Download as pdf or txt
You might also like
- ICO Exams. E-Source.2019 PDFDocument11 pagesICO Exams. E-Source.2019 PDFHussain SyedNo ratings yet
- Cardio 1Document11 pagesCardio 1Raluca Andreea AxinteNo ratings yet
- Bio Marker 1Document11 pagesBio Marker 1Raluca Andreea AxinteNo ratings yet
- JBC 22 497Document25 pagesJBC 22 497rasika bhatNo ratings yet
- Trackpdf10.1186s13054 020 03025 y PDFDocument4 pagesTrackpdf10.1186s13054 020 03025 y PDFNeda PiratvisuthNo ratings yet
- VEGF Expression in Colorectal Cancer Metastatic LyDocument14 pagesVEGF Expression in Colorectal Cancer Metastatic LyNana LianaNo ratings yet
- BMM 13 5Document7 pagesBMM 13 5zeravoneNo ratings yet
- Clinical Biochemistry: SciencedirectDocument4 pagesClinical Biochemistry: Sciencedirectfaraz.mirza1No ratings yet
- Prognostic Impact of The Advanced Lung Cancer Inflammation Index (ALI) in Metastatic Non-Small Cell Lung Cancer Treated With First Line ChemotherapyDocument32 pagesPrognostic Impact of The Advanced Lung Cancer Inflammation Index (ALI) in Metastatic Non-Small Cell Lung Cancer Treated With First Line Chemotherapyagustiawan28No ratings yet
- 68 406 1 PBDocument6 pages68 406 1 PBidhaNo ratings yet
- GC Sepsis Apr 28 2013Document31 pagesGC Sepsis Apr 28 2013Elys ElzNo ratings yet
- Treatment of Onychomycosis - A Clinical Study: Original PaperDocument4 pagesTreatment of Onychomycosis - A Clinical Study: Original PaperMagna Fitriani HutasuhutNo ratings yet
- Ignatiadis 2021Document16 pagesIgnatiadis 2021Igor VasićNo ratings yet
- Overcoming Treatment Challenges in Patients With Newly Diagnosed AMLDocument34 pagesOvercoming Treatment Challenges in Patients With Newly Diagnosed AMLsaldanhasmithaNo ratings yet
- 1.3. Biomarker Resti 19102019 Revisi 2Document33 pages1.3. Biomarker Resti 19102019 Revisi 2indriNo ratings yet
- Utilitatea Protein Coronei in TNBCDocument19 pagesUtilitatea Protein Coronei in TNBCRadu AndreiNo ratings yet
- Vincent J 2020Document11 pagesVincent J 2020Kala PatharNo ratings yet
- Expression Profiling of Metastatic Renal Cell Carcinoma Using Gene Set Enrichment AnalysisDocument6 pagesExpression Profiling of Metastatic Renal Cell Carcinoma Using Gene Set Enrichment AnalysisPradnya GNo ratings yet
- Clinica Chimica Acta: Martina Zaninotto, Monica Maria Mion, Chiara Cosma, Daniela Rinaldi, Mario Plebani TDocument3 pagesClinica Chimica Acta: Martina Zaninotto, Monica Maria Mion, Chiara Cosma, Daniela Rinaldi, Mario Plebani TWilliams Alejandro Choroco VillegasNo ratings yet
- Biomarkers Identifying Sepsis Phenotypes PDFDocument42 pagesBiomarkers Identifying Sepsis Phenotypes PDFjenaro heli Ardila CortesNo ratings yet
- Association Between Exposure Characteristics and The Risk For COVID-19 Infection Among Health Care Workers With and Without BNT162b2 VaccinationDocument4 pagesAssociation Between Exposure Characteristics and The Risk For COVID-19 Infection Among Health Care Workers With and Without BNT162b2 VaccinationChristian GaraffaNo ratings yet
- RX PDFDocument3 pagesRX PDFMASIEL AMELIA BARRANTES ARCENo ratings yet
- Overexpression of Mesothelin in Pancreatic Ductal Adenocarcinoma (PDAC)Document6 pagesOverexpression of Mesothelin in Pancreatic Ductal Adenocarcinoma (PDAC)Belia Bima NafisaNo ratings yet
- Pedersen Et Al., 2016 - BS PredictorsDocument8 pagesPedersen Et Al., 2016 - BS PredictorsJulia SCNo ratings yet
- Antibiotics: Clinical Findings and Antimicrobial Susceptibility of Anaerobic Bacteria Isolated in Bloodstream InfectionsDocument9 pagesAntibiotics: Clinical Findings and Antimicrobial Susceptibility of Anaerobic Bacteria Isolated in Bloodstream Infectionstsiko111No ratings yet
- Ctbeb MS Id 555558Document3 pagesCtbeb MS Id 555558lathifatulNo ratings yet
- Ersoz Et Al. Factors Afeecting Mortality in Fournier Gangrene Axperince With Fiftytwo PatientsDocument4 pagesErsoz Et Al. Factors Afeecting Mortality in Fournier Gangrene Axperince With Fiftytwo PatientsFHNo ratings yet
- Utilidad Biomarcadores en Manejo de Infeccion. Quimioter 2018Document4 pagesUtilidad Biomarcadores en Manejo de Infeccion. Quimioter 2018Liz HerreraNo ratings yet
- Panc Adenocarcinoma Recent Data and Perspective JR Delpero HPB Course 2022 V4-NuoveDocument176 pagesPanc Adenocarcinoma Recent Data and Perspective JR Delpero HPB Course 2022 V4-NuoveDiana MitreaNo ratings yet
- Wood-2016-Cytometry Part B: Clinical CytometryDocument7 pagesWood-2016-Cytometry Part B: Clinical CytometryWalter Jhon Delgadillo AroneNo ratings yet
- 274359-The Effect of Colchicine Administration On HSCRP LevelDocument6 pages274359-The Effect of Colchicine Administration On HSCRP Levelagung_safthonyNo ratings yet
- The Search For New Cardiovascular Biomarkers: Robert E. Gerszten & Thomas J. WangDocument4 pagesThe Search For New Cardiovascular Biomarkers: Robert E. Gerszten & Thomas J. WangJOUBERT ALVAREZNo ratings yet
- ClinikalDocument8 pagesClinikalnadaNo ratings yet
- Contribution of Systematic Serological Testing inDocument6 pagesContribution of Systematic Serological Testing inMuhammad Rifqi FakhriNo ratings yet
- RequestedDocument9 pagesRequestedGaurav MauryaNo ratings yet
- Arulkumaran 2020Document8 pagesArulkumaran 2020jose torresNo ratings yet
- Prevention Agnelli 3Document1 pagePrevention Agnelli 3s3lki3No ratings yet
- Asymptomatic COVID-19 Patients at A COVID Designated Asymptomatic COVID-19 Patients at A COVID Designated Hospital in Nepal Hospital in NepalDocument7 pagesAsymptomatic COVID-19 Patients at A COVID Designated Asymptomatic COVID-19 Patients at A COVID Designated Hospital in Nepal Hospital in NepalJudelle Enriquez-GazaNo ratings yet
- Which One in TheDocument5 pagesWhich One in TheEnvhy AmaliaNo ratings yet
- Wjarr 2024 1058Document7 pagesWjarr 2024 1058mcvallespinNo ratings yet
- Articulo EndocarditisDocument10 pagesArticulo EndocarditisAliss ReyesNo ratings yet
- Biomarker SepsisDocument18 pagesBiomarker SepsisSukma EffendyNo ratings yet
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDocument2 pagesProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNo ratings yet
- Correlation Between MIB-1 and Other ProliferationDocument9 pagesCorrelation Between MIB-1 and Other Proliferation1832303aNo ratings yet
- Journal Pmed 1003501Document28 pagesJournal Pmed 1003501Abi HinojosaNo ratings yet
- Cholangiocarcinoma Landscape in Europe - Diagnostic, Prognosis and Therapeutic Insights From The ENSCCA RegistryDocument14 pagesCholangiocarcinoma Landscape in Europe - Diagnostic, Prognosis and Therapeutic Insights From The ENSCCA RegistryAnna MariaNo ratings yet
- Research ArticleDocument5 pagesResearch ArticleRAFAELNo ratings yet
- Ceftaroline Jesus VallejosDocument6 pagesCeftaroline Jesus VallejosDiego VasquezNo ratings yet
- Salivary Biomarkers and Their Application in The Diagnosis and Monitoring of The Most Common Oral PathologiesDocument17 pagesSalivary Biomarkers and Their Application in The Diagnosis and Monitoring of The Most Common Oral PathologiesLU LAM THIENNo ratings yet
- Early Breast Cancer Prognostic Options Including CanAssistDocument49 pagesEarly Breast Cancer Prognostic Options Including CanAssistIndranil GhoshNo ratings yet
- PCR y PCTDocument12 pagesPCR y PCTRicardo PazNo ratings yet
- Extrapulmonary Manifestations of COVID-19: Nature Medicine July 2020Document17 pagesExtrapulmonary Manifestations of COVID-19: Nature Medicine July 2020Stefano Alvarez MatosNo ratings yet
- 2017 Article 233Document8 pages2017 Article 233Alfeus GradyNo ratings yet
- The Causes of Postoperative Meningitis The Comparison of Gram-Negative and Gram-Positive PathogensDocument8 pagesThe Causes of Postoperative Meningitis The Comparison of Gram-Negative and Gram-Positive PathogensPietroRossidisNo ratings yet
- Indications and Short-Term Outcome of Major Lower Extremity Amputations in Khartoum Teaching HospitalDocument8 pagesIndications and Short-Term Outcome of Major Lower Extremity Amputations in Khartoum Teaching Hospitaljean vargasNo ratings yet
- Introduction To Molecular DiagnosticsDocument19 pagesIntroduction To Molecular DiagnosticsJulian BarreraNo ratings yet
- Imaging Features and Differences Among The Three Primary Malignant Non-Wilms Tumors in ChildrenDocument9 pagesImaging Features and Differences Among The Three Primary Malignant Non-Wilms Tumors in ChildrenEMIRZA NUR WICAKSONONo ratings yet
- Procalcitonin Is It The End of Road To Sepsis Diagnosis - February - 2022 - 6546541022 - 2629943Document2 pagesProcalcitonin Is It The End of Road To Sepsis Diagnosis - February - 2022 - 6546541022 - 2629943RateeshNo ratings yet
- Levels of Procalcitonin in The Patients of SepsisDocument7 pagesLevels of Procalcitonin in The Patients of SepsisIJAR JOURNALNo ratings yet
- Advances in The Field of Nanooncology: Review Open AccessDocument11 pagesAdvances in The Field of Nanooncology: Review Open AccessscrabzNo ratings yet
- Biomarkers in Cancer Therapy: Liquid Biopsy Comes of AgeFrom EverandBiomarkers in Cancer Therapy: Liquid Biopsy Comes of AgeHideaki ShimadaNo ratings yet
- @anesthesia Books 2016 Oxford TextbookDocument1,016 pages@anesthesia Books 2016 Oxford TextbookAnny VelásquezNo ratings yet
- Policy Name: Membership No.: Particulars: Bupa 408651001 Slfe 17707077Document1 pagePolicy Name: Membership No.: Particulars: Bupa 408651001 Slfe 17707077Saber ElkassasNo ratings yet
- PPDDocument2 pagesPPDMaheen KalwarNo ratings yet
- Prescribing in ChildrenDocument4 pagesPrescribing in ChildrenArkopal GuptaNo ratings yet
- Authorization To Walk HomeDocument50 pagesAuthorization To Walk HomeAidan FranciscoNo ratings yet
- Principles and Examples of Design of Rehabilitation Centers in Russia and AbroadDocument6 pagesPrinciples and Examples of Design of Rehabilitation Centers in Russia and Abroadkratika gargNo ratings yet
- NCP GDMDocument2 pagesNCP GDMboomNo ratings yet
- NURS FPX 6210 Assessment 3 Strategic Visioning With StakeholdersDocument7 pagesNURS FPX 6210 Assessment 3 Strategic Visioning With Stakeholdersjoohnsmith070No ratings yet
- NP 3Document5 pagesNP 3Annelore ArcayNo ratings yet
- Dispelling The Malaria-Typhoid Co-Infection Myth in Nigeria. A Literature ReviewDocument8 pagesDispelling The Malaria-Typhoid Co-Infection Myth in Nigeria. A Literature Reviewwaleola25No ratings yet
- Hosp Study MMH2Document26 pagesHosp Study MMH2Bhell MendiolaNo ratings yet
- Hipnosis Con NiñosDocument17 pagesHipnosis Con NiñosAlberto Estrada0% (2)
- Spironolactone Hydrochlorothiazide OralDocument1 pageSpironolactone Hydrochlorothiazide Oraljinzo88No ratings yet
- Samantha Wiederkehr ResumeDocument1 pageSamantha Wiederkehr Resumeapi-520841770No ratings yet
- Summary of Movement DisordersDocument21 pagesSummary of Movement DisordersSamyukthaBalabhadraNo ratings yet
- Blood TransfusionDocument48 pagesBlood TransfusionJhade RelletaNo ratings yet
- Laporan Penggunaan Obat Rasional (Diagnosa: Ispa)Document8 pagesLaporan Penggunaan Obat Rasional (Diagnosa: Ispa)SessyNo ratings yet
- Psoriasis OSCEDocument2 pagesPsoriasis OSCEKatherynSotoNo ratings yet
- Alex Hardin Resume 2015Document3 pagesAlex Hardin Resume 2015api-306883462No ratings yet
- Social & Preventive Pharmacy (Thakur Publication) - 1Document218 pagesSocial & Preventive Pharmacy (Thakur Publication) - 1Manav Patel100% (1)
- NURS FPX 5003 Assessment 4 Executive Summary - Community Health AssessmentDocument5 pagesNURS FPX 5003 Assessment 4 Executive Summary - Community Health Assessmentjoohnsmith070No ratings yet
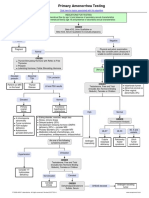
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- How Farmers Can Prevent and Treat Ringworm in CattleDocument3 pagesHow Farmers Can Prevent and Treat Ringworm in CattlepsmanasseNo ratings yet
- Homeopathy: 1 HistoryDocument32 pagesHomeopathy: 1 HistoryslowdogNo ratings yet
- UCLA Mobile Eye Clinic 2019 Needs AssessmentDocument1 pageUCLA Mobile Eye Clinic 2019 Needs AssessmentUMEC Young Professionals InitiativeNo ratings yet
- MetforminDocument2 pagesMetforminEdem LeeNo ratings yet
- EAP FormDocument2 pagesEAP FormRebecca LuiNo ratings yet
- Pediatrictone Management: Sathya Vadivelu,, Anne Stratton,, Wendy PierceDocument10 pagesPediatrictone Management: Sathya Vadivelu,, Anne Stratton,, Wendy PierceDeborah SalinasNo ratings yet
- Case Analysis SchizophreniaDocument2 pagesCase Analysis Schizophreniamark OrpillaNo ratings yet