32100% (2)